
Abstract
Background
Group B streptococcus (GBS) is a leading cause of severe infections in newborns. Intrapartum antibiotic chemoprophylaxis (IAP) reduces the rate of early-onset disease. The aim of this study is to determine the degree of clinicians’ compliance with the suggested protocol for GBS prevention in Emilia-Romagna (Italy).
Methods
Characteristics of each delivery were prospectively recorded in the period between October 2005 to December 2005. Standardized proforma were used to collect data.
Results
Among 5118 babies, 7.2% (369) were preterm and 92.3% were born at term (4749). Antenatal screening was performed in 86.6% of women who delivered at term, of which 18.1% were GBS culture-positive. Information regarding culture site was available in 93.2% of women screened and recto-vaginal cultures were documented in 42.7%. IAP was administered to 28.7% of 3937 women at term who had either spontaneous delivery or emergency caesarean section. In this cohort, 15.9% were diagnosed GBS culture-positive, of which 92.6% received IAP. Prophylaxis was also administered to 8.4% (331) of women for no apparent reason. Compared with tertiary level hospitals, women delivering in primary/secondary hospitals were more likely to be both GBS screened (P < 0.0001; OR 3.04; CI 2.33-3.97) and to receive prophylaxis ≥4 hours before delivery (P = 0.0025; OR 1.57; CI 1.17-2.12).
Conclusions
GBS screening was performed in > 85% of women and > 90% of culture-positive women received prophylaxis. However, there is a need to educate clinicians about protocol adherence, as most cultures were suboptimal and cases of unnecessary IAP were administered. The screening was more effective in hospitals with fewer deliveries.
Introduction
There are two main GBS prevention strategies: the culture- and the risk-based approaches.3, 4 The former suggests that IAP be offered either to women identified as GBS colonized in late pregnancy (35-37 weeks of gestation) or to women with clinical risk factors, which include GBS-bacteriuria during the current pregnancy or a previous GBS-infected infant. With the risk-based approach, IAP is administered to women with identified risk factors: preterm delivery (< 37 weeks gestation), prolonged rupture of membranes (ROM, ≥ 18 hours) and intrapartum maternal fever ≥ 38° C.
A multistate retrospective cohort study published in 2002 found that the culture-based approach prevented more cases of early-onset disease than the risk-based approach. 5 Interestingly, a similar amount of antibiotic administration was used in both strategies, thereby carrying a similar risk of chemoprophylaxis adverse effects.
On the basis of these results, the Centre for Disease Control and Prevention (CDC) in the USA endorsed guidelines in 2002 which recommend the adoption of universal prenatal screening. 3 The implementation of this strategy resulted in a further 27% decrease in the early-onset disease incidence after guidelines were issued (from 0.47 cases/1000 live births in 1999-2001 to 0.34 cases/1000 live births). 6
Individual practices and compliance with protocols for GBS prevention are rarely reported, and those available are mainly carried out through questionnaires, which are unreliable indicators of actual clinical practices. 7 13 Reliable information is essential to identify where additional public health prevention measures should be implemented.
In 2001 a GBS Prevention Working Group was set up in Emilia-Romagna, a region with a population of about 4,500,000, registering around 40,000 live births per year. The group promoted the culture-based approach, developing common protocols which were adopted among all the group healthcare providers. 14 In this region the incidence of culture-proven early-onset disease is 0.28/1000 live births. 15
However, the implementation of this strategy could be associated with insufficient adherence to recommendations or with outcomes that were neither intended nor desirable.
This prospective cohort study aims to determine the degree of clinicians’ compliance with the suggested protocol among the regional maternity units.
Methods
Study design
Antenatal GBS screening has been in place in all regional delivery units in Emilia-Romagna since 2003. 16 Maternity units were invited to participate in a prospective cohort study and were asked to record each delivery during a three-month consecutive period (October-December, 2005). Eleven centers, accounting for more than a half of regional births, participated in the study.
Trained abstractors collected standardized information to describe maternal and infant characteristics, including antenatal GBS screening, culture sites, risk factors, gestational age, delivery mode, administration of intrapartum chemoprophylaxis.
Administration of prophylaxis
According to CDC guidelines, 3 our protocol recommends recto-vaginal screening cultures at 35-37 weeks of gestation and optimal culture techniques (selective broth media). Penicillin is the recommended intrapartum chemoprophylaxis agent 3 but, as it is not produced in Italy, ampicillin is routinely administered. The regional protocol recommends a standard dose of ampicillin (2 g intravenously plus 1 g intravenously every 4 hours until delivery) during active labour to women GBS screened culture-positive; to women without screening results and risk factors, or to women with intrapartum fever.
Cefazolin is recommended for women with documented penicillin/ampicillin allergy without a consistent risk for anaphylaxis. If the GBS isolates are susceptible, erythromicin or clindamicin are recommended for women with high risk for penicillin/ampicillin anaphylaxis. 3
According to the CDC recommendations, prophylaxis is adequate only if administration of penicillin/ampicillin begins at least four hours prior to delivery.
Prophylaxis is not recommended for women with planned caesarean section in the absence of membrane rupture or the initiation of labour. 3
Statistical methods
Statistical analysis was performed according to the χ2 test and analysis of variance when appropriate. A P value < 0.05 was used as a threshold for statistical significance and 0.10 < P < 0.05 as an indication of a trend.
Results
In Emilia-Romagna, according to Regional Health Agency hospital discharge charts, there were 38,855 deliveries in 2005. During the study three-month period, 5,349 deliveries were recorded by participating centres. Due to incomplete data, 231 cases (4.3%) were excluded.
Delivery, antenatal GBS screening and IAP administration characteristics of preterm and at term deliveries
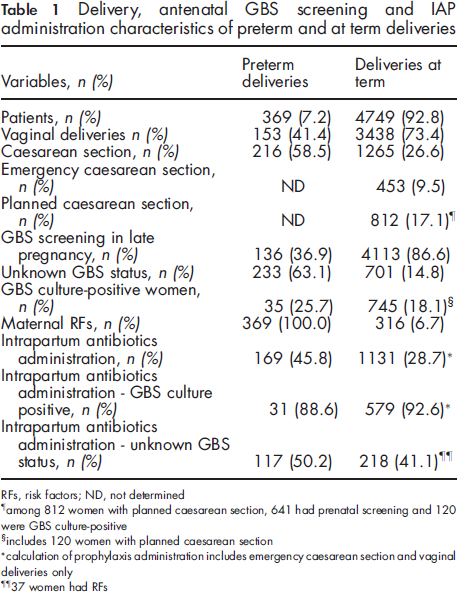
RFs, risk factors; ND, not determined
among 812 women with planned caesarean section, 641 had prenatal screening and 120 were GBS culture-positive
includes 120 women with planned caesarean section
calculation of prophylaxis administration includes emergency caesarean section and vaginal deliveries only
37 women had RFs
Colonization rates in maternity unit, divided according to hospital level

Compliance with the intrapartum chemoprophylaxis administration for maternity units (%), according to hospital level ¥
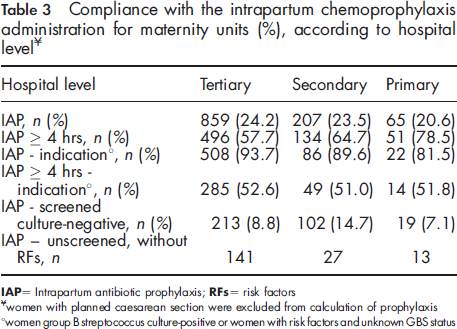
IAP = Intrapartum antibiotic prophylaxis; RFs = risk factors
Women with planned caesarean section were excluded from calculation of prophylaxis
Women group B streptococcus culture-positive or women with risk factors and unknown GBS status
Among the 11 participating maternity units, six were tertiary level, three were secondary and two were primary level hospitals.
Colonization status
The colonization status of individual participating maternity units is illustrated in Table 2. Antenatal GBS screening was performed in 86.6% of 4,113 women (range 74.9-97.8%) and the screening results were known at hospital admission in 97.0% of cases. Women who were screened GBS culture-positive were 18.4% (range 11.5-38.5%).
Women who delivered at primary/secondary level hospitals were more likely to receive GBS antenatal screening (χ 2 = 77.1; P < 0.0001, odds ratio (OR) 3.04; confidence interval (CI) 2.33-3.97) with respect to women delivering at tertiary hospitals.
Information on culture site was available in 93.2% of 4,113 women (n = 3,834) and recto-vaginal cultures were documented in 42.7% of cases (n = 1,637) (Table 2). The remaining specimens were collected at the vaginal site only. Recto-vaginal cultures were performed in < 10% of cases in five maternity units. No significant difference was found between primary/secondary and tertiary hospitals for rates of recto-vaginal cultures.
Identified rates of colonization were significantly higher (χ 2 = 132.1; P = 0.0001; OR 2.54; CI 2.15-3.0) in centres which performed the screening in at least 50% by means of recto-vaginal instead of solely vaginal cultures.
Intrapartum chemoprophylaxis administration
Women who received antibiotics during planned caesarean section were excluded from this analysis, as IAP is not recommended even for GBS culture-positive women.
3
Thus, prophylaxis was administered in 28.7% of 3,937 women who either had a vaginal delivery or an emergency caesarean section (Table 3, Figure 1).
Mode of delivery, GBS status, prophylaxis administration and risk factors among women at term. VD= vaginal delivery; ECS= emergency caesarean section; PCS= planned caesarean section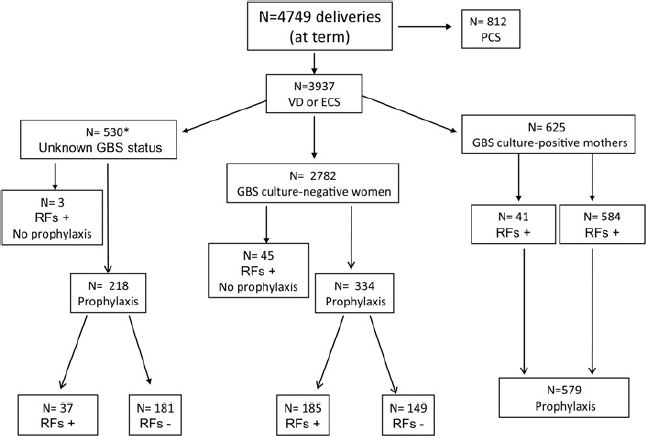
Prophylaxis was administered at least four hours before delivery in 63.2% of 1,131 women (range 46.5-79.2%). Women delivering at primary/secondary hospitals were more likely to receive prophylaxis > 4 hours before delivery (χ 2 = 9.14; P = 0.0025; OR 1.57; CI 1.17-2.12) with respect to those delivering at tertiary hospitals.
Prophylaxis was administered in 93.1% of 665 women with an indication for prophylaxis requirement (range 75.0-95.2%, Table 3). Among these cases, adequate ampicillin (≥ 4 hours before delivery) was administered in 52.0% of 579 GBS culture-positive women (n = 346) and in 62.2% of the 37 women with unknown GBS status and risk factors (n = 23).
Alternative agents to ampicillin were administered during labour to 10.5% of 1,131 women.
Prophylaxis was also administered to 34.2% of 530 GBS unscreened women without risk factors and to 5.4% of 2,782 women without risk factors who were screened GBS culture-negative.
Discussion
This is the first prospective study evaluating the adherence to GBS protocol specific recommendations. Our data show that universal screening has been successfully implemented in Emilia-Romagna. Indeed, more than 86% of women at term were screened in good time, 97% had a documented result at delivery and most women who had an indication for treatment received prophylaxis.
Antenatal screening was more likely to be performed at hospitals with fewer deliveries and women who were screened in the recto-vaginal, rather than vaginal site only, were more likely to be GBS colonized. However, greater than 50% of the screening cultures were suboptimal, as they were collected in the vaginal site only. This finding may partly explain why most residual early-onset disease cases registered in Emilia-Romagna are associated with the culture detection failure of organisms at 35-37 weeks of gestation. 15
Recently the screening strategy has been evaluated in surveillance areas of the USA.17, 18 During 2003-2004, most women (85%) were prenatally screened, but only 49-74% were screened at the recommended 35 or more weeks of gestation. During the same period most early-onset disease cases were registered in infants born to women who were screened GBS culture-negative. Authors could not evaluate if some negative test results were attributed to improper collection techniques or the use of non-selective media. Proper collection of specimens and use of optimal culture techniques are crucial steps for the success of this strategy.
Further, Goins et al. 18 reported that an appropriate agent (penicillin, ampicillin, cefazolin or vancomycin) was administered ≥ 4 hours before delivery in 61% of cases. Comparable rates of ≥ 4 hours prophylaxis duration have been reported elsewhere.19, 20 The proportion of women who fail to receive the required four-hour duration of IAP is therefore relevant in these studies.
In the current study, most women (93.1%) with an indication for prophylaxis received IAP but, among them, ampicillin was administered ≥ 4 hours before delivery in 52.0% of women only. Interestingly, the achievement of ≥ 4 hours prophylaxis duration was significantly more frequent at hospitals with fewer deliveries.
However, unnecessary intrapartum antibiotics may be an unintended consequence of prophylaxis. In this study 12.0% of culture-negative women and 34.2% of women with unknown GBS status without any risk factors received prophylaxis. The most common, not protocol specified reasons, were membrane rupture > 12 hours or unknown GBS status at delivery. An improved provider familiarity with the screening recommendations is needed, as the increased use of antibiotics in the perinatal period could select penicillin-resistant organisms. 21
This study has several limitations. Less than 50% of delivery units participated in this survey. Therefore our data may not be representative of the entire region, reflecting practices of more compliant maternity units. However, participating units account for > 50% regional deliveries and we included urban counties as rural areas.
Further, the rate of GBS bacteriuria may have been underestimated, since urine culture was not a standard practice of antenatal care in 2005.
In conclusion, these data show that culture strategy was correctly addressed in the vast majority of women at risk, being more effective at hospitals with fewer deliveries. However, there is a need to further educate healthcare providers about the strict protocol adherence, as cultures were often suboptimal and unnecessary intrapartum antibiotics were administered. The efficacy of this strategy, as well as protocol deviations, should be reassessed periodically.
Footnotes
Acknowledgments
We thank Dr Johanna Chester, who kindly revised the manuscript and gave valuable suggestions