
Abstract
Objective
To compare the health-related quality-of-life (HRQoL) of children with screening-detected coeliac disease (CD), before they learned of their diagnosis, with that of children without CD and in those previously diagnosed with CD.
Methods
In a cross-sectional CD screening study (‘ETICS’: Exploring the Iceberg of Coeliacs in Sweden), of 10,041 Swedish 12-year-olds invited, 7567 (75%) consented to participate, and 7208 (72%) children without previously diagnosed CD had serological markers analysed. Before the screening results were known, 7218 children (72%) and 6524 of their parents (65%) answered questionnaires. Questionnaires included the Swedish child-friendly pilot version of the EQ-5D instrument and proxy version of the EQ-5D instrument, which are generic tools used to describe HRQoL.
Results
We found no significant difference in HRQoL between the groups of children with screening-detected CD, without CD, and those previously diagnosed with CD.
Conclusion
The HRQoL reported by 12-year-olds with screening-detected CD, before they learned of their diagnosis, was not worse than that of the children without CD or those previously diagnosed with CD. Thus, mass screening for CD should not be justified on the basis that children with unrecognized CD have a poor HRQoL. However, because these children rated their HRQoL before diagnosis and treatment, they may not have recognized or perceived symptoms as severe enough to seek medical attention which demonstrates how difficult clinical/active case finding can be. Mass screening may still, therefore, be considered if the aim is early detection and prevention of future complications.
Introduction
The generally suggested prevalence of CD is around 1%, 2 however, many cases of CD are undiagnosed.2–5 People with unrecognized CD have enteropathy, but the health and health-related quality of life (HRQoL) 6 they experience is not fully understood.1,2,7–10
Mass screening may be an option for identifying hidden cases, 3 however, because screening is offered to people who have not sought medical attention on account of the disorder for which screening is conducted, those who are detected should benefit from diagnosis and treatment and the screening should minimize harm and maximize benefit.11,12 Based on the recommendations of Wilson and Jungner, 13 adapted by the World Health Organisation, 14 CD screening could be an appropriate public health intervention because it is fairly common, early detection through general clinical practice is often difficult, untreated the negative health consequences are extensive, reliable screening tools are widespread, and an effective treatment is available. 3 Nevertheless, screening for CD is still controversial,1,3,8,15,16 and more information is needed about long-term consequences of untreated CD and the HRQoL of screening-detected CD cases.1,3,16
Few studies have investigated HRQoL at the actual time of CD screening, before diagnosis.17,18 To our knowledge this is the only study where children (not chosen from high-risk groups) were asked about their HRQoL before receiving the results of the screening. The aim of the study was to determine the HRQoL of children with screening-detected CD before they learned of their diagnosis, and compare it with children without CD and those previously diagnosed with CD.
Methods
Study Design
A cross-sectional CD screening study, ‘ETICS’, Exploring the Iceberg of Coeliacs in Sweden, involved a birth cohort born during the Swedish CD epidemic.5,19 The study took place in 2005–2006, when the children were about 12 years old. It involved five regions in Sweden and included local schools and paediatric departments. 5
Subjects
In total, 10,041 children in the sixth grade were invited to participate, 7567 (75%) agreed to participate, and blood samples were collected from 7208 (72%) children without previously diagnosed CD. 5 Children with suspected CD were referred to the closest paediatric department for a small intestine biopsy, and for those with a confirmed diagnosis, follow-up care was provided according to current clinical standards. 5 Ultimately, 153 cases of screening-detected CD and 66 previously diagnosed CD cases were confirmed, for a total prevalence of 3%.5,20
For this study we classified three groups according to CD status: 1) screening-detected CD children, 2) previously diagnosed CD children, and 3) non-CD children.
Questionnaires
Questionnaires were given to children and their parents after blood samples were taken, but before they were aware of screening results. The child questionnaires were completed in school and the parent questionnaire, along with a pre-addressed and postage-paid envelope, were sent home to be completed by the parents. Questionnaires were collected from 7218 children (3490 girls and 3728 boys) and 6524 parents.
The questionnaires included the EQ-5D instrument which is a generic tool used to measure health status and report on HRQoL. 21 It consists of two parts, the EQ-5D descriptive system where health status is classified in five dimensions: mobility, self-care, usual activities, pain/discomfort, anxiety/depression and on three levels of severity (no problems, moderate problems or severe problems) and the VAS, a thermometer-like visual analogue scale, where respondents score their health today from worst to best imaginable (0–100). 21
The EQ-5D instrument has recently been developed and tested for use in younger age groups.22–25 In the present study, the child questionnaire included the Swedish child-friendly pilot version of the EQ-5D instrument, where the child-friendly headings of the five dimensions are: mobility, looking after myself, doing usual activities, having pain or discomfort and feeling worried or sad, and the severity levels are no problems, some problems and a lot of problems.24,25 The parent questionnaire included a standard proxy version of the EQ-5D adult version, which asked parents how they would rate their child's health. 21
Analysis
We dichotomized EQ-5D levels of severity into ‘no problems’ from those reporting no problems and ‘problems’ combining those reporting moderate or severe problems (some or a lot of problems on the child-friendly version).24–26 Cross tabulations and statistical tests were performed using the statistical software package SPSS 17 (SPSS Inc., Chicago, IL). To test statistical significance of the difference between those who reported no problems and problems within the groups we used Fisher's exact test. For the asymmetrical VAS data we conducted a non-parametric independent samples median test across the groups for child and parent responses and an independent samples Mann-Whitney U test to compare girls’ and boys’ responses. Spearman's rho test was used to explore the correlation between children's and parents’ VAS scores. VAS scores are presented with median values and 25th and 75th percentiles. 26 Statistical significance was defined at the 5% level. Adjustment for other variables was not done as there were no statistically significant differences across groups and further exploration would have been difficult due to the small number in the screening-detected and previous CD groups.
Responses were included for children (and their parents) who had: 1) elevated CD serological markers and a biopsy proven diagnosis, 2) their previous CD diagnosis confirmed by the national CD register and/or medical records, or 3) normal CD serological markers. The EQ-5D descriptive system and VAS responses were included even if the respondent had only completed one of these parts. Some did not answer all dimensions; however, responses were included for each dimension reported on even if the respondent had not completed all dimensions. For these reasons, the response numbers vary between the instruments and the dimensions.
Results
Of the 7218 children who returned questionnaires, 98% (n = 7052–7071, depending on dimension) met inclusion requirements and reported on at least one dimension from the descriptive system and 98% (n = 7051) responded to the VAS. Of the 6524 parents who returned questionnaires, 98–99% (n = 6388–6443, depending on dimension) met inclusion requirements and reported on at least one dimension on the descriptive system and 97% (n = 6298) responded to the VAS.
Eq-5D Dimensions
Children and parents were in general agreement and most reported no problems in all dimensions. However, in the dimensions having pain or discomfort and feeling worried or sad the percentage reporting problems, from each group, was higher than for the other dimensions (Table 1).
Based on the children's responses, no significant differences in the dimensions across the three groups were found (Table 1). However, screening-detected CD children more often reported problems in the dimensions mobility (4%), doing usual activities (3%), having pain or discomfort (22%) and feeling worried or sad (14%). The exception was in the dimension looking after myself, in which 2% of previously CD-diagnosed children reported problems. In the dimension having pain or discomfort there was a larger gap between groups, as 15% of previously diagnosed CD children reported problems, while 22% of screening-detected CD and 20% of non-CD children reported problems (Table 1).
Among the parent responses, no significant differences in the dimensions were found across the three groups (Table 1). A greater percentage of parents with children with screening-detected CD reported problems (3%) in usual activities. Like the children, the group most often reporting problems in the dimension self-care (2%) was the parents of previously diagnosed CD children. Parents of non-CD children most often reported problems in the anxiety/depression dimension (15%). In the dimension pain/discomfort, 18% of the parents of children previously diagnosed with CD and 18% of the parents of non-CD children reported problems. In the dimension mobility, 1% of both the parents of children with screening-detected CD and the parents of non-CD children reported problems (Table 1).
Children and parents reporting no problems and problems, by EQ-5D dimensions and across groups, before the children's screening-detected coeliac disease diagnosis
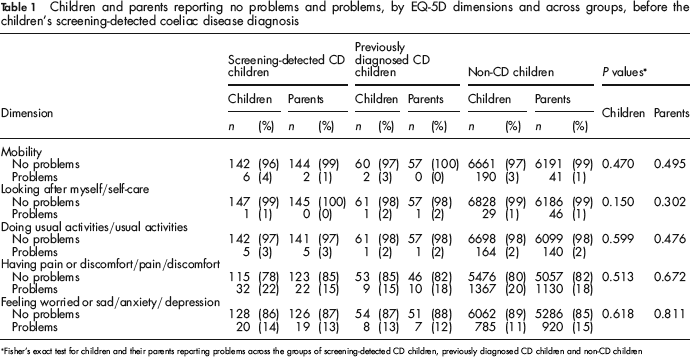
Fisher's exact test for children and their parents reporting problems across the groups of screening-detected CD children, previously diagnosed CD children and non-CD children
When comparing girls across the three groups and boys across the three groups, we only found a difference in the percentage reporting problems for the boys in the dimension doing usual activities (Fisher's exact test, P = 0.035) (Table 2). When girls were compared with boys, we found that within the non-CD group, more girls than boys reported problems in the dimensions having pain or discomfort (22% compared with 18%, Fisher's exact test, P = 0.001), and feeling worried or sad (16% compared with 7%, Fisher's exact test, P = 0.000). Boys in the screening-detected group reported more problems with doing usual activities than girls (7% compared with 0%, Fisher's exact test, P = 0.020).
Girls and boys reporting no problems and problems, by EQ-5D dimensions and across groups, before their screening-detected coeliac disease diagnosis
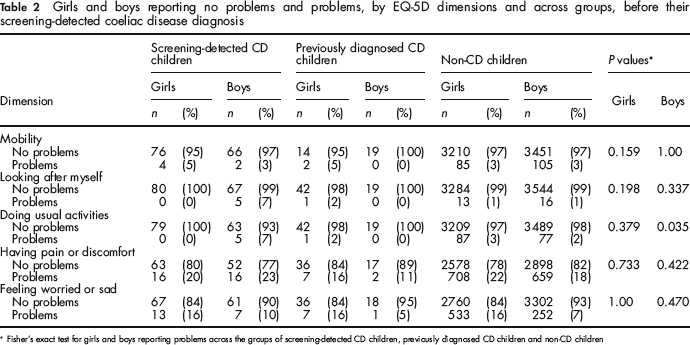
Fisher's exact test for girls and boys reporting problems across the groups of screening-detected CD children, previously diagnosed CD children and non-CD children
Based on the EQ-5D dimensions, the children and their parents showed general agreement. We found a significant difference in parents’ overall reports in the dimensions usual activity and pain/discomfort with respect to the sex of their child. The parents more often reported problems in the dimension usual activity if their child was a boy (3% compared with 2%, Fisher's exact test, P = 0.001) and in the dimension pain/discomfort if their child was a girl (20% compared with 17%, Fisher's exact test, P = 0.013).
Vas
There was no difference in VAS scores across groups for either children or parents. The median VAS score in each group for the children was 90, and for parents it was 95 (Table 3). The correlation between child and parent VAS scores was low and statistically significant (Spearman's rho 0.237, P = 0.001) (Table 3).
Children's and parents’ VAS scores across groups before the children's screening-detected coeliac disease diagnosis

There was a statistically significant difference in the children's VAS scores related to sex. In the non-CD group, which also represents the overall group results, girls reported worse health than boys, with a median score of 90 compared with 93 (independent samples Mann-Whitney U test, P = 0.001) (Table 4).
Girls’ and boys’ VAS scores across groups before their screening-detected celiac disease diagnosis
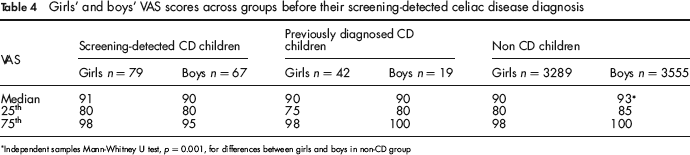
Independent samples Mann-Whitney U test, p = 0.001, for differences between girls and boys in non-CD group
Discussion
We found no significant difference in HRQoL between the groups of children with unrecognized CD, without CD, and those previously diagnosed with CD. This suggests that HRQoL, reported before diagnosis, is not worse for children with unrecognized CD compared with their peers. Our results capture the children's HRQoL before they knew of their diagnosis. Perhaps the children were truly asymptomatic and had similar HRQoL to their peers. On the other hand, someone with unrecognized CD may have mild or diffuse symptoms they do not recognize, ignore or adapt to, and therefore consider their HRQoL as optimal.8,18
Studies concerned with HRQoL for people with CD have typically focused on adults.27–32 However, a few studies have explored the HRQoL of children and adolescents with CD. In a sample of children and adolescents from a Dutch CD society, the HRQoL for those who were clinically diagnosed and treated was similar to that of the healthy controls, although the adolescent girls with CD reported more physical complaints than the adolescent boys with CD. 33 In a case-control study, Wagner et al. 34 investigated German and Austrian adolescents, invited from CD societies, who retrospectively reported on quality-of-life. They compared adolescents who were diagnosed with CD and initiated treatment early (before six years of age) and late (after six years of age) and found that those with a late diagnosis reported poorer quality-of-life in the areas of school, physical health and CD-associated burden compared with those who received an early diagnosis. 34 In contrast, a Scottish study by Solaymani-Dodaran et al. 35 found an increased long-term mortality risk in adults diagnosed with CD in childhood compared with those diagnosed as adults. However, these results may be related to external causes resulting from behavioural changes associated with CD and the treatment.1,35
Studies have also explored the HRQoL of people with screening-detected CD compared with clinically diagnosed patients18,36 and/or the general population,17,18 however, the focus has often been on physical or clinical symptoms.37–39 We found only a few studies that describe the HRQoL of screening-detected CD individuals (not from high-risk populations) from the time of screening, before the diagnosis was confirmed.17,18 In one of these studies, Van Koppen et al. 17 described a 10-year follow-up of screened Dutch children, aged 2–4 years at diagnosis. Before screening, parents of children who had symptoms and were later diagnosed with CD reported a lower HRQoL in their children than the parents of the healthy reference population, but the HRQoL of the symptom-free children, who were later diagnosed with CD, was similar to the healthy reference population. 17 In the other screening study by Johnston et al., 18 adults were asked about quality-of-life at the time of the screening and after one year. 18 No significant differences in quality-of-life were found between the screening-detected and the healthy controls at baseline or after one year. 18 They also looked at a clinically diagnosed group and found that their quality-of-life was lower at baseline compared with the healthy controls and, unlike those with screening-detected CD, those who were clinically diagnosed reported a higher quality-of-life at the one-year follow-up than at baseline. 18
Studies exploring HRQoL of people with CD have also asked respondents to recall their HRQoL before they were clinically diagnosed, 10 or the individuals who were screened belonged to a high-risk group.28,40 A recent study by Gray et al. 10 surveyed members of a UK coeliac society and asked them to recall HRQoL before and after the CD diagnosis. They used a questionnaire that included the EQ-5D instrument and showed that symptoms of unrecognized CD were associated with a prolonged and substantial reduction in HRQoL. 10 They explained that their estimates were based on retrospective assessments, and that this was unavoidable in the absence of large, long-term prospective studies. 10 However, our study with a prospective design helps fill this informational gap.
Although it has been suggested that a prospective design is needed to assess HRQoL related to screening-detected CD, 10 there may be an advantage to using a retrospective design. Results from a qualitative study, which included some of the same screening-detected children as from our study, showed that one year after diagnosis and a gluten-free diet, some children realized they had had symptoms before diagnosis of which they had not been fully aware. 9 We used the EQ-5D instrument which is a generic tool used to describe HRQoL, 21 and our results are similar to those reported in other studies with Swedish children,23,25 however, this tool may fail to capture the impact of mild or subtle symptoms of CD.
Conclusions
The HRQoL reported by 12-year-olds with screening-detected CD, before they learned of their diagnosis, was not worse than that of the children without CD or those previously diagnosed with CD. Thus, mass screening for CD should not be justified on the basis that children with unrecognized CD have a poor HRQoL. However, because these children rated their HRQoL before diagnosis and treatment, they may not have recognized or perceived symptoms as severe enough to seek medical attention, which demonstrates how difficult clinical/active case finding can be. Mass screening may still be considered, therefore, as a viable option if the aim is early detection and prevention of future complications. More knowledge is still needed regarding the long-term consequences of untreated CD.1,3,8
Footnotes
Acknowledgements
We thank all children and families, teachers, school nurses and research nurses involved in the ETICS study and Hans Stenlund for statistical analysis support. We would also like to thank Kristina Burström, Karolinska Institutet and Ann-Charlotte Egmar, Red Cross University Hospital, for providing the Swedish child-friendly pilot version of the EQ-5D instrument and valuable comments.