
Abstract
Objective
To examine rates and factors associated with adherence to annual repeat lung cancer screening in two cohorts.
Participants and methods
The self-pay cohort (n = 2083) was individuals aged 40 years and older with no prior cancer and a smoking history. Participants had to obtain a prescription from their doctor for the low dose, computerized tomography scan (CT), and were responsible for payment of $300 as these CT scans are not typically covered by insurance. The no-pay cohort (n = 1304) was individuals aged 60 and older with a smoking history, and no prior cancer. The initial and one year repeat CT were provided free of charge. Rates of adherence for each cohort were analyzed by demographic variables, smoking history, family history of lung cancer, smoking status (former/current), perceived risk and worry of getting lung cancer and baseline screening CT.
Results
Adherence to annual follow-up was lower for the self-pay than for the no-pay cohort (62% vs. 88%). Both the self-pay and no-pay cohorts had higher adherence rates among Caucasians and those who had a college degree. A greater perceived risk of getting lung cancer increased adherence among the self-pay cohort. Non-calcified nodules found on baseline CT increased the adherence for the self-pay cohort, but decreased the adherence for the no-pay cohort.
Conclusions
These findings should be used in developing educational materials and targeted retention strategies to increase adherence with repeat lung cancer screening.
Introduction
Participant adherence with screening recommendations, follow-up and treatment will all influence study findings. High rates of follow-up adherence are essential to ensure the quality of the findings obtained from randomized controlled screening trials (RCT). 4 Conversely, low rates of adherence can introduce bias that may threaten the overall interpretability of study findings. As screening RCTs are analyzed according to randomization irrespective of adherence (intent to treat), lack of adherence in either group will result in underestimation of the screening effect (positive or negative). 4
To date, lung cancer screening studies examining chest X-ray have found wide variation in repeat screening non-adherence with rates ranging from 10–45%.5,6 Within the Prostate, Lung, Colorectal and Ovarian (PLCO) screening trial, 14% of screening enrollees were non-adherent to one or more annual, repeat chest X-ray screenings. 7 Among individuals with a false-positive screening result, non-adherence was 17.2% compared with 10.3% among those with negative screening results. Montes and colleagues found that 45% of smokers did not return for annual repeat CT. 8
In the current study, we examined the return rate for annual repeat screening in two large lung cancer screening programme cohorts, those who were required to pay for their screening CT (self-pay) and those who did not (no-pay). In addition, we analyzed potential participant characteristics associated with adherence so as to target health education interventions to insure adequate follow-up among those at highest risk for non-adherence.
Methods
Weill Cornell Medical College (WCMC) developed a lung cancer screening programme, the Early Lung Cancer Action Program (ELCAP), for individuals at risk for lung cancer. The first screening cohort, called the ‘self-pay’ cohort, included 2083 individuals who enrolled in an unfunded study between 1999 and 2003. Individuals were 40 years of age or older with a smoking history of at least one pack-year, no prior cancer and no CT in the prior three years. Participants were required to obtain a prescription from their physician for the baseline and annual repeat CT. The cost of the initial CT was not covered by insurance and all participants were responsible for payments of $300 for their baseline and annual repeat CT scan. Participants with a finding on their baseline CT were able to apply their medical coverage towards the cost of subsequent CT tests, including the annual repeat CT. The study was approved by the Institutional Review Board (IRB#0296–212B).
The second cohort, called the ‘no-pay’ cohort, included 1304 individuals enrolled in a funded study also conducted at WCMC between 2001 and 2002. Enrollment was restricted to individuals at least 60 years of age, with a smoking history of at least 10 pack-years, no prior cancer (other than non-melanotic skin cancer) and no CT in the prior three years. The baseline CT screening and the first annual repeat CT test were provided at no cost. Similar to the ‘self-pay’ cohort, participants with a finding on their baseline CT could apply their medical coverage towards the cost of subsequent follow-up CT tests. The study was approved by the Institutional Review Board (IRB#0296–212A).
All other aspects of the screening protocol (written informed consent, baseline interview, definition of a positive initial CT result, the CT result notification procedures, and recommendations for further diagnostic work-up) were identical. CT results were sent to each participant and their referring physician. See the I-ELCAP protocol 9 for further details regarding the screening procedures. The web-based ELCAP Management System tracks baseline data, outcomes and adherence to the screening programme. With the exception of those found to have lung cancer at the baseline CT scan, all participants in both cohorts were recommended to return for an annual repeat CT scan.
Consistent with the standardized screening programme protocol, 9 there were multiple efforts made to schedule the annual repeat appointment. Sixty days prior to the annual follow-up date, the research staff began calling the self-pay and the no-pay cohorts to schedule their repeat CT scans. The self-pay cohort was reminded about the out-of-pocket cost ($300) and that a prescription from their physician was required. If a participant was not reached, a voice message instructing him/her to schedule an appointment was left. If need be, additional phone calls were made followed by personalized letters that were also sent to the patient's physician. If the participant did not respond after three calls and three letters, a final fourth letter was sent by certified mail stating that this was the final scheduling attempt. All scheduling phone calls and mailings were documented in the database. Participants that were reached but refused to schedule a follow-up CT scan were asked to provide a reason. If the participant was being followed elsewhere, external reports were requested and entered into the database. Both the self-pay and no-pay cohorts received a reminder call one day prior to their appointment.
The primary outcome was whether or not participants returned for the first annual repeat CT with adherence defined as evidence of repeat CT scan within 18 months following the initial baseline CT scan. For these analyses, we excluded participants with lung cancer diagnosed within 18 months from the baseline CT as well as those who died before their first annual repeat scan (n = 95). Factors examined as predictors of follow-up adherence were: age, gender, total pack-years of cigarette smoking, smoking status (former vs. current smoker), race, family history of lung cancer, perceived risk of lung cancer, education, and findings on initial baseline CT scan. Perceived risk of lung cancer was assessed using a single five-point Likert scale item.10,11 Participants were asked: ‘Compared to other people who are the same age and sex, is your risk of getting lung cancer much less than, slightly less than, about the same as, slightly more than, or much more than the risk that these people face?’ Responses were dichotomized as less likely/about the same or more likely. Education was coded as having at least a college degree or having less than a college degree. Baseline CT finding was coded as negative (no non-calcified nodules), semi-positive (solid and part-solid non-calcified nodules all < 5 mm in diameter, or non-solid non-calcified nodules < 8 mm in diameter), or positive (1 or more solid non-calcified nodules ≥ 5 mm in diameter, or 1 or more non-solid non-calcified nodules ≥ 8 mm).
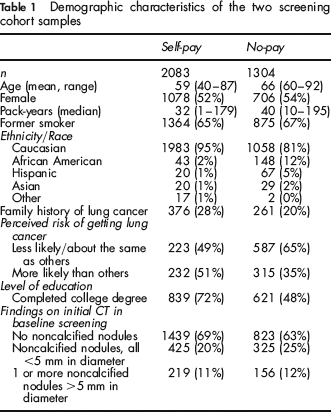
All statistical analyses were performed using the Statistical Analysis System, SAS Institute, Version 8.2. Univariate analyses and frequencies were generated to provide a descriptive summary of demographic variables and other sample characteristics. Table 1 shows the characteristics of the two screening cohorts. Participants in the self-pay cohort were younger, had higher level of education, reported greater perceived lung cancer risk and had a lower minority enrollment than the no-pay cohort. Point estimates were examined separately for each cohort. Chi-square and Wilcoxon's test statistics were used to examine follow-up screening adherence and each of the possible predictors. Odds ratios and 95% confidence intervals were calculated to examine the strength of the associations. Logistic regression analysis examined independent predictors of adherence within each screening cohort.
Demographic characteristics of the two screening cohort samples
Results
Rates of adherence to follow-up screening. Participants in the self-pay cohort had lower return rates than the no-pay cohort. Of the 2083 study participants in the self-pay cohort who were recommended for annual repeat screening, 1296 (61.5%) returned. Of the 787 (38.5%) that did not return for repeat CT, 357 (61%) did not respond to our extensive scheduling efforts (i.e. three letters and three phone calls) and 206 refused but did not specify a reason for non-adherence. Of the remaining 224 non-returning participants, the following reasons were provided: 58 (26%) noted a cost burden, five (2%) had a medical condition other than lung cancer, 14 (6%) reported that their physician advised against continued screening, two (1%) expressed concern about radiation exposure and 145 (65%) did not return due to other personal reasons.
Of the 1304 study participants in the no-pay cohort, 1146 (88%) returned for annual repeat screening. Of the 158 (12%) that did not return, 78 did not respond to three letters and three phone calls and 11 refused follow-up but did not specify their reason. The remaining 69 participants reported the following reasons for non-adherence: 14 (20%) had a medical condition other than lung cancer, five (7%) reported that their physician advised against screening, eight (12%) expressed concern about radiation exposure and 42 (61%) due to other personal reasons.
Factors associated with annual repeat screening adherence. Repeat adherence in the ‘self-pay’ cohort was positively associated with a higher perceived cancer risk (OR = 1.61, 95% CI = 1.11–2.33), being Caucasian (OR = 2.71, 95% CI = 1.79–4.09), having a college education (OR = 1.32, 95% CI = 1.03–1.71), being a former smoker (OR = 1.38, 95% CI = 1.15–1.67) and having a semi-positive or positive finding on baseline CT (OR = 2.47, 95% CI = 2.01–3.04). In the ‘no-pay’ cohort, repeat adherence was positively associated with being Caucasian (OR = 1.55, 95% CI = 1.05–2.28), having a college education (OR = 1.83, 95% CI = 1.29–2.59) and negatively associated with older age (OR = 0.67, 95% CI = 0.47–0.95) and having a semi-positive or positive finding on baseline CT (OR = 0.66, 95% CI = 0.47–0.93). A greater perceived lung cancer risk significantly increased adherence among the ‘self-pay’ cohort, whereas among those in the ‘no-pay’ cohort who reported higher baseline levels of perceived lung cancer risk, there was a non-statistically significant trend towards decreased adherence to repeat screening. In other words, positive findings on baseline CT significantly increased repeat adherence for the ‘self-pay’ cohort but the reverse was true in the ‘no-pay’ cohort (Table 2).
Adherence for annual repeat scan by screening cohort
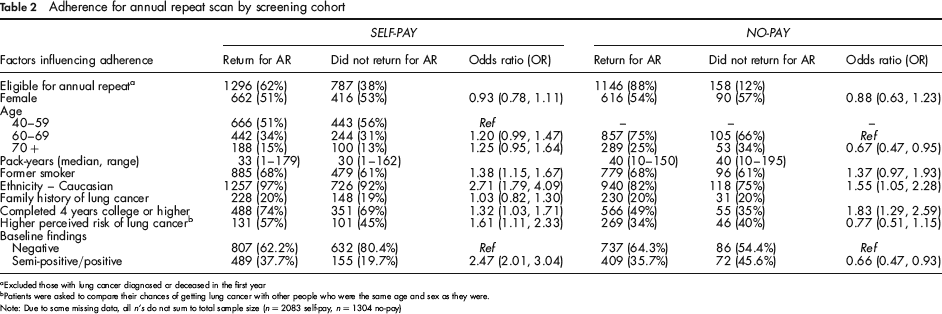
Excluded those with lung cancer diagnosed or deceased in the first year
Patients were asked to compare their chances of getting lung cancer with other people who were the same age and sex as they were.
Note: Due to some missing data, all n's do not sum to total sample size (n = 2083 self-pay, n = 1304 no-pay)
Multivariate logistic regression analysis revealed that annual repeat adherence was significantly associated with race (P < 0.0001), being a former smoker (P = 0.0003), positive findings on baseline CT (P < 0.0001), smoking pack-years (P = 0.005) and education (P = 0.001) in the self-pay cohort. For the no-pay cohort, education (P = 0.0008) and negative findings on baseline scan (P = 0.02) were significant predictors of repeat adherence.
Discussion
We examined adherence for annual repeat CT within two large cohorts of lung cancer screening programme enrollees. The return rate for annual repeat screening was lower for the self-pay cohort than the no-pay cohort (62% vs. 88%, respectively). Overall, Caucasian and college-educated participants were more likely to be adherent. The effect of the baseline screening finding differed by screening cohort with the self-pay cohort more likely to return if they had some abnormality on their baseline scan whereas the no-pay cohort was less likely to return for repeat scanning if they had a baseline abnormality detected. In the self-pay cohort only, participants who were former smokers and reported greater perceived risk of lung cancer were more likely to be adherent to repeat screening.
The higher rate of adherence in the no-pay cohort suggests that removing financial barriers by offering free screenings or health insurance coverage may facilitate follow-up adherence to a lung cancer screening programme. Similar findings have been observed for repeat mammography screening when financial barriers have been eliminated (e.g. coverage or offering free vouchers).12,13 Prior repeat mammography studies have also found that Caucasians and those who have completed a college education are more likely to be adherent to follow-up screening.14–17 As has been noted in breast and cervical cancer screening studies, 18 current smokers are less likely to be adherent to a wide range of cancer prevention and early detection guidelines. 19 Consistent with findings reported by Montes and colleagues, 9 former smokers have taken steps to reduce their cancer risk through smoking cessation and may in fact be more concerned and less ambivalent about adhering to repeat screenings. Further behavioural research is needed to better understand the underlying health beliefs and motivation associated with decision-making about adherence to repeat screening. 20 Current smokers enrolling in lung cancer screening programmes, particularly self-pay, should be targeted for educational efforts to identify and address barriers to repeat lung cancer screening adherence.
We found lower adherence rates among older participants in the no-pay cohort. Prior studies examining the effect of age on adherence to other cancer screening modalities have demonstrated mixed results. One study showed higher adherence among older participants 14 whereas other studies have found higher rates of repeat mammography among younger women.15,16,21 Unlike prior findings in the breast screening literature, we did not find family history of lung cancer to be an important factor associated with repeat scanning adherence.14,16 Perhaps this discrepant observation reflects keen awareness of family history as a risk factor for breast as opposed to lung cancer where smoking history is widely recognized as the predominant risk factor.
Consistent with work demonstrating the role of cognitive processes on cancer screening decisions, 20 adherence to repeat lung screening was associated with self-pay participants who reported greater perceived risk of getting lung cancer. The self-pay cohort, who can be considered to be early adopters of low dose CT scan for early detection of lung cancer, reported greater concern about their likelihood of developing lung cancer and hence appear more motivated to be adherent to recommendations for repeat annual screening. However, among the no-pay cohort, there was a non-significant trend of greater non-adherence to repeat screening among those with higher baseline levels of perceived risk. This finding warrants further investigation into the role of cognitive and affective (e.g. anxiety and cancer worry) determinants of repeat lung cancer screening. In addition, future studies wanting to better understand the role of cognitive processes associated with decisions to seek lung cancer screening should consider use of a more comprehensive tool for the measurement of lung cancer risk perceptions. 22
The observed effect of baseline CT finding on repeat adherence was complex. Finding a nodule on the baseline CT increased repeat adherence for the self-pay whereas it lowered adherence for the no-pay cohort. Interestingly, participants in the PLCO trial, also a no-pay cohort, showed the same pattern in that repeat adherence was poorer among those who had a prior positive result that turned out not to be lung cancer. 17 PLCO investigators hypothesized that receiving normal results provided positive reinforcement (reassurance) to continue with the screening trial whereas receiving abnormal findings required a further diagnostic work-up associated with medical billing charges and at least transient cancer-related anxiety prior to ruling out lung cancer. 17 In our no-pay cohort, participants were indeed billed for any follow-up diagnostic testing. Several no-pay participants felt that the screening programme should have covered the costs for any subsequent diagnostic workup, even though they had been informed at enrollment that any diagnostic work-up for a baseline abnormality would be billed according to standard medical billing practices. Medical costs and anxiety generated by a positive baseline finding may lead some screening participants to adopt a negative attitude towards returning for repeat screening in order to avoid the potential for threatening information. Future studies should examine the expectations and intentions of no-pay screening participants.
In contrast, we found that those in the self-pay cohort were more likely to return for annual repeat screening if an abnormality (nodule) was found on the baseline CT scan. We do not know whether their follow-up adherence was higher because of the increased cancer worry associated with confirmation of lung cancer risk or the likely approval of health insurance to cover the annual repeat CT. The adherence rate was highest for the self-pay cohort when there was a positive baseline result and high perceived cancer risk. These findings are consistent with a recent meta-analysis examining the effect of false-positive mammogram results on repeat breast cancer screening, in that US women who received false-positive results on screening mammography were more likely to return for routine screening than those who received normal results. 23 Given the sensitivity of CT scans future research is needed to understand whether individuals who receive positive results from a baseline screening are dissuaded from returning for routine testing or whether the scare’ of possible lung cancer encourages future screening behaviour. Similarly, when the baseline scan detects coronary artery and/or pulmonary disease, care should be taken to advise appropriate clinical management.
Prior repeat screening studies have demonstrated the utility of reminder calls and letters. In several prior mammography studies, physician recommendation was cited as critical cue for maintaining adherence to breast cancer screening.24,25 In the absence of sufficient public health data to recommend screening for lung cancer, participants may have lacked one of the essential cues (i.e. physician advice) associated with maintenance of other screening behaviours. If there were established screening guidelines for lung cancer of which both the participants and physicians were aware, then the return rate would likely improve.
Our findings underscore the need to increase awareness and understanding about the importance of adhering to follow-up protocols for screening trial participants and their referring physicians. Providing rationale for the importance of returning for repeat annual CT scans should be emphasized during the informed consent procedure and reinforced at the conclusion of the baseline screening appointment. This discussion should emphasize the importance of returning for annual repeat screening regardless of their results from the baseline screening CT scan. The adherence message can be reinforced by including a brief reminder with their baseline screening CT findings report. Another approach is to increase staff training about the importance of follow-up screening and enhance sensitivity to the potential psychological concerns of screening participants. In one prior study, rates of adherence to repeat breast and cervical cancer screening increased with staff training. 26
There are several noteworthy study limitations. First, measurement of adherence was limited to the one year annual repeat CT scan. Rates of adherence to longer term follow-up scans may differ. Second, we did not measure several other participant level characteristics such as knowledge of lung cancer screening guidelines and other cognitive and affective processes (e.g. perceived benefit, anxiety, cancer worry) that may also influence adherence to annual repeat for lung cancer screening. Information about adequacy of medical insurance coverage, physician advice, and participant satisfaction with the baseline screening is also likely to influence long-term rates of screening adherence. 27 Collection of this information in future studies will help determine the need and focus for developing educational materials to enhance follow-up adherence in screening studies. Future research should also recruit a more heterogeneous and diverse sample in order to examine the generalizability of these findings to at-risk African Americans and Hispanics.
In conclusion, we have identified some of the factors associated with adherence to annual repeat screening for lung cancer. Currently, the US Preventive Task Force states that the evidence is insufficient to recommend for or against lung cancer screening. 28 However, within the next few years, the results of two large, ongoing RCTs and several large simulation modeling studies based on large, multi-site observational data will resolve uncertainty regarding the cost-effectiveness of lung cancer screening and provide evidence necessary for guiding health policy and care practices. When there is sufficient evidence to support both physician recommendation and insurance coverage for lung cancer screening, further studies will be needed to establish effective protocols for maintaining repeat adherence to follow-up CT scans. In the meantime, data describing adherence with repeat screening and treatment should be collected as part of standard protocol. 5 Likewise, enhanced educational and patient tracking efforts should be undertaken to insure high adherence with protocol follow-up recommendations for annual repeat screening. Our findings provide insights into targets for future interventions to promote adherence to forthcoming recommendations for lung cancer screening.
Sources of funding for the screenings
These were supported by grants from the National Institutes of Health R01-CA-63393, R01-CA-78905, The City of New York, Department of Health and Mental Hygiene, New York State Office of Science, Technology and Academic Research (NYSTAR), General Electric, Kodak, Empire Blue Cross and Blue Shield, The Starr Foundation, Ernest E. Stempel Foundation, The New York Community Trust, The Rogers Family Fund, and AMDeC Foundation, Inc.