
Abstract
Objectives
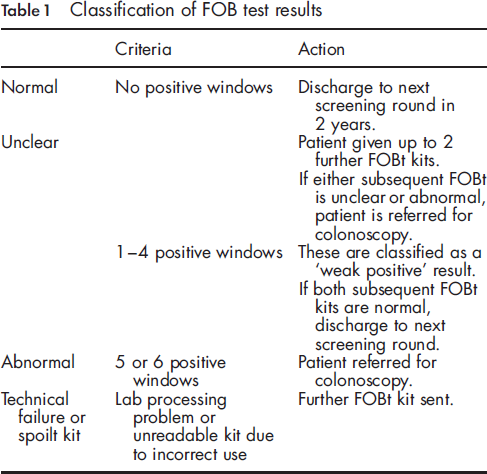
The UK National Health Service Bowel Cancer Screening Programme (BCSP) is based on a strategy of biennial faecal occult blood (FOB) testing. Positive results are classified as ‘abnormal’ or ‘weak positive’ based on the number of positive windows per kit or need for repeat testing. Colonoscopy is offered to both groups. We evaluate the relationship between FOB test positivity and clinical outcome in the BCSP.
Setting
The South of Tyne and Tees (UK) Bowel Cancer Screening Centres.
Methods
Data were collected prospectively on all individuals who were offered FOB testing and colonoscopy between February 2007 and February 2009. Univariable and multivariable analyses were performed to investigate the relationship between FOB test positivity and clinical outcome.
Results
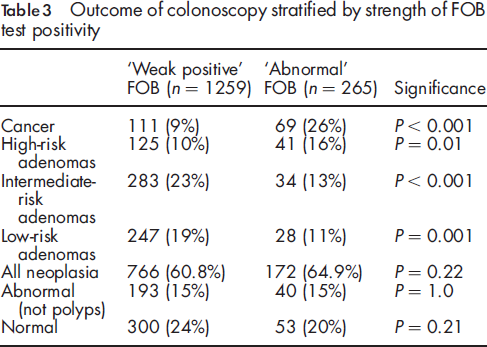
Following FOB testing, 1524 individuals underwent colonoscopy, 1259 (83%) after a ‘weak positive’ and 265 (17%) an ‘abnormal’ result. Cancer was detected in 180 (11.8%) and adenomas in 758 (49.7%). Individuals with an ‘abnormal’ result were more likely to have cancer or be ‘high risk’ for the development of future adenomas (110/265, 41.5%) than those with ‘weak positive’ results, (236/1259, 18.7%, P < 0.0001). Those with Dukes stage B, C or D cancers or cancers proximal to the splenic flexure were more likely to have an ‘abnormal’ result.
Conclusions
The majority of colonoscopies were performed following ‘weak positive’ FOB results. Those with an ‘abnormal’ result were more likely to be diagnosed with cancer. The high yield of pathology in both the ‘abnormal’ and ‘weak positive’ groups justifies the need for colonoscopy in both.
Introduction
Randomized controlled trials have demonstrated the efficacy of population-based faecal occult blood (FOB) testing in reducing mortality from CRC by 13 to 16%.5, 6 The UK pilot study of population-based CRC screening commenced in 2000. 7 Screening was undertaken using a non-rehydrated guaiac-based FOB test offered to 50-69-year-old adults. The overall positivity rate of the FOB test was 1.9% with the majority requiring repeat FOB testing. Colonoscopy uptake rate was 81.5%. The overall positive predictive value of a positive FOB test result was 10.9% for CRC and 35.0% for adenomas.
Classification of FOB test results
This study examines the association between FOB test positivity and clinical outcome in the BCSP.
Methods
Study population
The South of Tyne and Tees Bowel Cancer Screening centres are two first wave centres in the North East of England covering a combined population of approximately 1,500,000. Both centres are part of the Northern Region Endoscopy Group (NREG). This organization provides the framework for collaborative endoscopy-related research. Both centres commenced screening in February 2007 and completed prevalent round screening two years later.
Data collection
Data were collected prospectively on all individuals who were offered FOB testing in both screening centres. These included data on uptake of the screening test and results of the individual's FOB test results. Patients were divided into two groups according to whether they had an ‘abnormal’ or ‘weak positive’ FOB result.
Data were also collected on all individuals undergoing colonoscopy following a positive FOB result. These data were recorded at the time of the individual's attendance at the screening clinic or during the colonoscopy itself and included demographic details (age, gender) and colonoscopic findings. Clinical outcomes (including adenoma profile and cancer staging) were subsequently recorded using histological data from the local pathology database. Individuals in whom adenomas or cancer were not detected were classified as either ‘normal’ or ‘abnormal not polyps’ if an alternative diagnosis such as colitis or diverticular disease was made.
FOB testing
FOB testing was performed using a non-rehydrated guaiac-based FOB kit (Hema-screen, Immunostics, Inc.) No dietary restriction is required prior to completion. Individuals receive the kit by mail and, after completion, return it by mail to the screening hub in the World Health Organisation (WHO) approved postage paid envelope provided within 14 days of the first sample. When repeat testing is required, this is performed within 13 weeks of the previous test. All FOB kits are assessed on the day they are received at the hub by trained individuals. Quality assurance consists of continuous internal and external assessment for both FOB kits and kit readers to ensure that standards remain high.
Colonoscopist accreditation
All colonoscopies were performed by BCSP accredited colonoscopists. BCSP accreditation requires the colonoscopist to have a lifetime experience of over 1000 colonoscopies prior to commencing screening and to meet nationally agreed standards for adenoma detection rate, intubation rate and complications. In addition the colonoscopist must pass a knowledge-based assessment and directly observed procedure examination. Ongoing audit of practice is mandatory to ensure high-quality colonoscopy within the programme is maintained.
Pathology analysis
Histological examination of polyps and other endoscopic specimens were undertaken at three histopathology laboratories accredited by Clinical Pathology UK Ltd. in accordance with BCSP guidelines. Pathological examination of surgically resected tumours was completed using the RCPath dataset. 9
Data analysis
Univariable analyses were conducted using the χ 2 test. A P value of less than 0.05 was considered significant. Positive predictive values are calculated using the number of individuals with the relevant test result who underwent colonoscopy as the denominator and are presented with 95% confidence intervals (CI). Data were analysed using SPSS version 17.0® (SPSS Inc., Chicago, Illinois, USA).
Results
Between February 2007 and February 2009, 195,772 individuals were offered FOB screening with an uptake of 54%. FOB test positivity rate was 1.7%, comprising 18.9% with an ‘abnormal’ result and 81.1% with a ‘weak positive’ result. A total of 1668 patients were referred for colonoscopy, of whom 1524 individuals (91.0%) agreed to undergo the procedure.
A total of 1259 of 1524 (83%) patients underwent colonoscopy for a ‘weak positive’ FOB result and 265 of 1524 (17%) patients had an ‘abnormal’ FOB test result.
Bowel cancer was detected in 180 of 1524 (11.8%) patients. Histological and clinical staging was available for 171 of 180 (95%) cases at the time of analysis. Location of the cancer was available for all but one case.
Of 171 cancers, 72 (42%) cancers were Dukes A at diagnosis including 32 polyp cancers; 46 (27%) were Dukes B; 47 (27%) Dukes C; and 6 (4%) were Dukes D. The majority (146 of 179, 82%) of cancers were found at or distal to the splenic flexure.
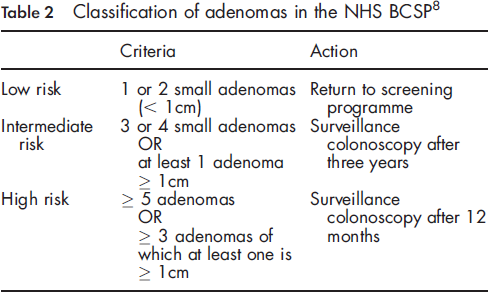
Adenomas were detected in 758 of 1524 individuals (49.7%). Eleven percent of individuals were classified as ‘high risk’, 21% ‘intermediate risk’ and 18% ‘low risk’ according to the BSG adenoma surveillance guideline classification (Table 2). 8
FOB result
Outcome of colonoscopy stratified by strength of FOB test positivity
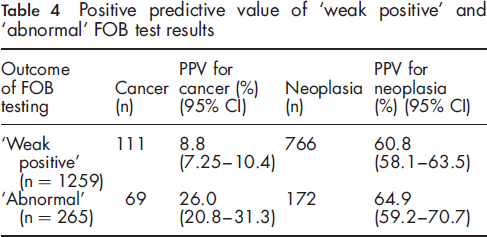
Positive predictive value of ‘weak positive’ and ‘abnormal’ FOB test results
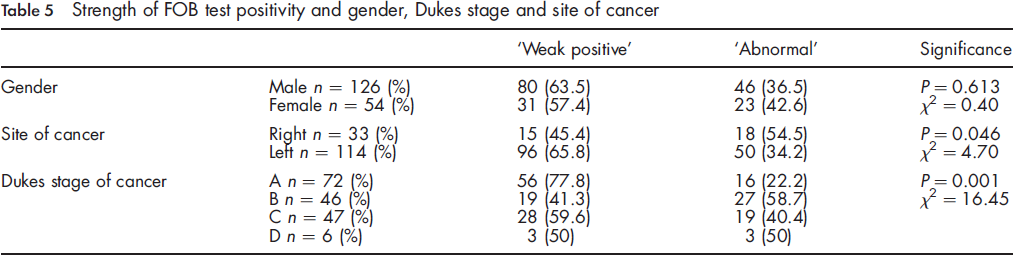
Strength of FOB test positivity and gender, Dukes stage and site of cancer
Strength of FOB test positivity and Dukes stage of cancer sub-grouped by site
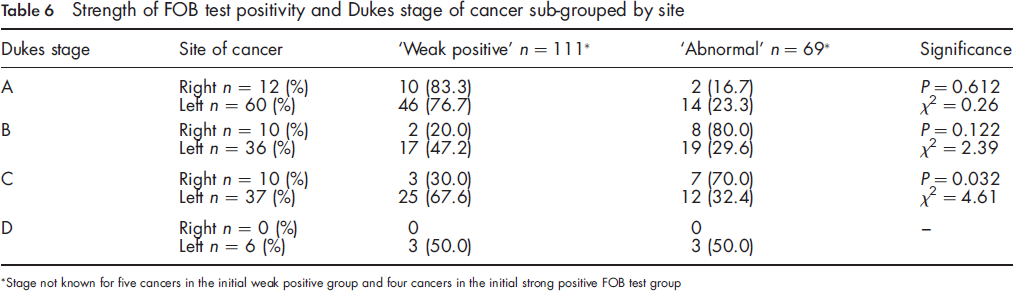
Stage not known for five cancers in the initial weak positive group and four cancers in the initial strong positive FOB test group
Discussion
Uptake of FOB testing and FOB test positivity in this study were comparable with those in the UK Colorectal Cancer Screening Pilot. 7 Cancer diagnosis rate and stage at diagnosis were also comparable with previously published data from the BCSP. 10 A marked shift in stage at diagnosis toward Dukes A cancers compared with the Dukes stage profile of non-screen detected cancers is observed. 1
The majority of colonoscopies were performed following ‘weak positive’ FOB results as opposed to ‘abnormal’ FOB results (83% vs. 17%). Those with an ‘abnormal’ result were more likely to be diagnosed with cancer at screening colonoscopy than those with a ‘weak positive’ result (26% vs. 9%, P = 0.008). This suggests that patients with an ‘abnormal’ FOB result have around a one in four chance of having cancer detected at colonoscopy compared with one in eleven for those with a weak positive FOB result. Those with a ‘weak positive’ result, as well as being the majority, also have a high rate of pathology detected at colonoscopy confirming the importance of colonoscopy in this group. These data may allow more precise explanation of risk of cancer diagnosis to be presented to patients unsure of the need to proceed to colonoscopy following FOB testing.
These data are comparable with the second round of the UK screening pilot in which no dietary restriction was recommended during FOB retesting. 11 In the pilot study, the positive predictive value (PPV) of a strong positive FOB result (analogous to the ‘abnormal’ classification in this study) for cancer was 18.2% compared with 5.3% following repeated testing (analogous to the ‘weak positive’ classification in this study). For all neoplasia the PPVs were 42.1% and 28.6% respectively. The PPV for adenomas was lower in the strong positive group than the repeat test group (23.9% vs. 28.6% respectively). Our results show a similar pattern but with a universally higher rate of neoplasia and less of a difference between total neoplasia rates between the two groups (60.8% vs. 64.9%, P = 0.22). This is due to a number of factors, the most important being the wider age range (50-69 years) in the pilot study. Other potential factors include differences in neoplasia prevalence in the underlying population and differences in colonoscopic technique.
Right-sided cancers were more common in those with an ‘abnormal’ FOB result than with a ‘weak positive’ FOB result. The effect of site of cancer on FOB test positivity may be explained by the differing stage distribution of right- and left-sided cancers. Dukes A cancers were more common in the left colon whilst right-sided cancers tended to be more advanced. It is likely that more advanced cancers bleed more frequently and in larger quantities than early cancers, increasing the chance of producing an ‘abnormal’ FOB result. A second factor which may increase the chance of a right-sided cancer giving an ‘abnormal’ FOB result is the mixing of blood throughout the stool during transit from the right colon, which may increase the chance of five or six windows on the FOB test being positive. A third possibility is that right-sided cancers differ biologically to left-sided cancers12, 13 and this affects tendency of the lesion to bleed.
There has been considerable discussion recently regarding the ability of colorectal cancer screening programmes to detect right-sided cancer. A large Canadian community-based study did not show any protective benefit from undergoing screening colonoscopy against death from right-sided colorectal cancer. 14 The UK randomized trial of FOB testing demonstrated a similar reduction in mortality from right-and left-sided cancer. 15 Our study suggests that FOB testing and high-quality colonoscopy are capable of detecting right-sided cancers. The ability of FOB testing to detect asymptomatic right-sided cancers will become ever more important with the rollout of flexible sigmoidoscopy screening.
An important consideration is that these data are from the prevalent round of screening. It is likely that the cancer detection rate will change in subsequent incident screening rounds and further work is needed to examine these factors in the future.
In conclusion, most people undergoing screening colonoscopy will do so on the basis of a ‘weak positive’ FOB result. The high yield of cancer seen in this study justifies the need for colonoscopy in both individuals with ‘abnormal’ and ‘weak positive’ FOB results. Those with an ‘abnormal’ FOB test are more likely to be diagnosed with cancer but overall detection of neoplasia is not significantly different between the two groups.
Footnotes
Acknowledgements
This paper was prepared in association with the Northern Region Endoscopy Group (NREG). We acknowledge I Ward, G Hanley, J Henry, S Panter, N Dempsey, C Taylor, J Singh, J Painter, L Hurst and J Bowes for their involvement in data collection and analysis.