
Abstract
Objectives
To assess whether pre-notification is effective in increasing uptake of colorectal cancer screening for all demographic groups.
Setting
Scottish national colorectal cancer screening programme.
Methods
Males and females aged 50-74 years received a faecal occult blood test by post to complete at home. They were randomized to receive in addition: the pre-notification letter, the pre-notification letter + information booklet, or the usual invitation. Overall, 59,953 subjects were included in the trial between 13/04/09 and 29/05/09 and followed to 27/11/09. Pre-notification letters were posted two weeks ahead of the screening test kit. Uptake was defined as the return of a screening test and chi-squared tests compared uptake between the trial arms. Logistic regression assessed the impact of the letter and letter + booklet on uptake independently of gender, age, deprivation and screening round.
Results
Uptake was higher with both the letter (59.0%) and the letter + booklet (58.5%) compared with the usual invitation (53.9%, p < 0.0001). This increased uptake was seen for males, females, all age groups and all deprivation categories including least deprived females (letter 69.9%, usual invitation 66.6%) and most deprived males (42.6% vs. 36.1%), the groups with the highest and lowest levels of uptake respectively in the pilot screening rounds conducted prior to the roll out of the programme. Uptake with the pre-notification letter compared with the usual invitation was higher both unadjusted and adjusted for demographic factors (odds ratio 1.24, 95% CI 1.193-1.294).
Conclusions
Pre-notification is an effective method of increasing uptake in colorectal cancer screening for both genders and all age and deprivation groups.
Introduction
Pre-notification has cost implications for a screening programme and it is important to know whether a letter needs to be sent to all those invited for screening or whether a more targeted approach would be equally effective. In the Scottish programme people are invited for screening every two years but there is no information as to whether pre-notification has the same impact when people are invited for their first screening round as when they are invited in subsequent rounds. Most notably there is no information on the effect of pre-notification in colorectal cancer screening by gender, age and deprivation, all of which are known to independently influence uptake. 5 If the impact of pre-notification differs among demographic groups and the affluent respond better, then it could potentially exacerbate the unequal uptake commonly seen in cancer screening.
Focus groups evaluating the Scottish programme have highlighted the large quantity of printed material that accompanies the screening test kit as a potential barrier to engaging with the programme and to the detriment of uptake. 6 This material includes a substantial booklet, ‘Know the facts’, which plays an important role in helping individuals make an informed choice whether to proceed with colorectal cancer screening. Delivery of this booklet prior to the screening kit, however, could lessen the burden of printed material. A randomized controlled trial was therefore carried out with the aims of assessing the impact of pre-notification on the screening population overall, among first and subsequent invitations and by gender, age and deprivation. Use of a pre-notification letter and also with the additional delivery of the booklet, ‘Know the facts’, prior to the delivery of the screening test kit was compared with current standard practice.
Methods
Participants in the national screening programme in Scotland consist of all residents aged 50-74 years who have a Community Health Index Number (a unique patient identifier) that is associated with an NHS Board. They are sent a guaiac FOBT by post to complete at home and then return to the laboratory at the Scottish Bowel Screening Centre in Dundee for analysis.
The screening programme had been rolled out to 10 of the 14 Scottish NHS Boards at the time of the study. One of these 10 had taken the decision to send their own pre-notification letter and therefore did not take part in the study. All other people who were invited to take part in the screening programme during the study period were included.
Timing of items sent to individuals in each group
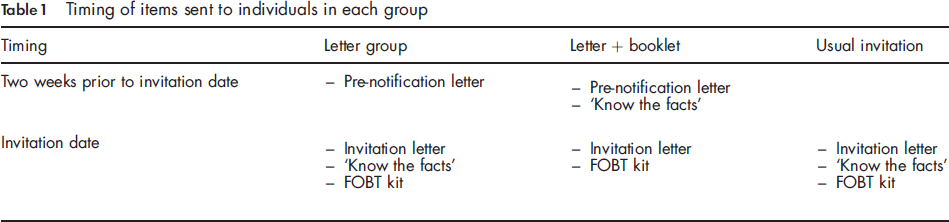
The randomization scheme of simple random sampling was computer generated within the IT system which governs the screening programme and which identifies when individuals are to be invited to participate.
The IT system electronically generates the appropriate mailing packages to be sent out to each individual and during the study period this was done according to the predetermined randomization scheme. The process of generating and mailing the FOBT kits with the appropriate printed information is fully automated therefore blinding the researchers to the allocation of the intervention to individuals.
At the end of the study period, a download of the data generated by the trial subjects was passed to NHS National Services Scotland in Edinburgh where a national deprivation score and a variable to indicate first or subsequent invitation were attached. The dataset was then anonymized and returned to the screening centre for analysis.
Invitees were not informed that they were taking part in a randomized study.
Sample size
Calculations showed that a sample of 60,000 subjects, (20,000 randomized to the letter group, 20,000 randomized to the letter + booklet group and 20,000 to the usual invitation) would enable an increase in uptake of between 3% and 5% to be detected in all social deprivation groups with 80% power at the 5% level. Deprivation was categorized using the Scottish Index of Multiple Deprivation (SIMD) which identifies small area concentrations of multiple deprivation across Scotland based on income level, employment, health, education, skills and training, housing, geographic access and crime. 7
Pre-notification letter
The pre-notification letter was created after viewing the advance notification letters used in the Australian and English screening programmes and that used in NHS Greater Glasgow and Clyde Breast Screening programme. Guidance on the use of plain English was followed 8 and comments from healthcare and non-healthcare individuals were sought in order to ensure that the letter was easy to read and understand. A copy of the letter is contained in Appendix 1.
Statistical methods
The outcome to be tested was uptake, which for the purpose of the study was defined as the return of a kit to the central laboratory.
Uptake in the trial arms was compared for gender, age group and deprivation and also for those who were receiving a first invitation and those receiving a subsequent invitation for screening. This was determined by the NHS Board of residence of the invitee. Invitees from one of the three NHS Boards which had taken part in the pilot screening rounds were classified as having previously been invited and those from a non-pilot NHS Board as receiving a first invitation for screening.
Uptake was compared using chi-squared tests and a logistic regression was performed to assess the impact of the letter and letter + booklet interventions independently of other factors that could influence uptake.
Results
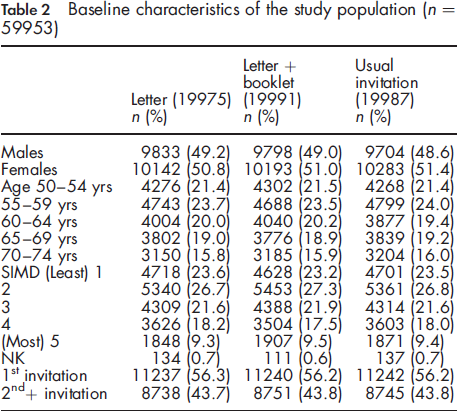
Baseline characteristics
The study population consisted of all 59,953 people from the nine eligible NHS Boards who were sent a screening test kit between 13/04/09 and 29/05/09. They were followed for between 26 and 32 weeks, for the return of their kit to 27/11/09.
Baseline characteristics of the study population (n = 59953)
Uptake
There were 34,249 (57.1%) screening test kits returned of which 88 (0.1%) could not be tested (55 kits had expired, 23 were incomplete, 8 were spoiled and 2 were unused). These 88 people were included in the uptake group in the analysis, since the kits had been returned.
In each of the trial groups, at least 72% of the returned kits had been returned within six weeks and at least 93% had been returned within 12 weeks.
Uptake by gender, age, deprivation and invitation
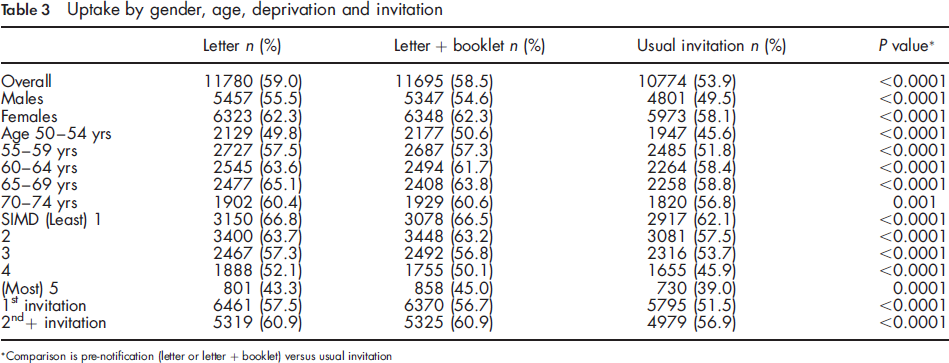
Comparison is pre-notification (letter or letter + booklet) versus usual invitation
Uptake by gender and age and deprivation and gender
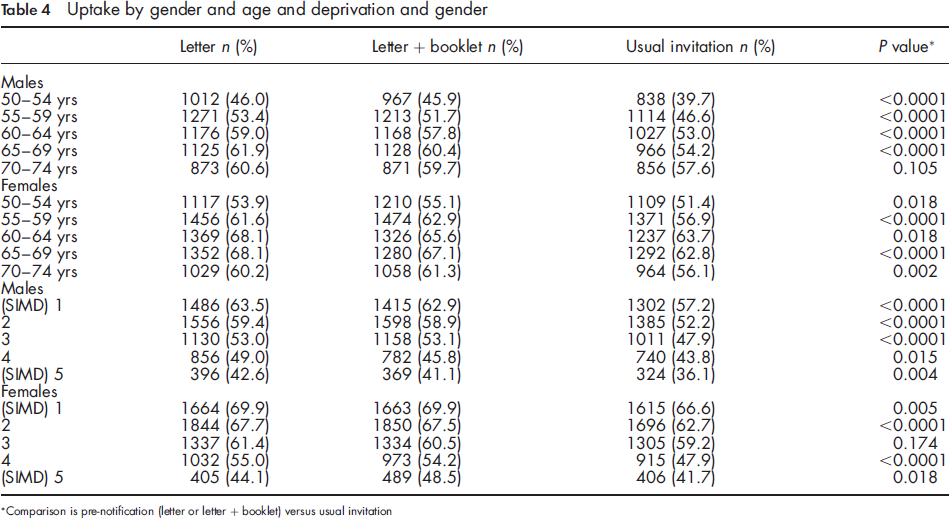
Comparison is pre-notification (letter or letter + booklet) versus usual invitation
Comparing uptake by gender and deprivation (Table 4) showed that, for males, pre-notification increased uptake in each deprivation group including the most deprived, the demographic group with the lowest uptake. For females, pre-notification increased uptake at each deprivation level except for SIMD 3. In the most deprived group, the addition of the booklet increased uptake more than the letter alone (p = 0.05).
Using figures from the first round of the screening pilot in Scotland (2000-2002), it is estimated that the increase in uptake from 54% to 59%, seen with pre-notification, could translate into approximately 11 additional cancers diagnosed per 100,000 of the target population.
Logistic regression
Uptake, unadjusted and adjusted for baseline characteristics
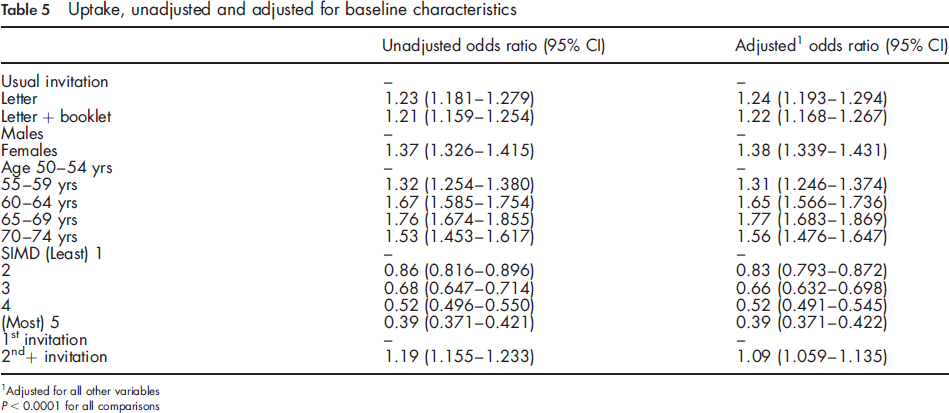
Adjusted for all other variables
P < 0.0001 for all comparisons
Impact of pre-notification on the Screening Centre Helpline
The trial was carried out within the ongoing national screening programme and the Helpline at the Screening Centre documented calls received as a consequence of issuing pre-notification letters. Overall the types of calls were no different from the standard calls. Some callers asked not to be sent the screening test kit as they did not wish or were not able to participate: however, it was not possible to action this due to the set up of the programme.
Discussion
In this study, uptake was significantly higher after a pre-notification letter and a letter + booklet compared with those invited in the usual way. It is of particular note that this increase in uptake was seen not just overall but for both males and females, over all age groups and in all deprivation groups. This included least deprived females and most deprived males, the groups with the highest and lowest uptake respectively in the pilot screening rounds confirming that pre-notification did not increase inequalities in uptake.
The present study has confirmed the findings of an increase in uptake in the Australian trial 2 but with a much larger study population and with the use of guaiac FOBT. Cole et al. did not report their results as odds ratios but, to compare their results directly, an OR of 1.43 (95% CI 1.139-1.801) was calculated from their published figures showing a greater impact of pre-notification in their study. This may have resulted from the comparatively lower uptake in the control group allowing the increase in uptake with pre-notification to have a greater impact on the OR. They reported little change in the effect of pre-notification after adjusting for gender, age and deprivation and our study also showed an independent effect of pre-notification after adjusting for the same variables. The English arm of the screening pilot had routinely used pre-notification but uptake was little different to that in the Scottish arm.3, 4 One difference of the English arm to both our trial and the Australian trial was that the pre-notification letter was sent only one week before the distribution of the screening test kit. The letter also allowed people to opt out of the pilot at that point. This option was not available in our study.
Uptake was also increased when the information booklet was included with the pre-notification letter. This may be an important combination in a screening programme where people can decline the invitation to participate at the time of receiving the pre-notification letter thus allowing them to do so after making a fully informed choice.
Cole et al. 2 suggest the rationale for the effectiveness of pre-notification is based on a health behaviour change model whereby pre-notification moves the individual a step along their pathway between no knowledge of screening and uptake of the test. A further underpinning thesis for this study is the Health Belief Model in which a basic tenet is that cues to action will be successful. 9 Such cues are events, for example, receipt of a pre-notification letter, which can activate the preparedness of individuals to react (participate) and that such a reaction can be estimated in some measurable behaviour, in this context, uptake. The results from this study would be consistent with both these proposed models of behaviour.
Conclusions
This study has clearly shown that pre-notification is an effective method of improving participation in a national programme of colorectal cancer screening in both genders, across all ages and levels of deprivation. It can therefore be recommended to improve the performance of the programme.
Footnotes
Pre-notification letter
Dear
You will soon get an invitation to take part in the Scottish Bowel Screening Programme. Screening is offered to everyone aged 50-74.
Bowel cancer is one of the most common cancers, especially for people over 50. It causes 1,600 deaths in Scotland each year.
The good news is there is a simple test that can help find early signs of bowel cancer. The chances of beating bowel cancer are very high when it is found early.
Your testing kit and information leaflets will arrive in the post in about 2 weeks. You should do the test at home and then post it to us for testing. The result will come back in 7 days.
Bowel cancer often has no early warning signs-so even if you feel well do the test.
This screening does not replace any health care you are already getting. If you already see a doctor about any bowel problem you must continue to go to your usual appointments.
Your doctor at medical practice knows that screening is being offered.
If you would like more information or have questions about bowel screening please call us at the helpline on 0800 0121833 (Mon-Fri, 8am-6pm).
Yours sincerely
Dear
You will soon get an invitation to take part in the Scottish Bowel Screening Programme. Screening is offered to everyone aged 50-74.
Bowel cancer is one of the most common cancers, especially for people over 50. It causes 1,600 deaths in Scotland each year.
The good news is there is a simple test that can help find early signs of bowel cancer. The chances of beating bowel cancer are very high when it is found early.
Your testing kit and information leaflets will arrive in the post in about 2 weeks. You should do the test at home and then post it to us for testing. The result will come back in 7 days.
Bowel cancer often has no early warning signs-so even if you feel well do the test.
This screening does not replace any health care you are already getting. If you already see a doctor about any bowel problem you must continue to go to your usual appointments.
Your doctor at medical practice knows that screening is being offered.
If you would like more information or have questions about bowel screening please call us at the helpline on 0800 0121833 (Mon-Fri, 8am-6pm).
Yours sincerely