
Abstract
Objectives
(i) To document the current state of the English, Scottish, Welsh, Northern Irish and Australian bowel cancer screening programmes, according to seven key characteristics, and (ii) to explore the policy trade-offs resulting from inadequate funding.
Setting
United Kingdom and Australia.
Methods
A comparative case study design using document and key informant interview analysis. Data were collated for each national jurisdiction on seven key programme characteristics: screening frequency, population coverage, quality of test, programme model, quality of follow-up, quality of colonoscopy and quality of data collection. A list of optimal features for each of the seven characteristics was compiled, based on the FOBT screening literature and our detailed examination of each programme.
Results
Each country made different implementation choices or trade-offs intended to conserve costs and/or manage limited and expensive resources. The overall outcome of these trade-offs was probable lower programme effectiveness as a result of compromises such as reduced screening frequency, restricted target age range, the use of less accurate tests, the deliberate setting of low programme positivity rates or increased inconvenience to participants from re-testing.
Conclusions
Insufficient funding has forced programme administrators to make trade-offs that may undermine the potential net population benefits achieved in randomized controlled trials. Such policy compromise contravenes the principle of evidence-based practice which is dependent on adequate funding being made available.
Introduction
A 2008 review of bowel cancer screening initiatives across 17 countries found FOBTs were the most commonly used screening modality. 7 There are good reasons for governments to allocate funding for FOBT screening programmes. If the 25% relative mortality reduction demonstrated in the intention-to-treat data from the most recent meta-analysis 8 was achieved, almost 4,000 lives in the UK and over 1,000 lives in Australia could be saved each year. Bowel cancer screening can also lead to lower incidence of bowel cancer in the screened population, as the removal of precancerous adenomas prevents the disease occurring. 9 Conversely, the number and severity of potential harms from bowel cancer screening are relatively small, as serious adverse events are rare, and anxiety associated with it is believed to be relatively short-term and minor. 10
In order to achieve the same or greater magnitude of benefits demonstrated in randomized controlled trials (RCTs), FOBT programmes should be based on the best available evidence. This paper focuses on seven key characteristics we believe are most salient for a population cancerscreening programme and explores the policy trade-offs in these characteristics that result from inadequate funding. Trade-offs are defined as compromises made in one area to obtain benefits in another.
Methodology
Comparative case study methodology was used to explore in detail the different versions of FOBT screening programmes. This approach emphasizes the importance of describing and interpreting events and their context, in order to illuminate more general issues. 11 For us, the wider issue was the relationship between evidence-informed policy decisions and the implementation of these policy decisions in practice.
Methods
Document Collection
Major documents relating to the five programmes were examined, beginning with background documents to the establishment of the UK and Australian Pilot Programmes. The aim was to establish as complete a set of programme documents as possible. Other sources included commissioned reports, guidelines, press releases, election campaign documents, websites and federal government budget papers. Interview respondents were also helpful in identifying additional relevant documents and some provided copies of background correspondence.
Interviews
A total of 42 key respondents were interviewed between August 2007 and October 2009 (34 from Australia and eight from the UK). Interviews were semi-structured and lasted between 30 and 90 minutes. Questions varied according to the participant's role in bowel cancer screening policy. All interviews were digitally recorded and transcribed by a professional transcription service.
The Australian interviews were conducted first and purposive sampling was used to achieve a maximum diversity sample, across clinical, methodological and policy expertise and involvement across the policy development timeline. Members of the two major government review committees4,6 were initially interviewed and our sample was extended based on further document analysis and suggestions from respondents. Interviewees included representatives from cancer organizations, academics, clinicians, former and current state and federal bureaucrats and political advisors.
The UK interviewees were also selected using purposive sampling, with interviews conducted in England and Scotland over a two-week period. Interviewees included those involved in establishing and analysing the Pilots, as well as those responsible for running the English and Scottish programmes. It was a small but highly knowledgeable group.
Email Correspondence
Email correspondence was used to obtain information on the Welsh and Northern Irish programmes, updates on the implementation of the English and Scottish programmes, and information on the implementation within the six Australian states and two territories. This added a further six UK and eight Australian respondents to the 42 key respondents interviewed via telephone or face-to-face, making a total of 56 informants. For confidentiality reasons, respondents are referred to only by their identification number, preceded by UK (United Kingdom) or an A (Australia) given in square brackets after quotations or references attributable to them.
Data Analysis
Information obtained from the documents, interviews and email correspondence was used to compile a table of the seven most salient programme characteristics, as determined by discussion among the authors. Based on our reading of the literature and interview responses from key informants, we proposed a set of ‘optimal’ features for each characteristic. We then compared what had actually happened in practice in each of the five countries (Table 1) with these optimal features (Table 2). Interview data provided insights into the rationale behind some programme implementation choices.
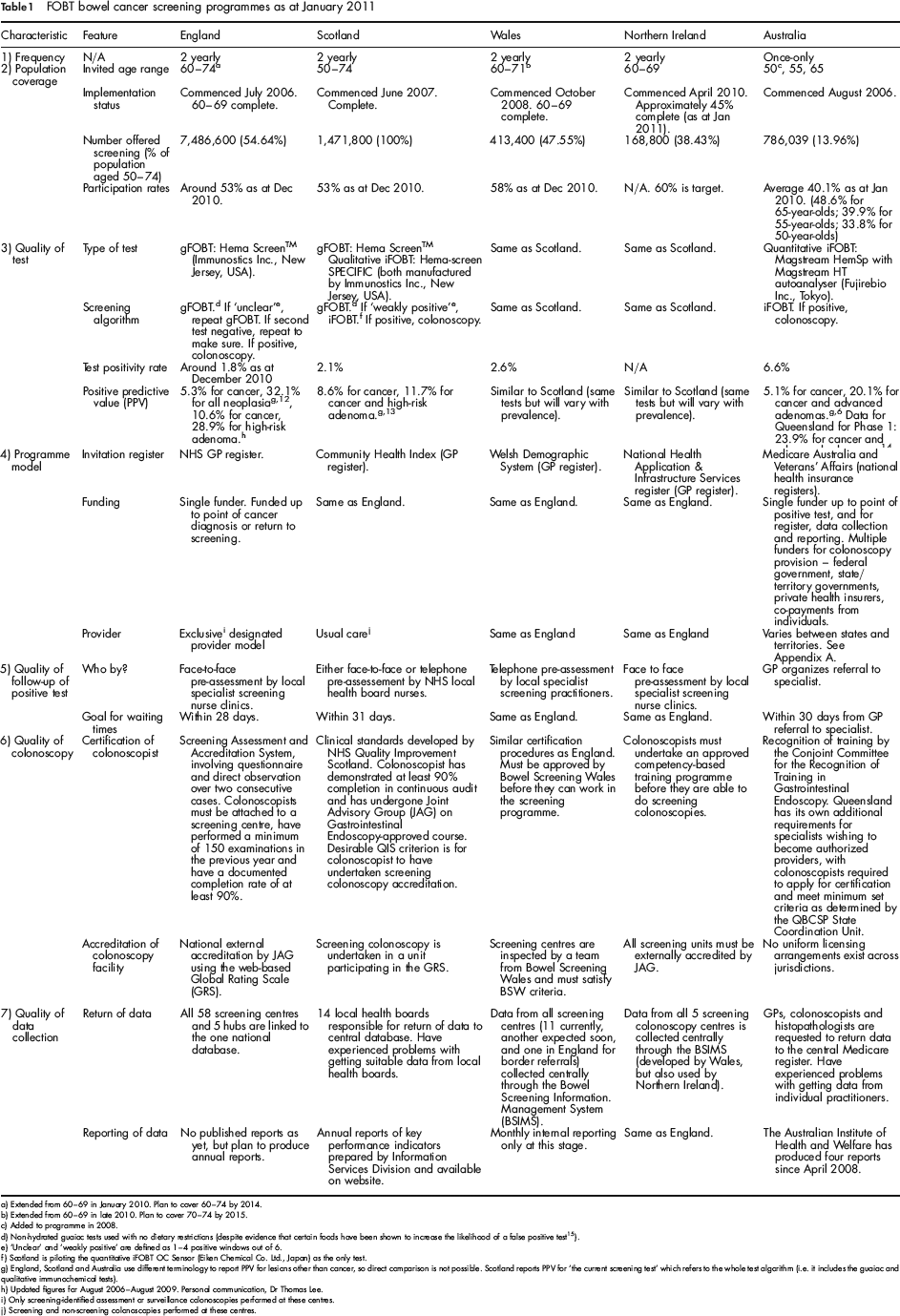
FOBT bowel cancer screening programmes as at January 2011
FOBT bowel cancer screening programmes as at January 2011
Extended from 60–69 in January 2010. Plan to cover 60–74 by 2014.
Extended from 60–69 in late 2010. Plan to cover 70–74 by 2015.
Added to programme in 2008.
Non-hydrated guaiac tests used with no dietary restrictions (despite evidence that certain foods have been shown to increase the likelihood of a false positive test 15 ).
‘Unclear’ and ‘weakly positive’ are defined as 1–4 positive windows out of 6.
Scotland is piloting the quantitative iFOBT OC Sensor (Eiken Chemical Co. Ltd., Japan) as the only test.
England, Scotland and Australia use different terminology to report PPV for lesions other than cancer, so direct comparison is not possible. Scotland reports PPV for ‘the current screening test’ which refers to the whole test algorithm (i.e. it includes the guaiac and qualitative immunochemical tests).
Updated figures for August 2006-August 2009. Personal communication, Dr Thomas Lee.
Only screening-identified assessment or surveillance colonoscopies performed at these centres.
Screening and non-screening colonoscopies performed at these centres.
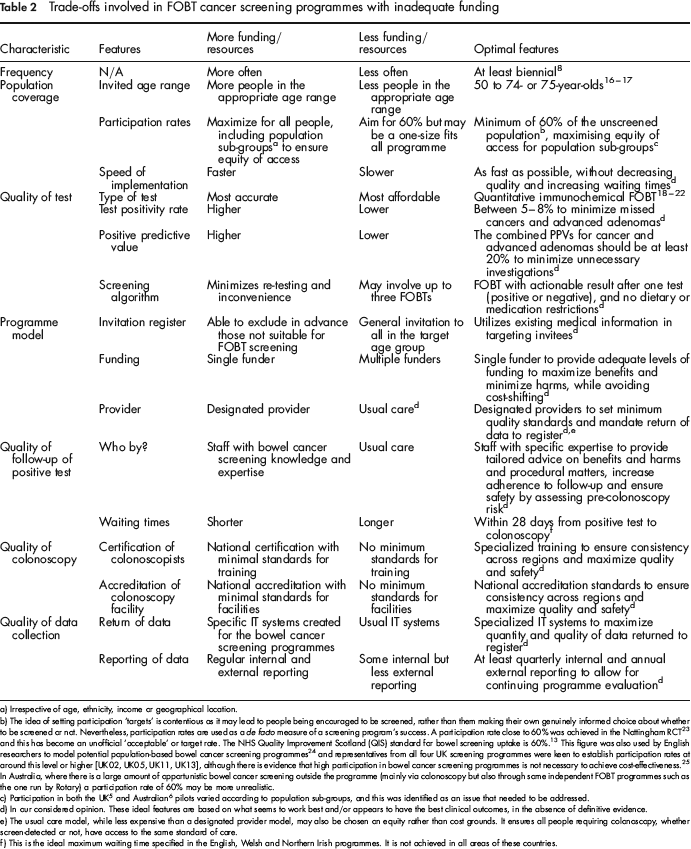
Trade-offs involved in FOBT cancer screening programmes with inadequate funding
Irrespective of age, ethnicity, income or geographical location.
The idea of setting participation ‘targets’ is contentious as it may lead to people being encouraged to be screened, rather than them making their own genuinely informed choice about whether to be screened or not. Nevertheless, participation rates are used as a de facto measure of a screening program's success. A participation rate close to 60% was achieved in the Nottingham RCT 23 and this has become an unofficial ‘acceptable’ or target rate. The NHS Quality Improvement Scotland (QIS) standard for bowel screening uptake is 60%. This figure was also used by English researchers to model potential population-based bowel cancer screening programmes 24 and representatives from all four UK screening programmes were keen to establish participation rates at around this level or higher [UK02, UK05, UK11, UK13], although there is evidence that high participation in bowel cancer screening programmes is not necessary to achieve cost-effectiveness. 25 In Australia, wherethereisa large amount of opportunistic bowel cancer screening outside the programme (mainly via colonoscopy but also through some independent FOBT programmes such as the one run by Rotary) a participation rate of 60% may be more unrealistic.
Participation in both the UK 5 and Australian 6 pilots varied according to population sub-groups, and this was identified as an issue that needed to be addressed.
In our considered opinion. These ideal features are based on what seems to work best and/or appears to have the best clinical outcomes, in the absence of definitive evidence.
The usual care model, while less expensive than a designated provider model, may also be chosen on equity rather than cost grounds. It ensures all people requiring colonoscopy, whether screen-detected or not, have access to the same standard of care.
This is the ideal maximum waiting time specified in the English, Welsh and Northern Irish programmes. It is not achieved in all areas of these countries.
Results
Our main findings are presented in Tables 1 and 2, followed by commentary on the types of trade-offs involved for each of the seven characteristics. Details of programme implementation within Australia are provided in Appendix A.
Australia is the only country to not offer screening every two years, despite biennial screening being part of the Australian Pilot programme's suggested framework 6 and the Australian National Health and Medical Research Council (NHMRC) guidelines recommending at least biennial FOBT screening. 26 Although screening less often reduces the cost of the programme, it is unlikely to improve its cost-effectiveness, as the expected benefits of the programme are also reduced. The trade-off here is between the up-front costs versus the longer-term cost-effectiveness of the programme. It is unlikely that the mortality reductions attained in the RCTs are achievable in the Australian programme which only offers screening to individuals at 50, 55 and 65.
Population Coverage
The more people included in the target population, the greater the cost of a screening programme. England's total target population is five times larger than Scotland's and eighteen times larger than Australia's. Bowel cancer screening is the first organized screening programme offered to men and women, so the target population is much higher than for programmes offered only to women in a similar age range. For example, in Scotland the target population for breast cancer screening (women aged 50–70) is 672,200, compared with that for bowel cancer screening (men and women aged 50–74) which is 1,471,800. 27 Scotland's choice to offer screening to 50–74-year-olds was based on the Council of the European Union's recommendation, 16 but suited Scotland's desire for age-based equity: “I think the whole ethos of the Scots Calvinistic sort of, Presbyterian approach is very socialist … and everyone has to have equitable access to health services and there shouldn't be different tiers of delivery of health services” [UK03]. Because 74-year-olds today are healthier and have a longer life expectancy than when the trials were conducted in the late 1970s to early 1990s, demand may increase in the future. As one respondent noted “we're now beginning to find people over the age of 74 knocking on the door and saying what about us?” [UK04].
The decision to initially limit screening to 60–69-year-olds in England, Scotland and Northern Ireland was pragmatic, reflecting the shortage of colonoscopy capacity in some areas [UK05, UK11, UK13], but was in line with the then recommendations of the UK NSC to routinely screen those in their 60s while allowing older people to request screening. The lack of screening for those in their 50s was not an ideal arrangement, as the risk of bowel cancer incidence and mortality does increase steadily from age 5028,29 and trial evidence included participants in this age range. 8 Following approval by the UK NSC in April 2011, 30 National Health Service (NHS) England has announced plans for once-only flexible sigmoidoscopy screening at age 55, in addition to FOBT screening. 31
Given the limited resources, however, the decision to focus FOBT screening on the above-60s, where the majority of cancerous and pre-cancerous lesions will be found, makes sense. In Australia, the decision to limit screening to 55- and 65-year-olds (later expanded to include 50-year-olds) was justified on the basis of the need to manage the capacity of health services, 32 although Australia has a much higher colonoscopy capacity per capita than the UK. 33 As a result, many of the people who may benefit most from screening, particularly those aged 66–75, are not screened at all in the current Australian programme.
Quality of Test
The choice of a FOBT represents a trade-off between the more costly but more accurate immunochemical test (iFOBT), versus the less expensive but less accurate guaiac test (gFOBT). Only Australia uses a quantitative automated iFOBT in their programme, which has been found to have superior clinical benefits over gFOBTs used in the UK.18–22
The choice of test also affects the screening algorithm, which is a trade-off between accuracy and convenience of testing for the screening participant. The iFOBT gives an actionable result (test is positive or negative) and avoids the need for repeated re-testing. In England, participants may be required to complete a gFOBT up to three times and the programme loses many participants to further testing due to the extended screening episodes [UK03]. The programmes in Wales and Northern Ireland have adopted the Scottish algorithm, which involves using gFOBT as the first test, and then following up people who have a ‘weakly positive’ test (that is, 1–4 of 6 windows positive) with a qualitative iFOBT. This ‘two tier’ approach is not without its problems. Although this strategy may reduce the number of colonoscopies (by reducing the number of false positive tests), the overall programme sensitivity is still limited by the sensitivity of the initial gFOBT. 34
Ideally, a screening programme should be capable of finding all the pathology that exists in the target population. In practice, this is usually not feasible. As van Rossum et al. have noted: ‘Policy makers will determine the optimal cutoff value [the point at which the test is considered to be positive or negative] on the basis of a largely arbitrary balance between the acceptability of missing cancer and the possibility and acceptability of assigning essential resources.’ 35 Scotland is currently conducting a trial of a quantitative automated iFOBT to replace the current algorithm, but even if funded, the positivity rate will still need to be set at around 2% as their health system will not cope with additional colonoscopies required to deal with a larger pathology yield [UK04].
Programme Model
The English, Welsh and Northern Irish programmes follow a single funder exclusive designated provider model. It separates the provision of screening colonoscopies from symptomatic or surveillance colonoscopies, and so follows the model for breast cancer screening. The developers of the UK breast cancer screening programme deliberately differentiated between screening and non-screening cases, arguing that this was preferable, because even though initially the women being screened for breast cancer may have better facilities, it was important to first establish those high standards [UK07].
Scotland intentionally took a different approach because they did not want to create a ‘two-tier’ system where people receiving colonoscopy as part of the screening programme were guaranteed high-quality colonoscopy, but those with symptoms or on a surveillance programme were not [UK03]. Each of the fourteen Scottish health boards are responsibile for ensuring a positive FOBT is treated in the same way as an urgent GP referral with fast-tracked investigation and treatment [UK03]. In all four UK countries, most screening follow-up is delivered in the public sector, without GP involvement.
In Australia, the bowel cancer screening programme was established as a ‘usual care’ model, with the federal government funding the screening pathway only up to the point of a positive FOBT. The state and territory governments, which are responsible for funding of hospital-based services, were left to cover the costs of colonoscopy facilities for follow-up of positive FOBTs performed in the public sector.
Quality of Follow-Up Of Positive Test
In the designated provider jurisdictions in the UK, a central body is responsible for organising precolonoscopy assessment appointments by specialized staff for those with positive FOBTs. In Scotland precolonoscopy assessment is arranged by local NHS boards and the quality may vary [UK04]. Similarly, in Australia there is no nationally co-ordinated process for precolonoscopy assessment, which is organized through GPs who may lack screening expertise or the time to devote to discussion of the pros and cons of further testing.
There is the potential for screening colonoscopies to impact on waiting times for people needing surveillance colonoscopies or those presenting with symptoms. Countries with limited colonoscopy capacity may find this difficult to manage. In Australia, over 500,000 colonoscopies are performed annually. As at January 2010, fewer than 29,000 colonoscopies were undertaken through the National Bowel Cancer Screening Program (NBCSP), 36 so colonoscopy capacity is not the major issue. The choice of the ‘usual care’ model, however, has led to wide variation in the quality of follow-up between the States (see Appendix A).
Over 75% of colonoscopies performed in Australia are carried out in the private sector. 33 Although this reduces the financial impact of a screening programme on public sector facilities, the federal government still pays the majority of colonoscopy costs through the fee for service-based Medicare Benefits Schedule. Participants are reimbursed through their private health insurance (if covered) but are liable for any ‘gap’ payment if there is a difference between the private health fund reimbursement and the private colonoscopist's fee (which is very likely). Reliance on the private sector may discriminate against those without private health insurance (55% of all Australians) 37 as colonoscopy waiting times are often longer in the public sector [A38, A39].
Quality of Colonoscopy
The quality of the colonoscopy itself is determined by the training and experience of the colonoscopist and the standard of facilities (personnel and equipment) available. England has established high standards in certification and accreditation procedures, and the other UK countries have largely followed its lead. A recent report from the Australian NBSCP Quality Working Group has recommended the introduction of a national scheme for certification and re-certification of competence in colonoscopy – based on many features of the English model 33 – but applying to all colonoscopy, not just screening. The ‘usual care’ model adopted in Scotland and most of Australia, can lead to difficulties in assessing the quality of screening colonoscopy, which may vary across regions [UK04]. 33
Quality of Data Collection
The quality of data collection is closely related to the programme model. England, Wales and Northern Ireland, where clinical outcomes data are linked to a central register, are much better positioned than Scotland and Australia which rely on this information being forwarded to a central register. In Scotland, the NHS health boards collect clinical data on different IT systems and are responsible for feeding that data back to the central Information Services Division (ISD) within NHS Scotland. Although the health boards are required to deliver the data, they do not always provide all the necessary data in the appropriate form [UK04].
In Australia, the situation is even less co-ordinated. The programmes in all states except Queensland rely on individual clinicians – GPs, colonoscopists and histopathologists – to return data to the central programme register run by Medicare Australia, and the rates of return, particularly by histopathologists, have been poor. 36 England, despite having an efficient data collection system in place, and a programme underway since mid-2006, has not yet published any programme outcomes, although they are expected to be produced annually in the near future [UK05]. The lack of reliable clinical outcomes data from all countries except Scotland has made meaningful comparison of the relative performance of each programme impossible.
Discussion
None of the programmes incorporated all of our proposed optimal features, with different programmes using different combinations of them. Insufficient funding has forced programme administrators to compromise on ideal implementation characteristics. England, with a much larger population, has opted for a less expensive, less accurate test, while Australia uses a more expensive, more accurate test, but only offers testing to three select age groups: 50, 55 and 65. It is clear that a trade-off between accuracy of test (and cost) and population coverage has been considered necessary in both settings. In contrast, Scotland is the only country to offer screening to the ideal age range of 50–74, as it has prioritized a philosophical commitment to age-based equity [UK03] over offering a more accurate (and expensive) test to a more restricted age range. These kind of trade-offs are necessary in all five countries because governments have baulked at the upfront costs of offering an optimal bowel cancer screening programme.
For example, the Australian Government has made a continuing commitment to fund biennial breast and cervical cancer screening programmes for all women in the recommended age ranges (50–69 for breast cancer; 18–69 for cervical cancer). Bowel cancer kills more people each year than each of these cancers combined, and FOBT screening has consistently been reported to be highly cost-effective.5–6,24,38 Yet the Australian Government appears to be weighting short-term costs more heavily than the potential future cost savings and improved health outcomes.
Limitations of this study include the fact that the seven most salient programme characteristics and some of our proposed optimal features are based on our detailed examination of the different programmes and our considered opinion about what appears to work best. This has been necessary because of the paucity of clinical outcomes data available to support all of our assertions.
Further research could explore the potential efficiency gains of having one central funding source for all cancer screening, and redistributing funding according to relative cost-effectiveness.
Conclusion
This review raises the broader question of the role of evidence in policy and practice, by demonstrating the clear link between funding and evidence-based practice. All five bowel cancer screening programmes are being delivered in different, but potentially inefficient, ways. The irony is that by delivering programmes that do not optimize operational efficiency, governments may not be achieving the net health benefits of FOBT screening that justified the initial decision to fund them in the first place.
Footnotes
![]() . KF, KH, SC, GS and LT declare no support from any organization for the submitted work, no financial relationships with any organizations that might have an interest in the submitted work in the previous three years, and no other relationships or activities that could appear to have influenced the submitted work.
. KF, KH, SC, GS and LT declare no support from any organization for the submitted work, no financial relationships with any organizations that might have an interest in the submitted work in the previous three years, and no other relationships or activities that could appear to have influenced the submitted work.
JSJ receives a sitting fee for one or two meetings each year as a member of the Program Advisory Group and as chair of the Quality Working Group for the Australian National Bowel Cancer Screening Program. He has no involvement with financial aspects of the Programme. MP was the recipient of a Packer Policy Fellowship from the Australian Government Department of Health and Ageing in 2010.
Acknowledgements
The authors wish to thank the key informants who generously gave their time to provide valuable insights into the implementation of these bowel cancer screening programmes, and the programme correspondents who so helpfully provided additional unpublished data.
Appendix A: Programme Models Within Australia
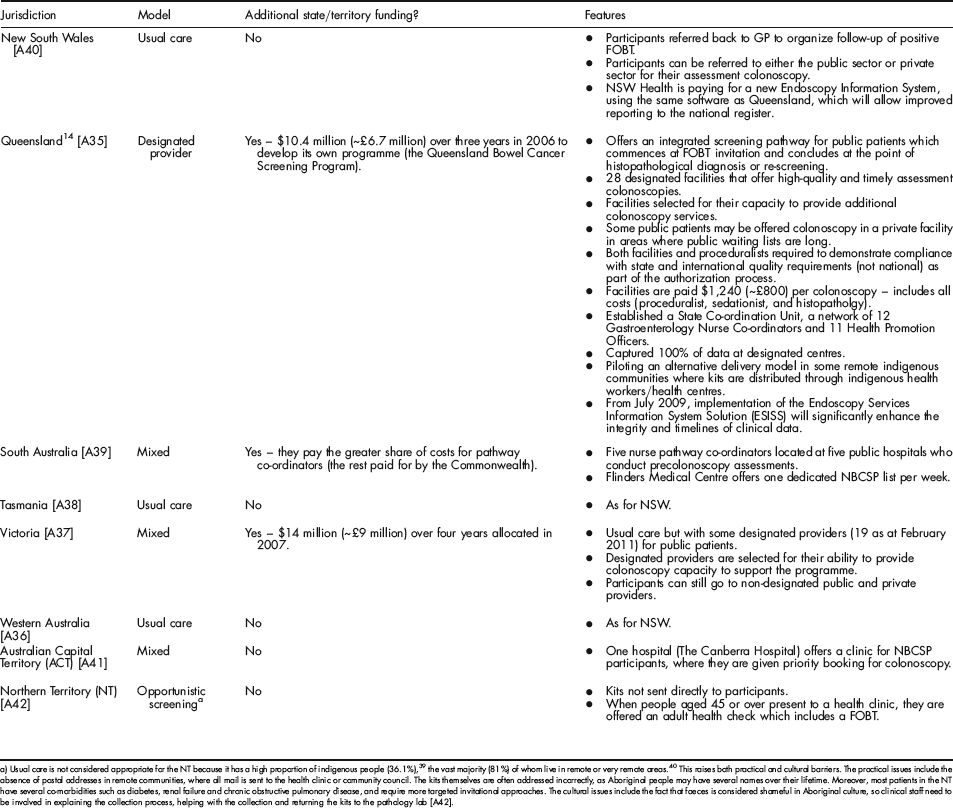
| Jurisdiction | Model | Additional state/territory funding? | Features |
|---|---|---|---|
| New South Wales [A40] | Usual care | No | • Participants referred back to GP to organize follow-up of positive FOBT. |
| • Participants can be referred to either the public sector or private sector for their assessment colonoscopy. | |||
| • NSW Health is paying for a new Endoscopy Information System, using the same software as Queensland, which will allow improved reporting to the national register. | |||
| Queensland 14 [A35] | Designated provider | Yes – $10.4 million (∼£6.7 million) over three years in 2006 to develop its own programme (the Queensland Bowel Cancer Screening Program). | • Offers an integrated screening pathway for public patients which commences at FOBT invitation and concludes at the point of histopathological diagnosis or re-screening. |
| • 28 designated facilities that offer high-quality and timely assessment colonoscopies. | |||
| • Facilities selected for their capacity to provide additional colonoscopy services. | |||
| • Some public patients may be offered colonoscopy in a private facility in areas where public waiting lists are long. | |||
| • Both facilities and proceduralists required to demonstrate compliance with state and international quality requirements (not national) as part of the authorization process. | |||
| • Facilities are paid $1,240 (∼£800) per colonoscopy – includes all costs (proceduralist, sedationist, and histopatholgy). | |||
| • Established a State Co-ordination Unit, a network of 12 Gastroenterology Nurse Co-ordinators and 11 Health Promotion Officers. | |||
| • Captured 100% of data at designated centres. | |||
| • Piloting an alternative delivery model in some remote indigenous communities where kits are distributed through indigenous health workers/health centres. | |||
| • From July 2009, implementation of the Endoscopy Services Information System Solution (ESISS) will significantly enhance the integrity and timelines of clinical data. | |||
| South Australia [A39] | Mixed | Yes – they pay the greater share of costs for pathway co-ordinators (the rest paid for by the Commonwealth). | • Five nurse pathway co-ordinators located at five public hospitals who conduct precolonoscopy assessments. |
| • Flinders Medical Centre offers one dedicated NBCSP list per week. | |||
| Tasmania [A38] | Usual care | No | • As for NSW. |
| Victoria [A37] | Mixed | Yes – $14 million (∼£9 million) over four years allocated in 2007. | • Usual care but with some designated providers (1 9 as at February 2011) for public patients. |
| • Designated providers are selected for their ability to provide colonoscopy capacity to support the programme. | |||
| • Participants can still go to non-designated public and private providers. | |||
| Western Australia [A36] | Usual care | No | • As for NSW. |
| Australian Capital Territory (ACT) [A41] | Mixed | No | • One hospital (The Canberra Hospital) offers a clinic for NBCSP participants, where they are given priority booking for colonoscopy. |
| Northern Territory (NT) [A42] | Opportunistic screening a | No | • Kits not sent directly to participants. |
| • When people aged 45 or over present to a health clinic, they are offered an adult health check which includes a FOBT. |
Usual care is not considered appropriate for the NT because it has a high proportion of indigenous people (36.1%), 39 the vast majority (81%) of whom live in remote or very remote areas. 40 This raises both practical and cultural barriers. The practical issues include the absence of postal addresses in remote communities, where all mail is sent to the health clinic or community council. The kits themselves are often addressed incorrectly, as Aboriginal people may have several names over their lifetime. Moreover, most patients in the NT have several co-morbidities such as diabetes, renal failure and chronic obstructive pulmonary disease, and require more targeted invitational approaches. The cultural issues include the fact that faeces is considered shameful in Aboriginal culture, so clinical staff need to be involved in explaining the collection process, helping with the collection and returning the kits to the pathology lab [A42].