
Abstract
Objectives
To evaluate the effectiveness of the Pap smear screening programme in Thailand in the prevention of invasive cervical cancer.
Setting
Four tertiary hospitals, in two provinces of north-east Thailand.
Methods
A hospital-based case-control study of women aged 30–64, who were resident in north-east Thailand. A total of 130 women with a diagnosis of invasive cervical cancer were compared with two groups of controls: a) hospital controls, b) hospital patient companions. Information on risk factors for cervical cancer and history of screening by cytology (Pap smear) were collected using a structured interview.
Results
Eighty percent of control subjects reported having had a Pap test in the past, and some two-thirds within the three years before interview. There was a significant protective effect for multiple (6+) previous screening tests as reported by 20% of controls. When women who had tests less than six months prior to the study were excluded, there was a strong, significant protective effect of the number of tests (for 1–5 tests: OR = 0.45 95% CI = 0.25 to 0.84, and for 6+ tests: OR = 0.29 95% CI = 0.11 to 0.82). Tests carried out 1–2 years and 3+ years before diagnosis were associated with an OR of 0.27 (95% CI = 0.13–0.56) and 0.42 (95% CI = 0.20–0.88), respectively.
Conclusions
The cervical screening programme in north-east Thailand has achieved excellent coverage and is preventing cervical cancer. Women who have been screened multiple times are at substantially lower risk than those only screened a few times suggesting that the quality of the screening could be improved.
Introduction
Cytological screening aims to prevent cervical cancer by identifying and allowing treatment of women with precursor lesions. To be effective, a screening programme should identify women at risk, ensure that they are examined at regular, defined intervals and provide appropriate follow-up and treatment for those women with abnormal cytological test results. In Thailand, prior to 2005, there were no ‘organized’ programmes of this kind; screening was opportunistic, involving fee-for-service testing of women ‘on demand’, or when attending services such as family planning, pregnancy counseling, ante- and postnatal clinics or sexually transmitted disease (STD) clinics, with sporadic campaigns mounted by local health departments or charitable foundations.5–7
In 2005 the Department of Medical Service (DOMS) and the Thai National Cancer Institute (TNCI) established a more formal cervical cancer screening programme, in which Pap smears were recommended each year for all Thai women at the age of 35, 40, 45, 50, 55 and 60. The programme was designed to offer colposcopy to women with abnormal test results, with cryotherapy and loop electrosurgical excision procedure (LEEP) provided for those found to have abnormalities. This screening programme has been implemented in all 76 provinces of Thailand. 8
Six years have passed since the introduction of this national programme, and it is time to evaluate how effective it has been in the prevention of invasive cervical cancer. In this paper, we evaluate the prevalence of cytological screening in the population of Khon Kaen province, northeast Thailand, and the protection offered against the risk of invasive cancer in relation to the recency and number of tests.
Various demographic and behavioural factors have been found to be associated with the probability of being screened, such as age, marital status, education, socioeconomic status and parity. 2 These, and other variables associated with them (such as smoking and sexual history), are also associated with the risk of cervical cancer, either directly, or through their link with infection with oncogenic human papillomavirus (HPV), the major aetiological agent. 9 Adjustment for the resulting confounding is therefore necessary when quantifying the protective effect of screening. 10
Materials and Methods
A case-control study was conducted between May and December 2009. All subjects were identified from four tertiary hospitals in two provinces of north-east Thailand: Srinagarind Hospital, Khon Kaen Regional Center Hospital, Udonthani Regional Center Hospital and Udonthani Cancer Center. Subjects were identified as residents of the north-east region aged 30–64. They were interviewed by one of four trained interviewers using a structured questionnaire seeking information on sociodemographic variables, reproductive and gynaecological history, potential risk factors for cervical cancer, and history of cervical cytology including the number of tests and timing of previous tests.
This study was approved by the Ethical Review Boards in Khon Kaen University, Khon Kaen Regional Center Hospital and Udonthani Regional Center Hospital.
Cases
Cases were women diagnosed with invasive cancer within three months before interview. Only cases with histologically confirmed primary invasive cervical carcinoma were included. A total of 130 women (out of 135 invited) agreed to participate and completed an interview.
Controls
Two groups of 130 control subjects (hospital controls and hospital patient companions) were recruited; each was frequency matched by age, within 10-year age groups, with the case group. The participation rates were 95% (130/137) and 93% (130/140), respectively.
Hospital controls were randomly selected from general surgery wards, medical wards and private rooms in the same hospitals as those where the cases were recruited; women with gynaecological diseases were excluded.
The hospital patient companions were apparently healthy women who were accompanying, or visiting, patients in the same hospitals (not including the patients who were included as cases in this study).
Screening history
The interviewers recorded information from case and control subjects on:
Whether the subject knew about screening for cervical cancer and/or the Pap smear; Whether the subject had ever had cervical cancer screening by Pap smear, and, if so; How many times they had had a test; and When was the most recent test.
The interval between the most recent test and date of diagnosis (or date of interview for controls) was grouped into five categories: (a) no Pap smears (never); (b) <6 months; (c) 6 months – 11 months; (d) 12–35 months; and (e) three or more years.
Statistical analysis
Univariate statistical analyses were undertaken for cases and each control group, as well as for cases and the combined controls. Logistical regression 11 was performed to evaluate the association between invasive cervical cancer and history of cervical cancer screening (recency of test) and the number of tests (0, 1–5, 6+). Similarly, potential risk factors for cervical cancer, including educational level (higher, high school, and primary school or less), income (≥10,000 baht/month, 5,000–9,999 baht/month and <5,000 baht/month), age at first sexual intercourse (>18 years, and ≤18 years), alcohol consumption (yes, no), ever used oral contraceptive pill (yes, no), ever used contraceptive implants (yes, no). Odds ratios (OR) were estimated with 95% confidence intervals (CI) in logistic regression models, and a P value of less than 0.05 was considered to indicate statistical significance. Multivariate logistic regression was used to control for potential confounding factors. All statistical tests were two-sided. Analyses were completed with the use of STATA software, version 10. 12
Results
The cases were resident in 11 provinces of the northern part of the north-east region, with 78 (60%) from the provinces of Khon Kaen, Udonthani, and Sakolnakorn. Seventy-seven percent of patients had squamous cell carcinomas and 23% adenocarcinomas. The mean age of the cases was 48.6 (SD = 8.0), and the control groups were closely matched for age (means 48.9 for hospital controls and 47.6 for hospital patient companions), and very similar by place of residence (58% and 62% respectively from the same three provinces). Virtually all study participants were (or had been) married (99% of cases, 97% of hospital controls and 98% of companion controls). The distribution of parity was similar in the patient and control groups: approximately 50% of both cases and controls had one or two children, with the mean number of children being 2.8 (SD = 1.3) for cases, 2.6 (SD = 1.3) for hospital controls and 2.4 (SD = 0.9) for hospital patient companions.
Table 1 shows the distribution of other risk factors in cases and the two control groups, and the associated crude odds ratios and 95% confidence intervals. Of the 130 cases, 65 (50%) had their first sexual intercourse at ≤18 years, but for control subjects the frequencies were considerably lower (26% and 22%). The educational level of cases was lower than that of controls (79% primary school or less). For more than half of cases and hospital controls, the occupations were unemployed/farmers, while 57 (44%) of hospital patient companions were business or government officers. The mean monthly household income was higher in the controls than in the cases (17,641 and 20,757 baht vs. 9029 baht).
Distribution of risk factors and screening history in cases and controls (hospital controls and hospital patient companions), and the associated crude odds ratios (with 95% confidence intervals)
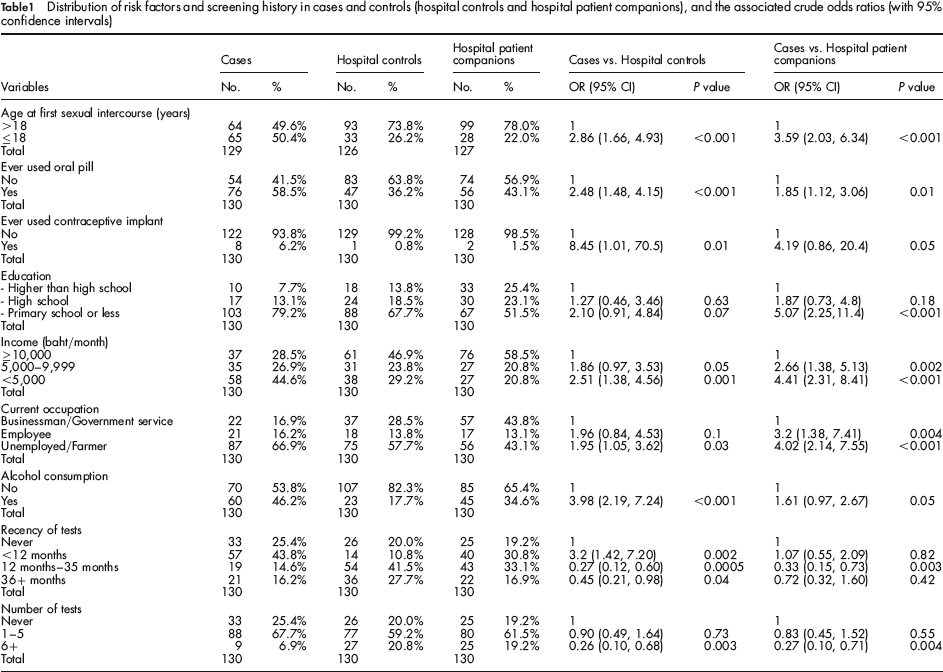
Risk of cervical cancer was significantly associated with age at first sexual intercourse in comparison with both control groups, as were use of oral contraception and income. Use of contraceptive implants and alcohol consumption were significantly associated with cervical cancer when compared with hospital controls (P = 0.01, and <0.001, respectively), while unemployment/farmer and employee status were significantly associated with cervical cancer compared with hospital patient companions (P = <0.001, and P = 0.004, respectively).
Nineteen percent of the disease-free hospital visitor companions reported never having had a Pap smear, while for 17% the most recent test was three or more years earlier; and 19% had had six or more tests in the past. The values were 20% (never), 28% (last test ≥3 years earlier), and 21% (6 or more tests) for the hospital controls. Compared with women who had never had a test, there were reduced risks with number and recency of tests, using either control group.
Using the categories in Table 1, formal comparison of the two control groups showed no significant differences between them with respect to the distribution of risk factors, or Pap smear history. Further analyses therefore made use of the combined control groups (260 subjects); Table 2 shows the crude odds ratios and 95% confidence intervals of risk factors for developing cervical cancer, using the combined control group. Risk factors significantly associated with cancer were age at first sexual intercourse (P = <0.001), use of oral contraceptives (P = 0.0004), use of contraceptive implant (P = 0.005), educational level (P = 0.0006), and alcohol consumption (P = <0.001). Other factors significantly associated with cancer were unemployment/ farmer and employee status (P = 0.0001, and P = 0.008 respectively), income of 5,000–9,999 baht/month and <5,000 baht/month (P = 0.004, and < 0.001 respectively), tests in past 1–2 years (P = 0.0003), and a history of 6+ tests (P = 0.001).
Crude and adjusted odds ratios and 95% confidence intervals for risk factors and screening history: cases and combined control groups
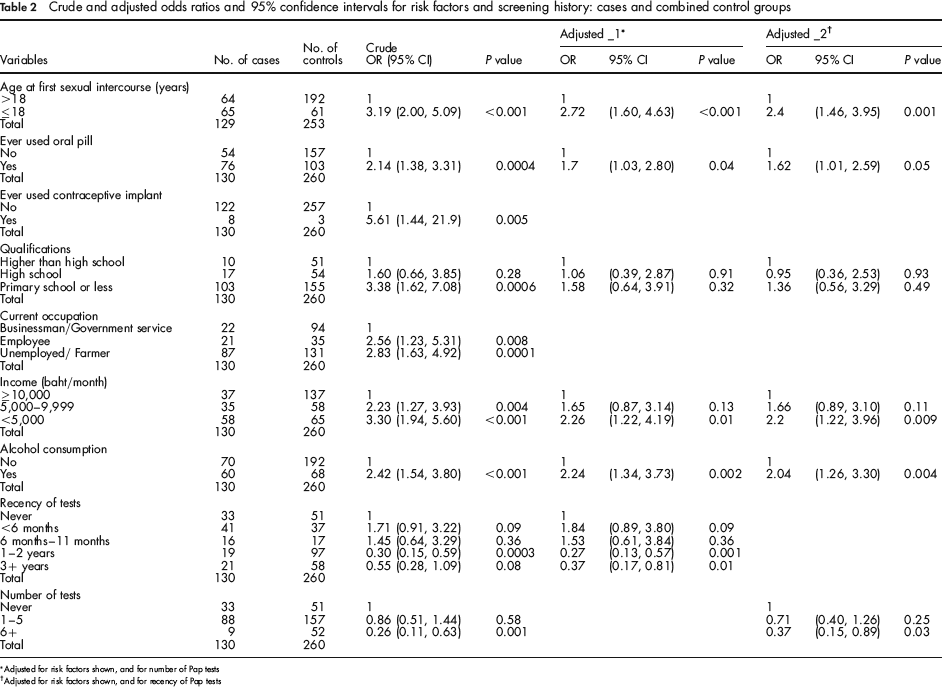
Adjusted for risk factors shown, and for number of Pap tests
Adjusted for risk factors shown, and for recency of Pap tests
Nearly a third of cases (32%) reported a screening test in the six months prior to enrolment. Undoubtedly many of these will have been symptomatic smears while others will have been in women with screen-detected cancer. It is difficult therefore to interpret the relevance of the odds ratios associated with recency of test. Nevertheless, the odds ratio comparing 1–2 years with 3+ years in cases versus the combined controls of 0.54 (95% CI 0.25–1.16) suggests that more recent screening is associated with a lower risk of cervical cancer.
Multivariable analysis was carried out using backward elimination logistic regression, including the five variables found to have a strong association with cervical cancer (but excluding occupation, because of co-linearity with education, and contraceptive implants, because of the small number of users). Table 2 shows the adjusted odds ratios and 95% CIs resulting from this analysis, when either recency of tests (‘Adjusted_1’) or number of tests (‘Adjusted_2’) is included as an independent variable. The significant remaining variables were alcohol consumption, age at first sexual intercourse, and use of the oral contraceptive pill. Markers of socio-economic status (educational level, occupation, income) were no longer significantly associated with risk of cervical cancer.
As expected the number of tests had a protective effect as indicated by the differences in results for 1–5 previous tests compared with those for 6+ previous tests (OR = 0.71 95% CI = 0.40 to 1.26 and OR = 0.37 95% CI = 0.15 to 0.89, respectively).
A distinction needs to be made between a Pap smear done for the purpose of screening and one done for diagnostic purposes in a patient coming to medical attention with a suspected diagnosis of cervical cancer. The multivariable analysis was therefore repeated excluding all women who had a smear performed less than six months prior to data collection. The results of this analysis are shown in Table 3. There was a protective effect of the number of tests (for 1–5 tests: OR = 0.45 95% CI = 0.25 to 0.84, and for 6+ tests: OR = 0.29 95% CI = 0.11 to 0.82; P for trend = 0.001) that was much stronger than in the analysis including recent tests (Table 2) suggesting that many of the cases with 1–5 tests had only been tested in the months leading up to diagnosis. The adjusted odds ratio for a recency of tests 6 months – 11 months (OR = 1.38 95% CI = 0.56 to 3.40) was slightly lower than the crude OR (1.45), while the significant protective effects of tests 1–2 years and 3 + years remained (OR = 0.27 95% CI = 0.13 to 0.56 and OR = 0.42 95% CI = 0.20 to 0.88, respectively; P for trend = 0.004)
Crude and adjusted odds ratios and 95% confidence intervals for the effect of screening on risk of invasive cervical cancer, excluding women who had tests less than six months previously. Case and combined control group
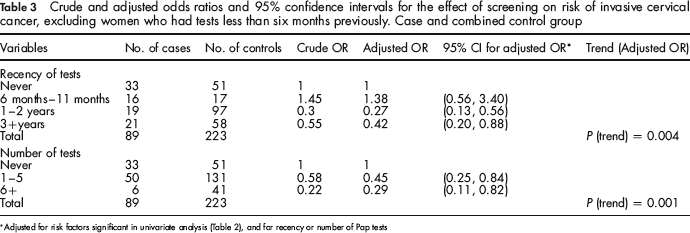
Adjusted for risk factors significant in univariate analysis (Table 2), and for recency or number of Pap tests
Discussion
Prior to 2005, screening for cervical cancer in Thailand was primarily opportunistic and resulted in screening being mainly offered to younger women at relatively low risk.13,14 As a consequence, population coverage has been poor. The Sexual and Reproductive Health Survey in 2005 found that 37% of the female population between 35 and 59 years of age had never been screened during their lifetime, and only 50% had been exposed to the screening service at least once within a five-year interval. 15 In Khon Kaen province, a self-report survey study conducted in 2000 found that 33% of women aged 20 and above had never undergone a Pap smear test. 13 A national call and recall programme, aiming at five yearly testing of women aged over 35 was launched in 2005. The current study was designed to evaluate the effectiveness of cervical screening in the north-east region, and, in doing so, we studied the role of risk factors for cervical cancer, in as much as many of them are important confounders (being also associated with attendance at screening). It is well known, for example, that cervical cancer risk is associated with low socio-economic status. In our study, women with only primary-level education had a three-fold increased risk when compared with those who had graduated higher than high school. However, after adjustment for other factors, no association remained. Similarly, the findings of other studies in Mexico reported that in the crude analysis, women who did not have any formal education had a two-fold increased risk when compared with those who had more than seven years of education. When adjusted for other risk factors, no association with cervical cancer remained. 16 Combined oestrogen-progestogen oral contraceptives are known to increase the risk of cervical cancer. 17 The association between cervical cancer and alcohol intake observed in our study is surprising, since alcohol is not an accepted risk factor for cervical cancer. 18 The crude odds ratio of 2.4 was only slightly reduced by adjustment for the other factors; nevertheless, residual confounding, or confounding with an unmeasured variable, seems the most likely explanation.
The case-control design has been widely used in studies evaluating cervical cancer screening. 19 Evaluation of the protective effect of screening tests would ideally enumerate such tests, and their timing relative to the diagnosis of invasive cancer. 20 Our study relied upon self-report of Pap smears and included information only on the number of tests and the timing of the most recent test. Inevitably, there will be considerable misclassification in a population of women who may not be well informed about Pap smears or the nature of gynaecological examinations that they have undergone; furthermore it is possible that accuracy of reporting would be higher in cases compared with controls, because of recall bias. Observer bias was unavoidable, since the interviewers knew which subjects belonged to the cases or a control group. This knowledge could have affected the way in which the interviews were conducted and the information elicited from the participants in the different groups. In addition, we were unable to distinguish between reports of Pap smears taken for screening, and those for diagnostic purposes in women with gynaecological symptoms. Such diagnostic tests are more likely in the case group, and this is most likely the explanation for the slightly increased risk (non-significant) associated with recent tests (within 12 months of diagnosis). One conventional solution is to exclude from analysis all tests within six months of diagnosis (and an equivalent period in the controls), although this is not ideal, and results in an over-estimate of the protective effect of screening, to the extent that the screening test results in the diagnosis of invasive cancer, rather than precursor lesions. 21 Since we have no information on the timing of the previous tests in women whose most recent test was within six months of study entry, we instead excluded all women with a test in the last six months. After this exclusion, we observed the risk reduction appeared to be greater for more recent smears, and even smears done three years or more previously were associated with a reduced risk of cervical cancer.
There have been only a few previous studies of the effectiveness of screening with Pap smears in Thailand. In one hospital-based case-control study, the risk of invasive cervical cancer decreased significantly as the frequency of Pap smears increased and was reduced by 75% in women, who had at least one Pap smear per year. 22 A larger hospital-based case-control study in southern Thailand found that the risk of cervical cancer increased with the interval since the previous Pap smear. 23 These are similar to observations in other developing country settings, for example in China, Mexico and South Africa.24,16,25
We used two control groups with no evidence of cervical cancer (or other gynaecological disease). Hospital controls are the conventional method of matching with the case group with respect to those (unmeasured) factors resulting in treatment in a particular hospital. 26 The use of hospital patients as controls also has the advantage that, as inpatients, they may be more motivated to help medical research and more conscientious in supplying information than community control subjects. However, hospital patients may have rather different exposure experience than healthy subjects. We therefore also used a group of women without disease, who happened to be present as visitors to, or otherwise accompanying patients in the same hospital as the cases. Such subjects are a convenient alternative to community controls, and are presumably well matched to cases with respect to factors related to hospital referral. 27 The selection of visitor/companions of hospital patients who were not study subjects minimizes the risk of overmatching on social factors.
This study aimed to evaluate the effectiveness of cervical cancer screening by cytology in north-east Thailand. The protective effect is quantified based on the odds ratios of screening in cases and control subjects, and taken at face value suggests that a smear every one or two years would prevent more than 70% of cervical cancer, and tests at intervals of three years or more, around 60%. It is likely to be an overestimate. These estimates do not take into account any residual selection bias; although the protective effects were estimated following adjustment for important behavioural risk factors, it is quite possible that there is residual bias, in that subjects who choose to be screened are at lower risk of disease, irrespective of the effect of the test. The ORs in cohort studies of risk between non-responders and controls (a population not offered screening) was about 1.5 which indicates that the non-responders have an inherent risk up to two times that among responders. 2 If this were the case in this Thai population, the real protective effect of a test within the previous two years would be about a halving of risk, with tests at longer intervals having quite a small (∼20% reduction) benefit. These estimates also do not take into account screen-detected cancers. If such cancers are mostly early stage then our estimates may be reasonable for the proportion of advanced stage cancers prevented.
On the other hand, population coverage by the screening programme was, by 2009, rather good, as judged by the reported screening experience of the control subjects (and especially the hospital visitors, who would most likely have a screening experience comparable to that of the general population). Only about 20% had never had a Pap smear, while some 64% had been examined within the previous two years. It will be of interest to observe whether a change in the trends in the incidence of cancer of the cervix can be observed in data from the provincial cancer registries of Khon Kaen and Udonthani; any change in mortality rates would be of smaller magnitude, and occur rather later. Further research is underway to investigate the factors relating to attendance at routine screening, including knowledge, attitude, beliefs in relation to the disease and its prevention, so the relevant health departments can improve quality and availability of screening in the local population.
Footnotes
Acknowledgements
We would like to acknowledge the financial support from the Royal Golden Jubilee PhD Program scholarship for Chananya Kasinpila (Grant No. PHD/0184/2549) from the Thailand Research Fund, the Graduate School, Khon Kaen University, and the National Research Council of Thailand. This research was approved by the Khon Kaen University Ethics Committee for Human Research based on the Declaration of Helsinki and Good Clinical Practice Guideline (ICH GCP), Reference No. HE511025.