
Abstract
It has been proposed that women who have a negative colposcopic examination or who have no cervical intraepithelial neoplasia (CIN) on colposcopic biopsy can be safely returned to routine screening with the next visit being three or five years later. We present data regarding 551 women who had colposcopy in Wales for a low-grade cytological abnormality and who were followed through Cervical Screening Wales for subsequent CIN. Of 436 women declared CIN free initially, 26 (6.0%) had high-grade CIN diagnosed on follow-up. We suggest that additional screening at an interval of less than three years should be offered to women with a negative colposcopy or a biopsy without CIN.
We conducted a randomized controlled trial in women with borderline changes or mild dyskaryosis on cervical cytology within Cervical Screening Wales (CSW). Recruitment took place between October 2004 and December 2007. All women were offered colposcopy between four and 12 months after randomization. Examinations were performed by BSCCP accredited colposcopists practicing within the NHS. Using the CSW Programme database, we identified further cytology and histology results taken outside of the trial up to March 2009. Of 551 women who had an initial colposcopy (Figure 1), 436 had negative colposcopy (or negative biopsy). A total of 94 women were found to have CIN2+ either at initial colposcopy (n = 54) or during follow-up (n = 40). Of these, 26 (27.7%) were in women with negative initial colposcopy/biopsy and 14 (14.9%) with CIN 1 initially. Women with a negative initial colposcopy or a biopsy showing less than CIN1 had a non-negligible risk of subsequent high-grade disease with 25/392 (6.4%) women diagnosed with CIN2+ between nine and 36 months following the initial negative colposcopy. (Additionally, one woman, aged 44 years, had a diagnosis of CIN3 more than 36 months after the negative colposcopy.)
CONSORT diagram showing the results of follow-up of 551 women who had a baseline colposcopic examination within the study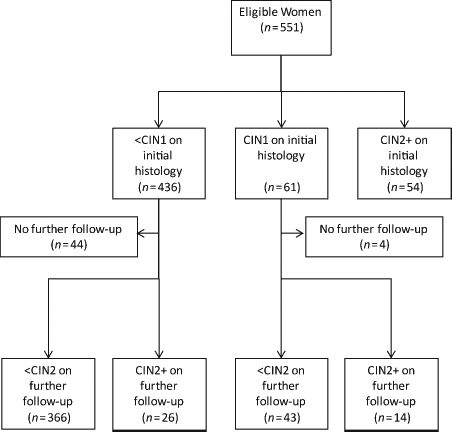
National policy should not be based only on results from centres with a specialist interest in colposcopy, but needs to be safe for every BSCCP accredited colposcopist. For women referred to colposcopy based on abnormal screening results it seems unlikely that a single negative colposcopy is sufficient to provide reassurance against concurrent CIN2 + or by extension the development of cervical cancer over the next three years. Although we support the introduction of HPV triage into the NHS Cervical Screening Programme we suggest it is necessary to provide additional screening at an interval of less than three years for women with a negative colposcopy or a biopsy showing less than CIN1.