
Abstract
Objective
Quantitative information on adverse reactions associated with colorectal cancer (CRC) screening tests is useful to estimate the balance between benefit and risk in different strategies.
Setting
Six Italian screening centres.
Methods
Thirty-day active follow-up (interview about side-effects and acceptability of the screening procedure and review of hospital admissions) among average-risk people undergoing flexible sigmoidoscopy (FS), total colonoscopy (TC), fecal immunochemical test (FIT) in a multicentre randomized trial of CRC screening. Multivariable logistic models were used to assess determinants of completion rate and self-reported pain.
Results
The attendance rate following the first invitation and mail reminder was 28.2% (1696/6018) in the FS and 23.0% (1382/6021) in the TC arm. Response rate to the 30-day follow-up questionnaire was 88.6% (1502/1696) among people undergoing FS, and 86.7% (1198/1382) among those undergoing TC. The proportion of people complaining of serious reactions following bowel preparation (odds ratio [OR], 5.17; 95% confidence interval [CI] 3.70–7.24) or reporting severe pain immediately after the exam (OR, 1.86; 95% CI 1.47–2.34) was higher for TC than for FS. The most common post-procedural complaints were abdominal distension and pain. People mentioning pain or bowel distension following preparation were more likely to report severe pain both after FS (OR, 2.13; 95% CI 1.52–2.97) and TC (OR: 2.03; 95% CI 1.41–2.90). The 30-day hospitalization rate was similar after FS, TC and FIT.
Conclusions
Screenees reported higher pain levels after TC than FS. The proportion of people complaining of severe side effects after discharge was similar. Bowel preparation was poorly tolerated by people undergoing TC. Subjects’ reactions to the bowel preparation was predictive of post-procedural discomfort. A commitment of at least 48 hours was required of people undergoing TC, compared with 3–4 for FS.
Introduction
Therefore, additional information is needed to quantify the risk and the severity of adverse effects associated with FS and TC screening. We conducted a 30-day active follow-up of people examined with FS or TC in a screening setting to estimate and compare the burden of adverse effects associated with these two exams. A more accurate estimate of the balance between benefits and risk is important to inform both providers’ and patients’ decisions.
Methods
We conducted a survey among participants in a large population-based randomized trial of different screening strategies for CRC, 9 involving six Italian centres. The study protocol has been described in detail elsewhere. 9 Between November 2002 and January 2004 an average-risk population sample of men and women aged 55–64 was randomized (ratio 1:1:1) within general practitioner (GP) to: 1) biennial immunochemical fecal occult blood test (FIT); 2) ‘once-only’ FS; 3) ‘once-only’ TC. All eligible subjects were mailed a personal invitation letter, signed by the GP, with a pre-fixed appointment for endoscopy. Those who agreed to fix a test date were advised to visit their GP, or the screening centre, to obtain the bowel preparation. A reminder letter was mailed to all non-responders. All enrolled subjects were asked for written consent to the study procedures, which did not entail any cost. The local ethics review committees approved the study.
Bowel preparation
FS preparation was limited to a single enema (133 ml, 22% sodium phosphate) self-administered at home two hours before the test. TC oral preparation with sodium phosphate solution (2 L), starting in the afternoon preceding the scheduled appointment, was adopted in all centres. Limited dietary restrictions (i.e. to reduce consumption of foods with high fibre content and to increase water intake) were recommended for both exams.
Screening procedure
FS and TC were performed by experienced gastroenterologists in hospital endoscopy units, using 140 cm colonoscopes and air insufflation. The aim of the FS examination was advancing the scope beyond the sigmoid-descending colon junction under adequate bowel preparation. No sedation was offered. All polyps <10 mm were removed during FS. Subjects with polyps ≥10 mm, or with ‘high-risk’ polyps <10 mm (>2 adenomas, or villous component >20%, or high-grade dysplasia) were referred for TC.
TC screening examination was conducted as far as could be achieved without producing pain/stress to the patient and it was considered complete when the cecum could be visualized. No standard protocol for sedation was stipulated. However, the option of administering intravenous sedation was always discussed when patients contacted the screening centre and endoscopists routinely explained advantages and drawbacks of a sedated TC.
Data collection
All screenees completed a questionnaire asking about gastrointestinal symptoms during the previous month, family history of CRC, history of previous colorectal endoscopy and use of aspirin or anticoagulants. Endoscopists recorded on a standard form quality of bowel preparation, reach of the scope, characteristics of detected lesions and complications. After completing the exam a research assistant, independent from the endoscopy-staff, administered to all screenees a short itemized questionnaire already used in previous studies10,11 checking pain (four mutually exclusive levels: mild discomfort; I thought it would be worse; I hope it will not be necessary to repeat the test; it was the most severe pain I have ever experienced) and embarrassment (rated as: unacceptable, severe, moderate, mild) experienced during endoscopy. Individuals were advised to contact their GP, or the endoscopy unit, if rectal bleeding or severe abdominal pain had occurred following discharge.
Active follow-up
All subjects examined were called one month after screening by trained interviewers asking for their consent to answer a short questionnaire. They were requested to report adverse reactions associated with preparation and those occurring after the test and to grade their intensity (mild – moderate – severe). The interviewer attempted to contact each subject at least three times over different week days, also outside working hours. We checked hospital admissions occurring within 30 days from the test among attenders in four centres. Due to regional differences in the implementation of the privacy legislation, we were not allowed to link the study database with the hospital discharge records in the other centres. Admissions planned to excise screen-detected lesions were excluded from the analysis. Hospitalizations occurring among people with a negative FIT represented a reference for the admission rate among attenders to a non-invasive test. Comparing hospitalization rates among FS and TC screening attenders with the rates in the general population would lead to biased results, as screening attenders are likely to be healthier.12,13
Statistical analysis
Assuming an attendance of about 25% and 20% in the FS and TC group respectively and the conventional 5% (2-tailed) level of statistical significance, the planned groups size (n = 3000) allows for 80% power to detect 5% absolute differences in the prevalence of side-effects or minor complications associated with the preparation or the test procedure, across intervention groups, given their expected frequency.14,15 As the expected number of severe complications is low (2–3 per 1000 TCs, 1–2 per 10,000 FSs) the study size does not allow to evaluate possible differences across groups.
Chi-square tests were used to test for statistical significance in comparisons of proportions. In the multivariable logistic regression analysis self-reported pain associated with the test was modelled as a function of gender, age at screening, endoscopic findings, use of sedation (for TC), duration of the test, previous experience of endoscopy and trial centre. Separate models were fitted for FS and TC screening. Odds ratios (ORs) and their 95% confidence interval (CI) were used to estimate the associations of interest, both in the univariate and in the multivariable analysis. All statistical tests were two-sided and were considered statistically significant at P < 0.05. The SAS statistical package was used for the analysis.
Results
The attendance rate following the first invitation and mail reminder was 28.2% (1696/6018) in the FS and 23.0% (1382/6021) in the TC arm (OR: 1.24; 95% CI: 1.141.35). The characteristics of subjects screened are reported in Table 1.
Characteristics of the study population
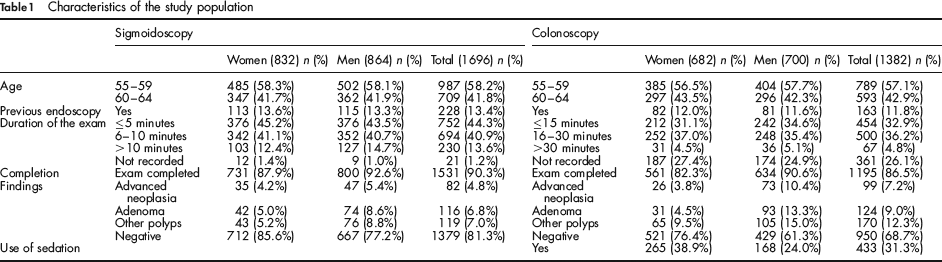
Among people examined with FS, 1659 (97.8%) completed the short itemized questionnaire immediately after the exam and 1502 (88.6%) answered the 30-day follow-up questionnaire (10–0.6% – refusals; 184–10.9% – not traced). The corresponding figures among the 1382 people undergoing TC were 96.7% (n = 1336) and 86.7% (n = 1198; 9–0.6% – refusals; 175–12.7% – not traced).
Bowel preparation.
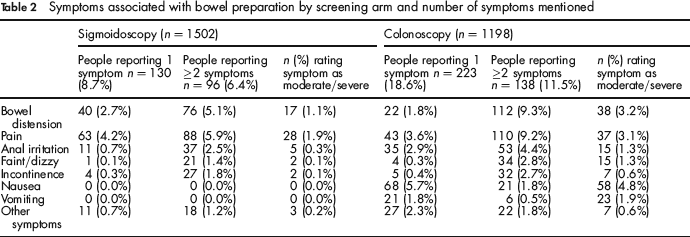
The proportion of people who reported having completed the recommended bowel preparation was 92.4% (1388/1502) among those undergoing FS and 93.8% (1124/1198) among those examined with TC. Overall, some adverse effects associated with the preparation (Table 2) were reported by 15.0% (226/1502) of the interviewees examined with FS and by 30.1% (361/1198) of those examined with TC (OR: 2.44; 95% CI: 2.01–2.95). Also, the proportion of people rating symptoms related to the preparation as moderate or severe was higher (OR: 5.17; 95% CI: 3.70–7.24) with TC (15.1%; n = 181) than with FS (3.8%; n = 57). The most common complaints in both groups (Table 2) were abdominal pain, bowel distension and anal irritation, mentioned by 10.1%, 7.7% and 3.2% of people in the FS group and by 12.8%, 11.1%, and 7.3% of those in the TC group. Bowel distension and pain were associated among those complaining of multiple symptoms in 81.8% (72/96) of the cases in the FS group, and in 67.9% (93/138) of the cases in the TC group.
Symptoms associated with bowel preparation by screening arm and number of symptoms mentioned
Experience of the test.
Screenees were more likely to report severe pain (‘the most severe pain I ever experienced’ or ‘I hope it will not be necessary to repeat the test’) immediately after a TC (16.6%) than after a FS (9.5% – OR: 1.86; 95% CI: 1.47–2.34). People experiencing more than mild embarrassment were 3.8% and 4.0% for FS and TC respectively. This proportion was higher among women (5.4%) than among men (2.4% – OR: 2.34; 95% CI: 1.33–4.15) with FS, while no gender difference was observed with TC. Men were less likely to report severe pain than women both with FS (OR: 0.46; 95% CI: 0.31–0.69) and with TC (OR: 0.46; 95% CI: 0.29–0.72) screening (data not shown), adjusting for screening centre, use of sedation (for TC), completion, exam findings, previous experience of endoscopy and duration of the exam.
One month after screening, 91.7% of people examined with FS and 89.0% of those undergoing TC stated they would recommend a relative or a friend to undergo the same test. Subjects undergoing sedated TC (31% of those examined) were not more likely to recommend the exam (94.3%) compared with those who had no sedation (91.8% – P = 0.112), while those reporting severe pain were less likely to recommend the test compared with those rating the pain mild or lower than expected, both among subjects examined with FS (78.0% versus 95.2%; P < 0.001) and with TC (84.2% versus 94.7%; P < 0.001).
Impact of screening on daily life.
A total of 6.7% of subjects undergoing FS reported having stopped their activity for more than two hours (range 3–24 hours), compared with 15.5% (sedated TC 19.8%; unsedated TC 13.0%) of subjects undergoing TC (OR: 2.55; 95% CI: 1.96–3.32). This trend was similar when considering employed subjects only. Subjects requiring to be escorted for screening were 38.2% in the FS arm and 61.9% (sedated TC 68.4%; unsedated TC: 58.4%) among those examined with TC (OR: 2.99; 95% CI: 2.53–3.53).
Late post-procedural reactions.
Adverse physical reactions following discharge (Table 3) were reported by 521 (34.7%) people examined with FS and by 448 (37.4%) of those examined with TC (P = 0.145).
Symptoms occurring in the days following the screening examination by screening arm and number of symptoms mentioned
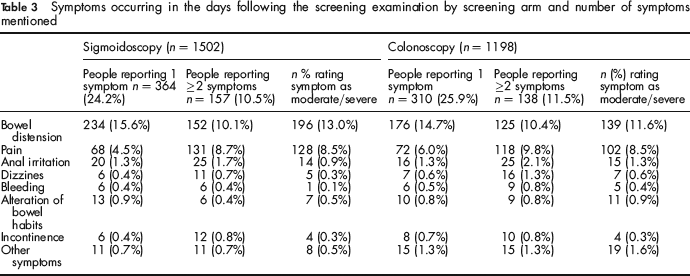
The reported complaints were rated as moderate or severe in 51.2% of the cases (267/521) following FS, and in 49.3% (221/448) following TC (P = 0.551); subjects undergoing TC screening were however more likely (OR: 2.22; 95% CI: 1.04–4.80) to seek medical advice (1.8%–21/1198), as compared with those undergoing FS (0.8%–12/1502).
In about 90% of the cases symptoms arose within two hours from screening and resolved within four hours. Bowel distension and abdominal pain were the most common complaints (Table 3): they were reported as the only symptom by 15.6% and 4.5% of interviewees examined with FS and by 14.7% and 6.0% of those undergoing TC screening, and in association by 8.5% (n = 127) of people examined with FS and by 8.8% (n = 106) of those undergoing TC. In both groups this combination was reported by about 80% of subjects complaining of multiple symptoms (80.9% of those screened with FS and 76.8% of those examined with TC). Bowel distension was rated as moderate or severe by 40.7% and 39.4% of subjects mentioning this single ailment following FS and TC respectively, but this proportion raised to 68.5% and 70.5% among those mentioning multiple side-effects.
Patients who underwent sedated TC were more likely to report feeling dizziness after discharge (3.4% – OR: 4.06; 95% CI: 1.50–11.33) than those having an unsedated exam (0.8%).
Adjusting for screening centre, exam findings, previous experience of endoscopy and duration of the exam (Table 4), people who suffered from abdominal pain and/or distension following bowel preparation were more likely (OR: 2.24; 95% CI: 1.57–3.20) to report post-procedure pain and/or bowel distension following FS, which were instead less frequent among men (OR: 0.62; 95% CI: 0.49–0.79), subjects over 59 (OR: 0.77; 95% CI: 0.60–0.99), and those who had a complete exam (OR: 0.63; 95% CI: 0.43–0.92).
Factors associated with occurrence of bowel distension and/or abdominal pain following discharge (multivariable logistic regression analysis)
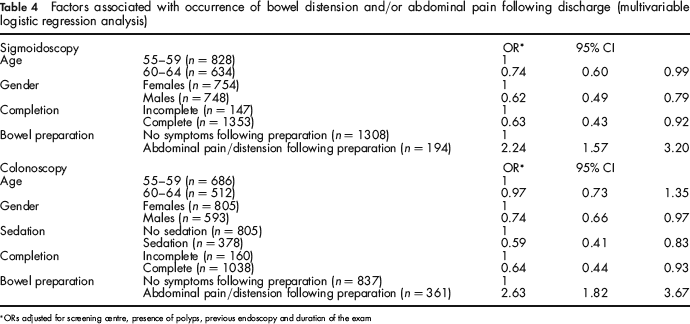
ORs adjusted for screening centre, presence of polyps, previous endoscopy and duration of the exam
A similar trend could be observed in the multivariable analysis among people screened with TC (Table 4): pain and/or bowel distension were less likely among subjects who had a complete (OR: 0.64; 95% CI: 0.44–0.93) or a sedated TC (OR: 0.59; 95% CI: 0.41–0.83), while they occurred more frequently among people reporting abdominal pain and/or distension following bowel preparation (OR: 2.62; 95% CI: 1.62–3.67).
Unplanned hospital admissions within 30 days.
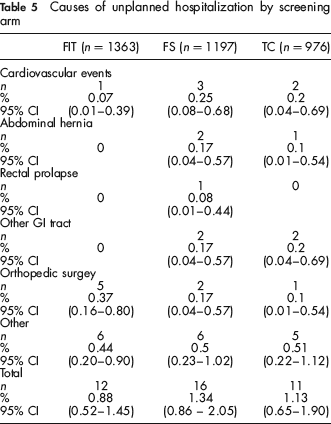
The 30-day admission rate was 1.34% (16/1197), 1.13% (11/976) and 0.88% (12/1363) in the FS, TC and FIT arms respectively (Table 5). In addition, four people (2 in the FS and 2 in the TC arm) reported at the phone interview having been referred to an emergency department following onset of abdominal pain (3 cases) or hypotension: they recovered and were discharged within a few hours.
Causes of unplanned hospitalization by screening arm
Discussion
This is the first large study comparing subjects’ experiences of FS and TC in a screening setting, with a prospective 30-day follow-up after discharge. Also, while most previous reports focused on perforation and bleeding risk,3,16–18 or on complications leading to unplanned hospitalizations,4–6,19 we assessed also the frequency of side-effects, which do not lead to hospitalization but may carry direct and indirect costs for participants and may heavily affect everyday life.
The most striking difference between the two screening methods is related to the burden of bowel preparation, which required longer time and was associated with a nearly five-fold increase in the occurrence of serious disturbances among people undergoing TC, as compared with FS. Contrary to other reports,20,21 screening TC was judged to be more painful than FS, while the proportion of people complaining of any side-effect following discharge, as well as the proportion of those rating these symptoms as severe, was similar for FS as for TC.
Our findings concerning the impact of bowel preparation are consistent with a previous survey showing that three out of four subjects screened with TC rated the preparation as the most difficult part of the procedure. 7 The impact of bowel preparation for TC might be underestimated in our study, as we adopted the two-litre sodium phosphate preparation. This regimen was shown to be better tolerated and equivalent in terms of cleansing efficacy, as compared with the standard four-litre polyethylene-glycol preparation, 22 but recent reports of adverse renal side-effects prompted a warning against its utilization. 23 The adoption of the standard higher liquid doses regimen would likely result in a higher incidence of severe side-effects.
In both groups subjects complaining of symptoms associated with preparation were also more likely to complain of pain and/or bowel distension following discharge. Collecting information about reaction to the preparation might therefore orient the adoption of specific examination procedures (sedated TC, insufflation with carbon dioxide [CO2]) or instruments (i.e. pediatric 24 or variable stiffness scopes 25 ) which might reduce the likelihood of side-effects after the exam.
Abdominal distension and pain, lasting a few hours after discharge, represent an important cause of distress, reported by about 40% of the screenees, who rated them as moderate or severe in nearly half of the cases. These proportions are even higher than previously reported (range 5–30%) in settings where air insufflation was used.7,8 Gas insufflation is mandatory to ensure good visualization, but the air, now commonly used for this purpose, may be retained in the bowel, 26 causing pain and discomfort.27–30 Our data would support therefore the adoption of CO2 insufflation, which is associated with a significant reduction of abdominal pain and discomfort following endoscopy,28–31 as it might abate the most important component of self-reported post-procedural distress This policy might also influence acceptability of endoscopic screening, as pain associated with these procedures has been identified as a major barrier to participation.32,33 Warm water infusion as an adjunct to air insufflation might also be associated with an attenuated abdominal discomfort and a reduced use of sedation. 34 This approach may represent an option to improve patients’ experience with endoscopic screening, if its effectiveness will be confirmed by randomized trials.
The proportion of people rating the pain associated with the exam as severe was not reduced following sedated TC, and the proportion of screenees who would recommend the test to relatives or friends was similar among those undergoing sedated as among those having unsedated TC. Sedation was instead associated with a lower likelihood of experiencing bowel distension and/or pain after discharge, even if time to recovery to normal life was longer and post-discharge symptoms not related to insufflation were more frequent. The lack of impact of sedation on the reported level of pain associated with the exam might be explained by the adoption of a selective sedation policy: sedated exams were performed in about 30% of the cases and apparently tended to be offered more often to patients who were more likely to report a painful experience in the exam (i.e. women). However, the observed trends were maintained when restricting the analysis to the two centres offering sedation routinely. Although our study was not designed to assess the role of sedation, these findings would thus suggest that, in a screening setting, the benefits ensured by routine use of sedation should be carefully balanced against the expected decrease of the complications rate,14,35,36 the cost reduction, resulting from the decreased need of cardiopulmonary monitoring, and the lower impact on the patient's life of unsedated TC.
The study size does not allow for detecting small differences in the incidence of major complications across screening strategies. However, comparing the rates of unplanned hospitalizations among people undergoing FS or TC with those of subjects with a negative FIT, we did not find any indication of a substantial increase in risk. We could check for 30-day hospital admissions after discharge in four centres only, but we found only one unplanned admission among non-responders to the phone questionnaire. The finding at the follow-up interview of four cases of unplanned referrals to an emergency department confirms that the endoscopy complication rate may be underestimated, if an active follow-up of patients after discharge is not implemented.8,14
Given the relatively low participation, attenders might represent a self-selected group of highly motivated, health-oriented people, who might be more prone to tolerate minor side-effects of screening and therefore to under-report screening-related adverse reactions. However, given the randomized design, the estimates of the relative differences between FS and TC screening should not be affected by the possible underestimation of the absolute frequency of side-effects.
In conclusion, although the reported level of pain associated with the test was significantly lower for FS than for TC, the proportion of people complaining of side-effects following discharge, as well as the proportion of those rating these symptoms as severe, was similar. TC has a much higher impact on everyday life: about 15% of the screenees experienced severe symptoms when assuming the preparation, about 20% could not go back immediately to their life activities and about 60% needed an escort to go back home, these proportions being higher among people undergoing sedated TC. Therefore, consistent with previous reports,37,38 when taking into account the time devoted to the bowel preparation, and the time needed to return to normal activities after discharge, a commitment of at least 48 hours is required for screening TC, while the corresponding time for FS is about 3–4 hours.
Our data support the adoption of CO2 insufflation, as post-discharge pain and bowel distension, likely associated with air insufflation, represent the major components of post-test distress. Finally, as subjects’ reactions to the bowel preparation was predictive of post-procedural discomfort, collecting information about side-effects of the preparation might be useful to plan the performance of the examination.