
Abstract
Ductus venosus blood flow, expressed as a pulsatility index (DVPI) has been shown to improve the performance of the Combined and Integrated antenatal screening tests for Down's syndrome using previously published data. The use of ductus venosus blood flow as a categorical marker (reversed or absent end diastolic blood flow indicating a positive result) is less discriminatory but simpler, so is sometimes preferred over DVPI. For example, with the Integrated test the false-positive rate for a 90% detection rate was 1.5% as a categorical marker compared with 1.1% expressed as DVPI. We here provide the necessary algorithm and parameters for using ductus venosus blood flow as a categorical marker with the Combined and Integrated tests.
The use of ductus venosus blood flow, expressed as a pulsatility index (DVPI; the difference between the maximum blood velocity in systole and that at the end of diastole [A-wave] in the ductus venosus divided by the maximum velocity averaged over the time of one heartbeat) has been shown to improve the performance of antenatal screening tests for Down's syndrome. At a 90% detection rate (DR) the inclusion of DVPI reduced the false-positive rate (FPR) of the late first trimester Combined test from 8.5% to 4.6% and the FPR of the late first and early second trimester Integrated test from 2.0% to 1.1%. 1
The use of ductus venosus blood flow as a categorical marker (reverse or absent end diastolic blood flow indicating a positive test result, and forward flow a negative result) is less discriminatory than DVPI (for example, at a 90% DR, including ductus venosus as a categorical marker with the Integrated test yielded a 1.5% FPR compared with a 1.1% FPR including DVPI, and with the Combined test yielded a 6.1% FPR compared with a 4.6% FPR). Nevertheless, some screening groups have asked us to provide an algorithm for estimating the risk of a pregnancy being affected with Down's syndrome in which ductus venosus is incorporated as a categorical marker. We therefore here, using data reported by Borrell et al., 1 provide the necessary algorithm.
The direction or absence of end diastolic blood flow in the ductus venosus was recorded in 49 of the 66 Down's syndrome and 4896 of the 7184 unaffected pregnancies that formed the basis of the previous analysis.
1
Blood flow was reversed in 41% of affected and 2.5% of unaffected pregnancies, and absent in 8.2% affected and 0.35% of unaffected pregnancies. Using logistic regression in affected and unaffected pregnancies separately, reversed or absent ductus venosus blood flow was found to be dependent on nuchal translucency (NT) measurement (P = 0.016 and P < 0.001 respectively). This analysis yielded the following equations:
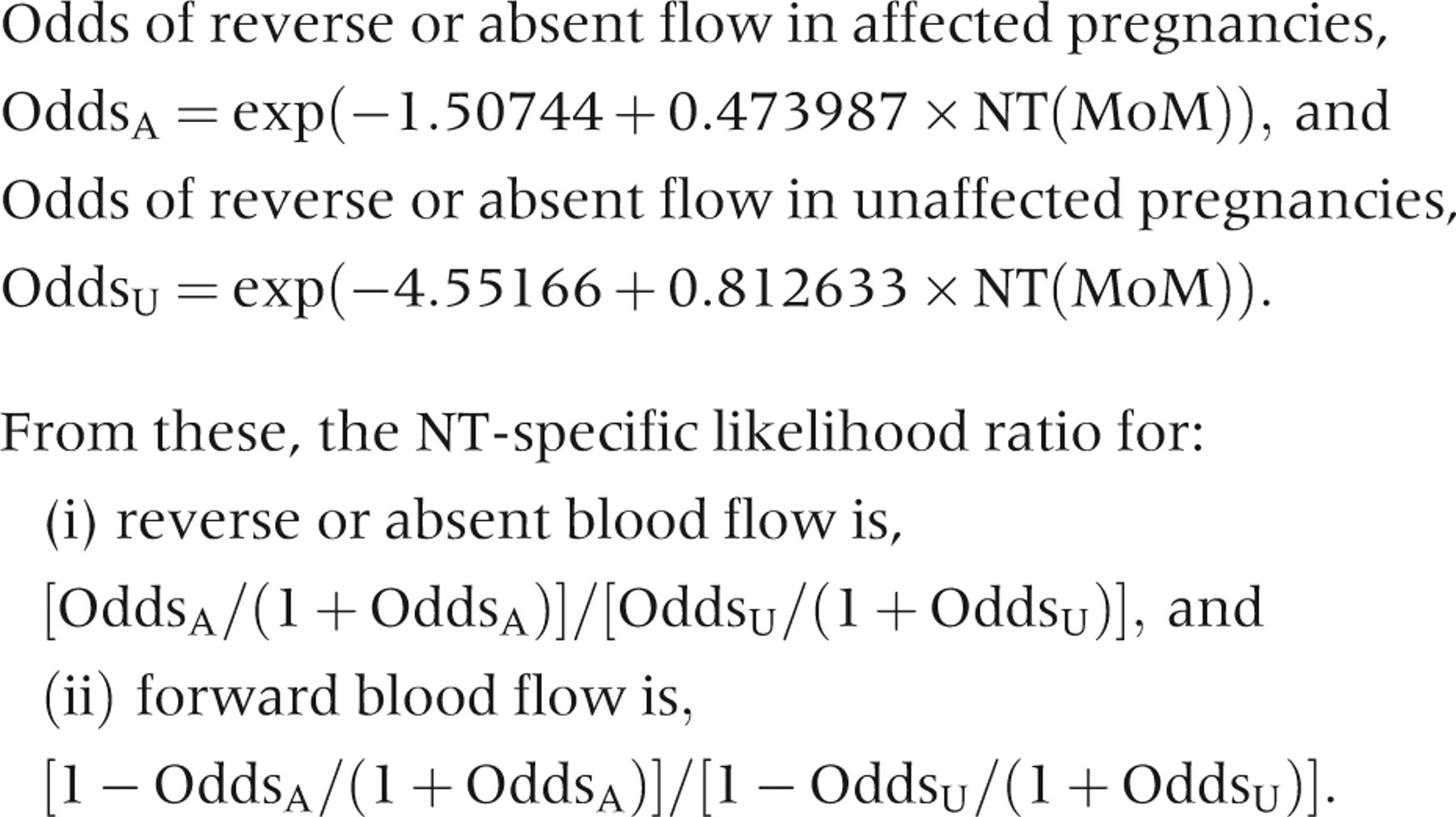
For example, if a woman had a pregnancy with an NT value of 2.0 MoM, then the odds of reverse or absent ductus venosus blood flow if her pregnancy is affected is exp(−1.50744 + 0.473987 × 2) = 0.57, and if her pregnancy is unaffected is exp(−4.55166 + 0.812633 × 2) = 0.05. If blood flow through the ductus venosus is reversed, then her likelihood ratio is (0.57/1.57)/(0.05/1.05) = 7.6. If her Combined test likelihood ratio is 5, then the likelihood ratio including ductus venosus is 7.6 × 5 = 38. If her maternal age-related risk of an affected pregnancy is 1:500 then her final risk is 1:13.
If an NT measurement is not possible then the likelihood ratios can be calculated directly from the proportion of affected and unaffected pregnancies with reverse of absent blood flow described above, so that for reverse or absent blood flow the likelihood ratio is (41 + 8.2)/(2.5 + 0.35) = 49.2/2.85 = 17, and for forward blood flow the likelihood ratio is (100−49.2)/(100−2.85) = 0.52.
Disclosure of interests
N Wald has a patent for the Integrated test. With others, he holds a patent in connection with the use of uE3 as a second trimester screening marker in prenatal screening for Down's syndrome. He is Director of Logical Medical Systems Ltd, which produces software for the interpretation of Down's syndrome screening tests.