
Abstract
Objective
To compare the uptake of faecal immunochemical occult blood test (FIT) with guaiac faecal occult blood test (gFOBT) in a screening programme, with specific attention to the demographic and socioeconomic factors that might affect test uptake.
Setting
The Clalit Health Service screening programme, Israel.
Methods
Average-risk individuals aged 50–75 years were randomized into a FIT arm or gFOBT arm using a programme based on the socioeconomic status (SES) of their primary care clinics. G-FOBT was performed with Hemoccult SENSA™ (3 evacuations) and FIT with the OC- MICRO™ (3 evacuations, refrigerating mandated). The GLIMMIX model was used.
Results
There were 5,464 and 10,668 eligible participants in the FIT and gFOBT arms respectively. Compliance in taking the kits was better (but not statistically significantly better) with gFOBT (37.8% vs. 29.3%; odds ratio [OR] 1.43 [95% CI 0.73–2.80]; P = 0.227). Kit return was higher in the FIT arm (65.0% vs. 78.9%; OR 0.45 [95% CI 0.24–0.83], P = 0.021). Overall test uptake was affected by age, gender, being immigrant and SES (determined by whether or not the participant paid national insurance tax, and the SES of the primary care clinic). The overall uptake of gFOBT and FIT was comparable (OR 0.996 [95% CI 0.46–2.17], P = 0.99).
Conclusions
Overall compliance for test uptake was comparable between the two methods despite the more demanding procedure in the FIT arm. Sociodemographic parameters were the major determinants of compliance. An educational programme, with emphasis on the sociodemographic characteristics of the target population, should be instigated.
Introduction
Faecal immunochemical occult blood testing (FIT) has several technological advantages compared with gFOBT: FIT is fully automated, its usage eliminates the need for dietary restrictions, and its sensitivity for CRC detection is almost as high as the sensitivity of colonoscopy. The American College of Gastroenterology (ACG) guidelines for CRC screening specify annual FIT as the preferred cancer detection test. 4 The ACG states that FIT has superior performance characteristics when compared with earlier guaiac-based Hemoccult II cards 4 , but the United States Multi-Society Task Force on CRC maintains that in overall test performances there are no clear patterns of superiority between a high-sensitivity guaiac-based test (Hemoccult SENSA)and FIT. 5
Clalit Health Services, the largest health services provider in Israel, conducts a gFOBT-based CRC screening programme with a current participation rate of about 34.0%. Before considering a change to the CRC screening strategy, we conducted a prospective study comparing gFOBT with FIT. In our recent paper we reported that FIT was feasible and that its usage was associated with an improved performance for the detection of advanced adenomatous polyps (AAP) and CRC. 6
We here compare test uptake in the FIT arm with that in the gFOBT arm, with special emphasis on demographic and socioeconomic factors that might affect compliance.
Methods
The target population and the primary area clinics were clustered according to socioeconomic status (SES). Clinics from each SES were then randomly allocated into either the FIT or gFOBT arm.
The primary outcomes of the study were (i) to compare the ‘kit compliance’ (compliance with taking the kit) in the FIT arm with that in the gFOBT arm; (ii) to compare the compliance for ‘kit return’ (test performed among those who took the kit) in the FIT arm with that in the gFOBT arm; and (iii) to compare the overall compliance for test uptake (test performed among the target population) in the FIT arm with that in the gFOBT arm. The secondary outcome of the study was to assess the effect of the sociodemographic factors on the compliance for test uptake.
Participants and eligibility
Under the Clalit Health Services strategy, every insured citizen is linked to a primary care clinic. Eligible participants were aged 50–74 years and were linked to the nine selected primary care clinics. Patients who had an established CRC or inflammatory bowel disease were excluded. Patients with visible rectal bleeding, hematuria, menstruation or with symptoms related to the gastrointestinal tract were instructed not to perform FOBT.
Randomization (Figure 1)
Flow diagram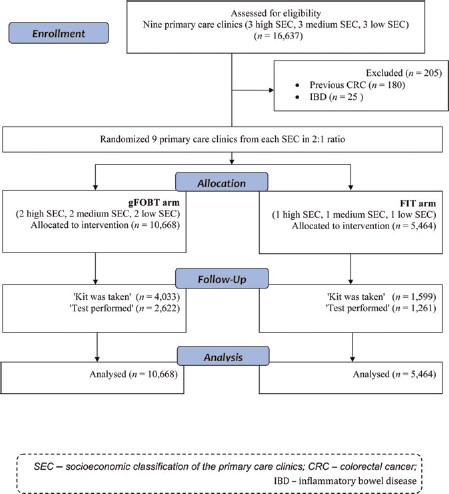
Clalit Health Services primary care clinics are classified into three SES classes (high, medium, low) using software based on postal code and estimated income. Nine medium-sized primary care clinics, including three clinics from each SES class were randomly selected. Because FIT is more expensive and needs more complex strategy (cooling bags and specific transportation), the clinics were randomly allocated into the gFOBT arm or the FIT arm in 2:1 ratio with equal presentation of the SES classification in each arm. Hence, the FIT arm included one clinic from each class and the gFOBT arm included two clinics from each SES class.
Intervention
Participants were instructed to collect FOBT kits from their primary care clinic and to prepare the FOBTs on three separate days (in both arms). They were then asked to bring the kits back to the clinic. Dietary restrictions were required only in the gFOBT arm and cooling measures were required only in the FIT arm (see specific instructions below). Kits were then transported to a central laboratory.
Ascertainment of data
Data on age, gender, remission of national insurance tax, immigration status, and the SES class of the primary care clinic as well as previous diagnosis of CRC or inflammatory bowel disease were retrieved from the Clalit Health Services headquarters database. Immigrants were defined as those who have immigrated to Israel since 1980 (99.9% were from the former USSR).
Specific instructions
OC-MICRO™ (FIT): This FIT has been previously described. 7 Participants in the study received a verbal explanation and written instructions about the test preparations. They received a kit for faecal sampling and were requested to prepare three consecutive daily samples without any limitation of diet or medications. Participants were instructed to keep the samples in their refrigerator and bring the samples back to the clinic using a cooling bag provided with the kits. The samples were refrigerated at 4°C. Within two weeks the samples were analyzed by the OC- MICROTM instrument (Eiken Chemical Co, Tokyo, Japan), the hemoglobin amount was measured and the results were given automatically as ng/mL of buffer. 70 ng/ml threshold was determined as a positive test (the highest of three tubes).
Hemoccult SENSA™ (HOS)
Participants were provided with cards (Hemoccult SENSA™, Beckman Coulter, Fullerton, CA) at the primary care clinic and were requested to follow the manufacturer's instructions on diet and use of medications before and during preparation of the gFOBT. They applied stool on six windows of three cards and brought the cards back to their clinic. The cards were then collected and checked at the central Clalit Health Services Laboratory. The test result was sent to the participant and appeared online in his electronic file. The test was positive if any one of the six HOS windows was positive.
Analysis and statistical methods
Compliance among the 16,360 participants was modeled using SAS 9.2 for Windows GLIMMIX procedure. The appropriate GLIMMIX model for a Binary outcome comprises of a Binary distribution associated with a Logit link function. The GLIMMIX procedure estimates the parameters by applying pseudo-likelihood techniques as in Wolfinger and O'Connell 8 and Breslow and Clayton. 9 Based on these estimates, GLIMMIX also provides odds ratio estimates and 95% confidence intervals (CIs). Tests of hypotheses for the fixed effects are based on Wald-type tests and the estimated variance-covariance matrix. This procedure takes into account the two-level hierarchical structure of the data: participants clustered within clinics. Based on this model the effects of both participant and clinic level predictors on the outcomes were estimated. The clinic level (specific) predictors are: test type (FIT, gFOBT) and SES (high, moderate, low), and the participants’ level predictors are: age (continues or dichotomous above and below 60), gender (F/M), former USSR (Y/N) and remission of national insurance tax (Y/N).
In order to address to the issue of compliance between FIT and gFOBT among different populations according to the SES, we added to the model the interaction between test type and the SES. Compliance is represented in three ways: ‘kit compliance’, ‘test performed’ among all participants, and among participants who just took the kit.
Ethics
The study was authorized by the Rabin Medical Center Institutional Review Board. Individuals were informed and asked whether they wanted to participate in the study, but did not have to sign an informed consent.
Results
Of 16,337 participants, 205 (1.2%) were excluded, 180 had a diagnosis of CRC and 25 had inflammatory bowel disease.
Table 1 presents participants’ characteristics in the 5,464 participants in the FIT group and the 10,668 participants in the gFOBT group. The arms differed in the proportion of M/F, age distribution, percent of immigrants, and percent of participants from primary care clinics classified as low SES.
Characteristics of the included participants
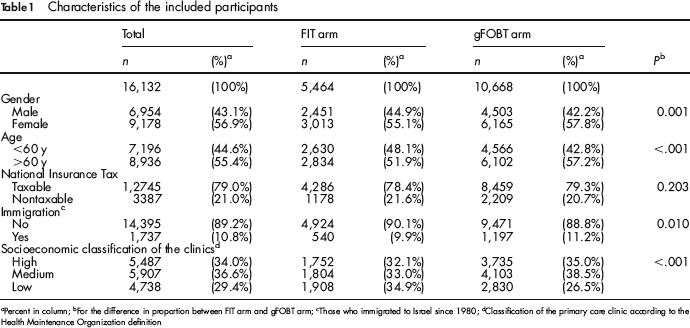
Percent in column;
For the difference in proportion between FIT arm and gFOBT arm;
Those who immigrated to Israel since 1980;
Classification of the primary care clinic according to the Health Maintenance Organization definition
Table 2 shows the univariate and multivariate analysis of the factors affecting compliance in taking the FOBT kits. Independent factors associated with increased compliance were female gender, age ≥60 years, remission of national insurance tax, and immigrants from USSR (since 1980). Compliance favoured non-significantly the gFOBT arm (gFOBT 37.9% vs. FIT 29.3%, P < .001; OR 1.43 [95% CI 0.73–2.80], P = 0.23).
Factors affecting compliance to take FOBT kits
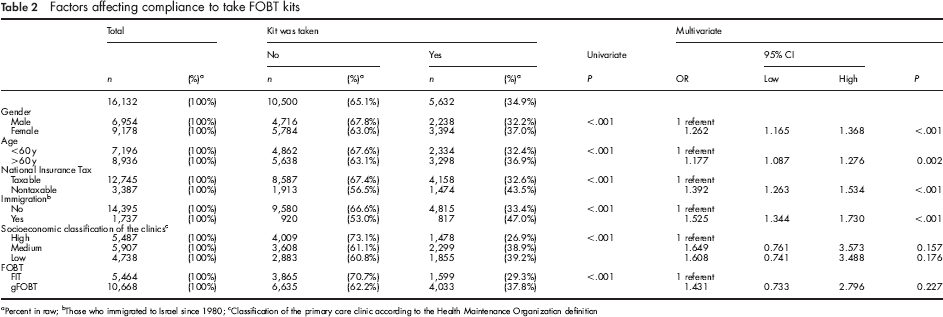
Percent in raw;
Those who immigrated to Israel since 1980;
Classification of the primary care clinic according to the Health Maintenance Organization definition
Table 3 presents, in the same way as Table 2, the factors affecting compliance with kit return. Independent factors associated with increased compliance were female gender, age ≥60 years, immigrants from USSR, classified in the medium SES (as compared with high SES) and test type. Compliance favored the FIT arm (gFOBT 65.0% vs. FIT 78.9%, P < .001; OR 0.45 [95% CI 0.24–0.83], P = 0.021).
Factors affecting compliance with Kit return
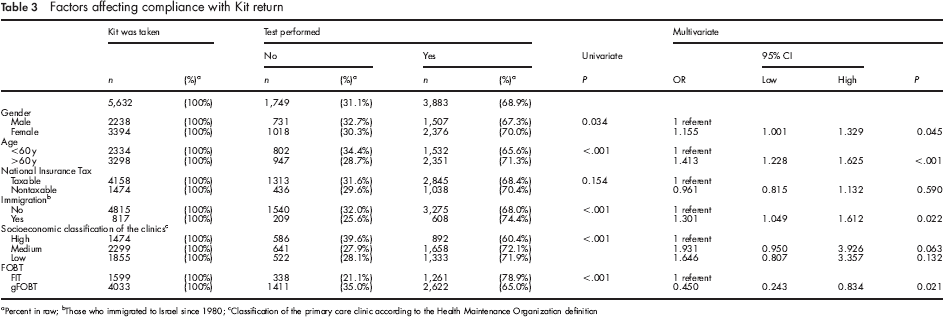
Percent in raw;
Those who immigrated to Israel since 1980;
Classification of the primary care clinic according to the Health Maintenance Organization definition
Table 4 presents the univariate and multivariate analysis of the factors affecting overall test uptake. Independent factors associated with increased compliance were female gender, age ≥ 60 years, remission of national insurance tax and immigrants from USSR. Medium SES (as compared with high SES) showed a trend only (0.096). The overall uptake of gFOBT and FIT was comparable (OR 0.996 [95% CI 0.46–2.17], P = 0.99).
Factors affecting overall compliance in performing FOBT
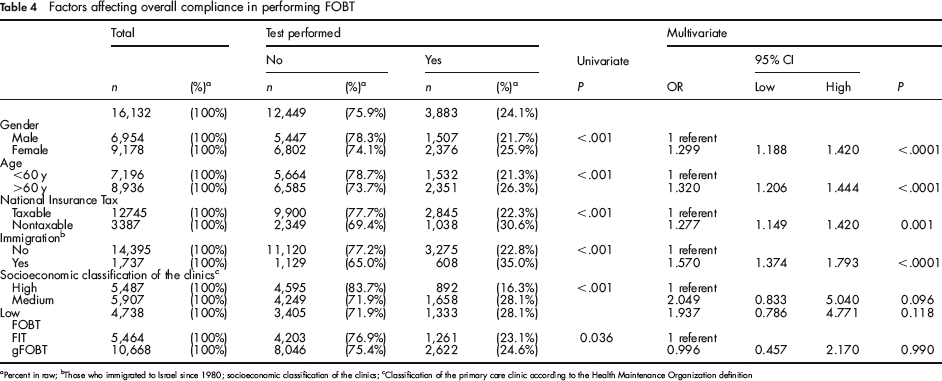
Percent in raw;
Those who immigrated to Israel since 1980; socioeconomic classification of the clinics;
Classification of the primary care clinic according to the Health Maintenance Organization definition
The tests of effect slices for test type x SES sliced by both SES and test type were all non-significant.
Discussion
In this study we aimed to compare the compliance for test uptake in two arms. Dietary restrictions were required only in the gFOBT arm and cooling measures were required only in the FIT arm. Sampling the stool in three different days was required in both arms. Compliance with taking the kits favoured gFOBT and compliance for kit return favoured FIT. The overall compliance for test uptake was comparable between the two methods.
Sociodemographic parameters were the major determinants of compliance. Compliance was greater among the population characterized by low income (remission of national insurance tax), immigrants from USSR and those from primary care clinics classified as medium-low SES. Data on participation rates according to the SES of the primary care clinic in the gFOBT CRC prevention programme in 2009 (Table 5) support the observation that in the Clalit Health Services, which is the provider of about four million citizens, low SES is significantly associated with an increased participation rate. Data from other countries suggest that low SES is usually associated with decreased participation in CRC screening programmes.10,11,12 The impact of SES on cancer screening is complex. Low-SES participants more often reported barriers than their higher-SES counterparts. 13 This may be evident for FIT, representing new technology. Young et al. 14 reported that the SES did not affect participation rate when comparing the old gFOBT with the improved technology-based FOBT (FlexSure, InSure). In our study, immigration from USSR was also associated with increased participation (OR 1.15 [95% CI: 1.04–1.26]).
Participation rate in the gFOBT programme in the Clalit Health Services a according to the SE class of the primary care clinic in 2009
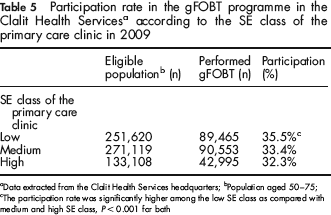
Data extracted from the Clalit Health Services headquarters;
Population aged 50–75;
The participation rate was significantly higher among the low SE class as compared with medium and high SE class, P < 0.001 for both
Gender and age were independent predictors of participation in all screening arms. A low participation rate was especially found among men aged 50–60 years (gFOBT, 22.8%; FIT, 19.2%).
Several studies have compared gFOBT with FIT,14–25 but only a few have compared gFOBT with FIT in different arms.22–26 In their 2010 paper, Hol et al. 25 compared three days of gFOBT without dietary restrictions with one day of FIT (OC-Micro) and flexible sigmoidoscopy (FS) in a Dutch population randomized by age, gender and SES (using postal code). The participation rate was 49.5% for gFOBT, 61.5% for FIT and 32.4% for FS screening. In our results age above 60 years and female gender were independent predictors of increased attendance, however, in the Dutch population, high SES of the participants was associated with increased attendance in all screening arms (gFOBT [OR 1.1 95% CI: 1.0–1.3], FIT [OR 1.3 (1.1–1.5), FS 1.2 (1.0–1.5)]). In another large prospective study, van Rossum et al. 26 compared three days of gFOBT without dietary restriction with one day of FIT (OC-micro), using a randomization programme based on age and gender, but not SES. Again the greater participation was found with FIT (59.6% vs. 46.9%, P < 0.001). Because of the hot climate in Israel, and our previous experience of the degradation of FIT by heat,27,28 participants in the FIT arm were requested to keep the samples in their refrigerator at home and bring the samples back using cooling bags. Our design was, therefore, much more demanding for the FIT arm (three samples, keeping the samples in the refrigerator), although in the gFOBT arm there were dietary restrictions.
In conclusion, we have shown that the overall compliance for test uptake was comparable between the two methods. Sociodemographic parameters are the major determinants of compliance. An educational programme, with emphasis on the sociodemographic characteristics of the target population should be instigated.
Footnotes
Acknowledgements
Eiken Japan provided the OC-MICROTM instrument, reagents and partial financial support for administration.