
Abstract
Setting
The NHS breast screening programme (NHSBSP) in England currently invites women aged 50-70 every three years. Whilst screening is acknowledged as efficacious for women aged 50-69, several countries routinely invite women up to the age of 74. The NHSBSP in England is beginning to invite women up to the age of 73. Although the incidence of breast cancer increases with age, the possible benefits of screening older women must be balanced against shorter life expectancies and possible overdiagnosis. In England women can self-refer after reaching the invitation upper age limit.
Objective
We examined the extent to which older women in England self-referred over a three-year period and studied the screening outcomes in these women.
Methods
Routinely collected data from screening units in England were used to calculate screening performance measures for women who self-referred between 1 April 2005 and 31 March 2008. The tumour characteristics of all screen-detected cancers were examined by previous screening history and age group (71-74 and ≥75 years).
Results
During the three-year period 139,910 women aged over 70 self-referred; equivalent to 4% of the female population aged over 70 having been screened. The majority of women who self-referred had been screened within the previous five years (76% of those aged 71-74 and 65% of those aged 75 or over). Approximately 4% of these women were recalled for assessment and cancer detection rates were similar in both age groups.
Conclusion
Only a small proportion of all women aged over 70 utilize the self-referral policy of the NHSBSP, and most such women are aged below 80.
Introduction
Screening is acknowledged as efficacious for women aged 50-69, but evidence from randomized controlled trials for screening in older women is minimal due to the limited number of trial participants over age 70 years. Data from the Swedish Two-County Study showed a statistically significant decrease in mortality associated with screening the 65-74 age group. 2 Several countries with organized screening programmes routinely invite women up to the age of 74. Screening in the United States is opportunistic and is recommended for women up to age 75 but in practice there is no upper age limit. In England the NHS Cancer Reform Strategy announced the increase of the upper age limit to 73 by 2012 3 , and a pilot randomized study of this increase in invitation age has recently been completed. 4
In addition to the lack of evidence regarding the benefits of screening older women, reasons often cited for not routinely inviting older women include: lower uptake, co-morbidities, less aggressive tumours and shorter life expectancies. However, the incidence of breast cancer increases with age. Whilst incidence rates in the 65-69 and 70-74 age groups reflect routine screening in women aged 70 and under (4.0 and 3.1 per 1000 women respectively); incidence rates in the 75-79, 80-84 and ≥85 age groups in England in 2007 were 3.7, 3.8 and 4.1 per 1000 women respectively.
In England, women in the target age group are automatically sent an invitation to screening every three years. Women can continue to be screened every three years after reaching the upper age limit by requesting an invitation to screening (self-referring). Women are informed of this in their letter following a screening episode which ends in a ‘normal’ result (the episode can include assessment where mammographic interpretation was abnormal). In this study we have looked at the number of women aged over 70 who self-referred, and the screening outcomes of these women over a three-year period in England.
Methods
We analysed data for all women in England over the age of 70 who self-referred in the three-year period: 1 April 2005-31 March 2008. We used mid-2007 population figures from the Office for National Statistics to estimate the number of women who self-referred as a proportion of the total population.
Aggregated screening activity and outcome data are collected annually from individual screening units. These routine data categorize women both by their previous screening history (never screened, screened by the NHSBSP within the last five years and screened more than five years previously) and by age (71-74 years and aged 75 or over). We calculated screening performance outcomes (recall to assessment, cancer detection, positive predictive value of recall to assessment [PPV], benign biopsy and non-operative diagnosis of cancer) by both age group and previous screening history. Anonymized individual-based pathology data for each screen-detected cancer collected annually from screening units were used to study the tumour characteristics of screen-detected cancers following self-referral in women aged over 70 years. We compared the results in women who had self-referred with those from the oldest age group routinely invited and screened by the NHSBSP (65-70 years).
Results
During the three-year period of the study 139,910 women aged 71 or over requested an invitation to screening: equivalent to 4.3% of women aged over 70 having been screened during the three year period (10.6% aged 71-74 and 2.2% aged 75 or over). During the same period, 4,617,493 women aged 50-70 accepted an invitation to screening, and uptake in the 65-70 age group was 71.9%. Of the older women self-referring, 62% were aged between 71 and 74 and 72% of self-referring women had been screened within the past five years; 47% of women aged 71-74 and 25% aged 75 or over.
Rates of recall for assessment and cancer detection by previous screening history and age group
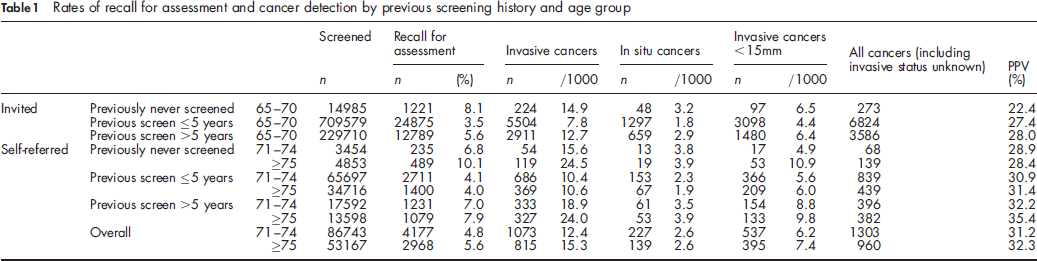
Invasive cancer detection rates in women screened less than five years previously were 10.4 and 10.6 per 1000 women in the 71-74 and ≥ 75 age groups respectively. The rates of invasive and non-invasive cancer detection followed similar patterns to overall rates of cancer detection and the proportion of cancers that were non-invasive was similar in both age groups and by previous screening history. The proportion of cancers measuring less than 15 mm was similar in self-referring women who had been screened within the last five years compared with the invited age group and was lower in those women who had not previously been screened or those who had been screened more than five years previously. The PPV was higher overall in women who self-referred (31.7%) compared with invited women aged 65-70 (27.5%) (χ 2 = 52.7, P < 0.001). The rate of benign biopsy was similar in women screened within the last five years compared with invited women aged 65-70 (0.7 and 0.6 per 1000 women screened, χ 2 = 2.95, P = 0.09) whilst rates in women not previously screened or screened more than five years previously (1.6 and 1.2 per 1000 women screened were both significantly higher, χ 2 = 6.82, P < 0.01).
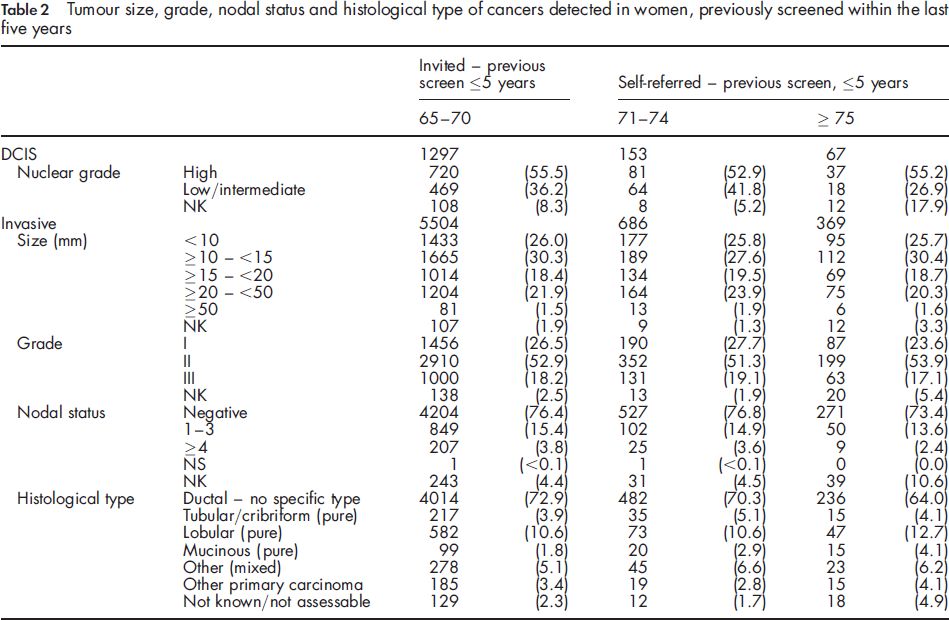
Tumour size, grade, nodal status and histological type of cancers detected in women, previously screened within the last five years
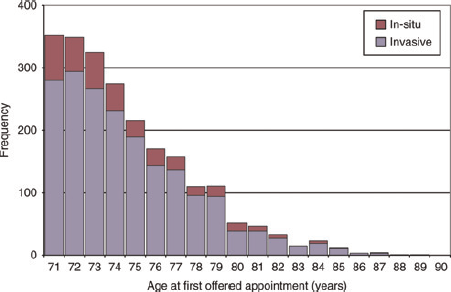
Histogram of screen-detected cancers in women aged over 70 who self-referred by age at first offered appointment and invasive status
Discussion
The results of this study have shown that the self-referral policy of the NHSBSP was only utilized by a small proportion of women aged over 70. During the study period routine invitation to screening ceased at age 70, and only 4% of women aged over 70 self-referred whilst 72% of women aged 65-70 were screened following routine invitation. The majority of women who self-referred were aged between 71 and 74 and most of these had been screened within the last five years; the youngest of these women will have been screened following routine invitation within the previous three years. Most women aged 75 or over had also been screened within the last five years and these will have routinely requested screening after they reached 70 years. These results suggest that only a small cohort of women repeatedly self-refer after age 70. Less than one third of self-referrals were in women who were recorded as having not previously been screened or who had been screened more than five years previously. A higher proportion of these women were recalled for assessment and detected with cancer compared with those screened within the previous five years. Some of these women may have requested screening because they had breast symptoms, and the proportion of benign biopsies was significantly higher in these women compared with those screened within the last five years. In this study we were unable to look in detail at self-referrals in women aged 75 or over as routinely-collected screening outcome data were grouped together for these women. However more than half of the cancers in women aged 75 or over occurred in the 75-79 age group: this suggests that only a small proportion of women aged 80 or over self-referred, as cancer detection rates would be expected to be highest in the oldest age group however 8% of cancers were found in women aged 80 or over.
The increase in the upper age limit from 64 to 70 resulted in more women aged 65-70 being screened than had previously self-referred and uptake was comparable with that in younger women. 5 Women in this study aged 71-74 who had been screened within the previous five years had a higher rate of recall to assessment than invited women aged 65-70. The cancer detection rate was higher in the age group that had self-referred, although the tumour characteristics were similar in both groups. The PPV was greater in women aged over 70 compared with the 65-70 age group; an increase in PPV with age was observed previously in the 65-70 age group compared with the 60-64 age group when the upper age limit of invitation was increased to age 70. 5 A higher PPV of recall in the invited 70-74 age group has also been reported in the Netherlands, and uptake in this age group was 79.1% in 2007. 6
Many older women present with late stage disease. 7 Further follow-up of a recent awareness study will determine if earlier presentation occurs as a result of educating older women about both their risk of breast cancer and breast changes that may be indicative of cancer. 8 Despite the incidence of breast cancer increasing with age some women assume their risk is reduced because they are not invited to screening and these women support either greater promotion of the NHSBSP self-referral policy or the removal of the upper age limit of invitation. 9 However women in this survey were not likely to be representative of all women over age 70 as 43% of women were under age 75, and only 28% of women were aged 80 or over. Whilst the self-referral policy of the NHSBSP currently allows women to be screened beyond age 70, our results showed that most self-referrals are in women under age 75 as most women self-refer within three years of their last invitation. However when the upper age limit of invitation is increased to 73 years most self-referrals will be in women aged over 75. A reduction in breast cancer mortality from screening has been shown only from the invitation of women up to age 75 although Boer suggested that screening is likely to benefit healthy older women. 10 In this study we showed that tumour characteristics were similar in the 71-74 age group compared with the 65-70 age group but there was a greater proportion of cancers in women aged 75 or over that had unknown histological information compared with younger women. This may reflect the fact that co-morbidities increase with age and that these women do not have surgery as result of co-morbidities. However, the All Breast Cancer Report showed that older women with screen-detected cancers were more likely to have surgery than those diagnosed symptomatically. 11 The authors concluded that surgery is possibly more appropriate for screened rather than unscreened older women because they are healthier. However, women who self-refer are likely to be more breast aware and not delay presentation even in the absence of screening. 12 Furthermore, screening has a propensity to identify slow-growing invasive tumours and also to detect a proportion of non-invasive cancers, both of which may not have presented clinically during a woman's lifetime. The proportion of such cancers is likely to be greater in older women compared with younger women because of increasing sojourn time 13 and shorter life expectancies. A modelling study has estimated that inviting the 71-73 age group to screening will prevent around one breast cancer death per 1000 women screened, though at a cost of greater overdiagnosis than at younger ages. 14
In conclusion we showed that the rate of self-referral in women aged over 70 was low. Women were most likely to self-refer within three years of their last routine screen, and when the upper age limit is increased to 73, we would therefore expect a higher proportion of women aged 74 or over to be screened and an increase in the absolute numbers of cancers detected compared with a similar age group in the present study. These self-referrals should be carefully monitored as most will be in the age group for whom there is no evidence that screening is effective, and these women will have shorter life expectancies and are likely to have more co-morbidities than those women who self-referred in the present study.