
Abstract
Objectives
To assess the impact on equity of access of an organized breast cancer screening programme, compared with opportunistic breast and cervical cancer screening activities.
Methods
Two cross-sectional health interview surveys conducted in 1994 and 2006 in Catalonia (Spain), with 6382 and 7653 women participating in both surveys. The main outcome measures were having undergone regular mammography, and regular cytology. Age-standardized prevalence rates for both screening tests were computed using the direct method. The relative inequality index was computed to measure changes over time in inequality on screening utilization.
Results
Participation among women aged 50-69 has increased after the introduction of the organized breast screening programme; the greatest impact has been observed among those women with lower educational levels (from 17% in 1994 to 79% in 2006). Equity of access by education was particularly increased in the target group for breast cancer screening.
Conclusion
This study indicates that an organized screening programme could improve participation and equity of access.
Introduction
Screening activities can be carried out as an organized programme that requires (1) a defined target population, actively invited by the programme; (2) the use of homogeneous criteria and quality control activities; and (3) the evaluation of results and quality. 2 European guidelines for quality assurance in screening for both cancers, breast and cervical, clearly establish the implications of such organized programmes.5,6 Alternatively, opportunistic screening tests can be offered during contact between the woman and her physician in primary health care or in other healthcare settings. The main differences are that the opportunistic approach does not systematically invite the whole target population and it is more likely to result in variability in the definition criteria of the women invited and in the quality of the screening process, and reduces the possibility of systematically assessing the outcome of the screening activities at the population level.
The recommendations for screening differ for breast and cervical cancer in Catalonia: breast cancer screening with biennial mammography is recommended for all women aged 50-69, in the framework of an organized programme by the National Health Service that began in the mid-1990s and has covered the entire Catalan target population since 2002. This is not the case for cervical cancer screening, which is recommended only on an opportunistic basis in the framework of the primary healthcare setting. Its criteria are an age range of 20-65 and a three-year interval between tests, after two initial negative annual Pap tests. These different screening strategies offer an opportunity to assess the impact of the organized screening on the socioeconomic inequalities in access to these secondary preventive activities.
The Spanish healthcare system is defined by the universal coverage established in constitutional law, and it is organized following the National Health Service model. 7 The provision of health care, including preventive activities, is decentralized over 17 regions.
The introduction of breast cancer screening in an organized way, initiated by the Catalan Health Service, provides an opportunity to assess its impact on the equity of access to screening and to compare it with that of opportunistic cervical and breast cancer screening, which has had no change in policy.
Methods
We used individual data from two independent cross-sectional health interview surveys (Catalan Health Interview Survey) conducted in 1994 8 and 2006. 9 Both surveys had a stratified multistage sampling design. Participants were identified from the official registry of residents in Catalonia. The final samples included in this study were women aged 18 or older: 6389 women in 1994 and 7653 in 2006. To minimize non-response when the selected sampling units were not found or declined to participate, there was replacement by extra units in the same age group, sex group and neighbourhood. 9
Independent variables included in this study were age and educational level. We used 10-year groups except for age groups 60-64 and 65-69 due to the fact that, until 2002, theupperagelimitwas64forthewomeninvitedtothe breast cancer screening programme. Educational level was used in this study as a measure of socioeconomic status, and was based on the highest level attained: less than primary school, primary school, secondary school or university. The dependent variables used in this study were the regular performance of a mammography or Pap test as declared in the interview. The questions were ‘Do you have a mammography (breast X-ray)/cytology (Papanicolau test) done regularly?’. In the context of these surveys, regular meant 1-2 years interval for breast cancer screening and 1-5 years interval for cervical cancer screening. For the purposes of this analysis, three different options were considered: opportunistic breast cancer screening for women aged 40-49; organized breast cancer screening for women aged 50-69; and opportunistic cervical cancer screening for women aged 18-69.
Age-standardized prevalence rates for both screening tests were computed using the direct method and five-year groups; the standard population was the 2001 Catalan population. A chi-square test was applied to estimate whether two categorical variables were independent. Analyses have been done taking into account the adequate weighting of respondents and strata due to the complex sample design. 10 As a measure of temporal changes in inequality, the relative inequality index (RII) and corresponding confidence intervals were calculated from the prevalence ratio of a generalized linear model using a binomial regression.11,12 The RII takes into account the population size and socioeconomic position of cumulative groups. Educational level categories were assigned a value between 0 and 1, which represents the relative position of the central subject of the class. The RII expresses the risk for those at the bottom of the educational hierarchy compared with those at the top.13,14 Statistical analysis was carried out with SPSS v.13 software.
Results
Figure 1 compares participation in both screenings in 1994 and 2006; the highest increase is observed in breast cancer screening among women aged 50-69. The increase in prevalence of cervical cancer screening between both surveys is more important in women over 40.
Participation in breast (Mx) and cervical (Cyt) cancer screening, 1994 and 2006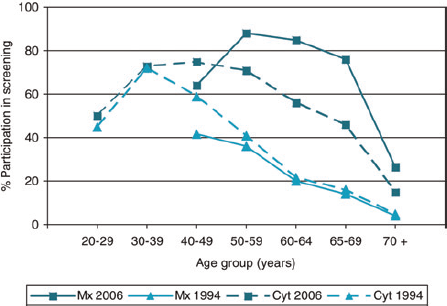
The prevalence of screening in both surveys by educational level is presented in Table 1. The highest increase is observed among women aged 50-69, the target group for the organized programme, and particularly in the lowest educational group. An increase in prevalence is observed for all screening strategies. These increases, although remarkable, are lower in the opportunistic setting, either in cervical or in breast cancer screening for women aged 40-49.
Distribution (age-adjusted prevalence rates) of women with preventive mammography/cytology test according to educational level, 1994 and 2006
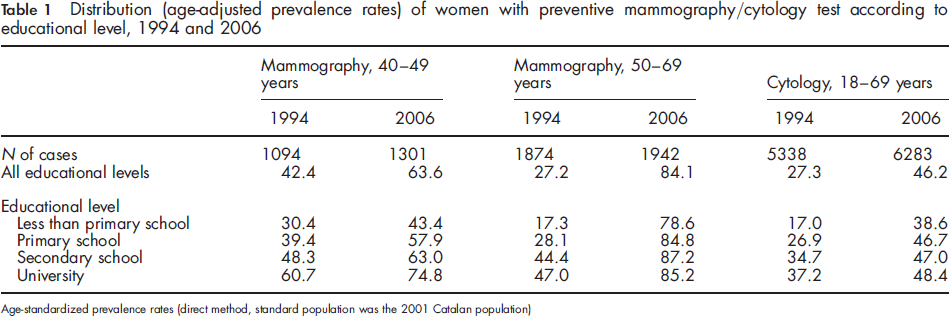
Age-standardized prevalence rates (direct method, standard population was the 2001 Catalan population)
The RII shows a reduction in 2006 as compared with the 1994 survey in all the screening approaches considered here, although the RII is still statistically significant in 2006 in the three cases (Figure 2). The greatest reduction is observed in the target age group for breast cancer in organized screening (ages 50-69), with an RII of 3.2 (95% CI 2.29-4.43) that is reduced to 1.2 (95% CI 1.08-1.23).
Relative inequality index (CI 95%) for breast and cervical cancer screening, 1994 and 2006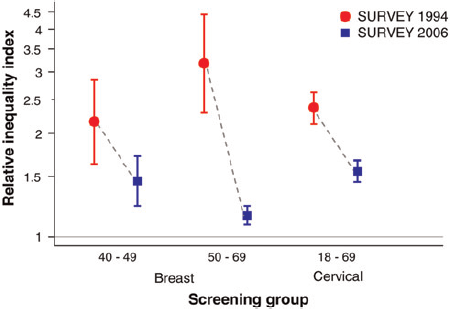
Discussion
The results of this study show a marked increase in the percentage of women self-reporting participating in breast cancer screening in 2006 compared with 1994. This increase is more important among women aged 50-69, the target population of the organized screening programme, compared with the women aged 40-49 or with opportunistic cervical cancer screening. The highest increase in participation was observed among women with a lower educational level. There was an inverse gradient in the relative changes between the 1994 and 2006 surveys: the higher the increase in participation, the lower the educational level. Thus, these results suggest that introducing an organized screening programme could be associated with a reduction in inequality of access to an effective test.
Organized screening programmes have improved access to preventive tests for invited women, and allowed the possibility to assess the quality of the process and its outcomes, which are necessary for further improvements to such programmes. 15 At the same time, organized screening programmes can narrow the educational gap in access, 16 and are a cost-effective strategy to carry out breast and cervical cancer screening.17,18 Inequality of access to cancer screening has been observed in countries with publicly-funded screening services, as well as in countries with a partial or complete lack of public funding for these activities.19-22 Comparison of participation among women in the target age group for the breast cancer screening programme with the Pap test cytology (with an opportunistic approach based on primary health care) shows the potential to improve access. Evidence to establish the impact of health programmes on the reduction of inequalities has been lacking, 23 but these results show that the impact could be relevant in organized screening programmes. Our results also agree with others from a different healthcare context. 24 Thus, organized screening programmes are an effective health activity that could be used as an example of the potential contribution of the health services to reduce health inequalities.
Participation in cervical cancer screening in this study has reached an upper limit in the younger age groups, with no change in the period analysed. Major changes have been observed in groups aged 50-69. The time elapsed between both surveys seemed to have been used by the health system to increase cervical screening in the older age groups while favouring participation of women in the lower educational groups. By comparison, utilization of mammography among women aged 40-49 plateaued, even in the light of intense public debate with some groups of health professionals and women promoting the extension of breast screening to this age group. However, the official recommendation for breast screening remains the same: biennial screening with mammography for women aged 50-69.
It is important to acknowledge that one of the problems associated with opportunistic screening, particularly but not exclusively with the Pap test, is the unnecessary annual repetition of the test, which implies an inefficient use of health resources. 18 In Spain, previous studies have shown that more than 50% of Pap tests are carried out in the public primary healthcare centres, without any cost to the user. 25 This suggests that the annual repetition of the test is not only related to economic incentives, but probably also to the health professional's recommendation.
The increase in screening participation from 1994 to 2006 among invited women was higher among the lower education groups. While there remains some differential inequity of access, it has markedly improved, as shown by more than 80% participation. 26
There are some limitations in this study. It was not possible to determine from the surveys whether the screening test was carried out in public or private health centres, or in the organized or opportunistic setting. Participation in the organized programme for breast cancer screening is now 65%. The difference in participation could give an estimate of the percentage of women who could access mammography outside the organized programme. Another factor is the accuracy of the self-reporting of preventive tests in surveys, which, according to a recent review, 27 is acceptable. A further limitation is the women's potential confusion of tests carried out with a preventive or a diagnostic intent.
Conclusion
Implementing an organized cancer screening programme aimed at a defined target group with active invitation reduces inequality of access to the preventive test. This potential benefit is higher among women with lower educational levels. Moreover, in this case, organized screening programmes increased the participation rate of the women invited, as compared with opportunistic screening. A health policy consequence is to support the implementation of an organized cervical cancer screening programme as a way of improving access to this test. Whether this observation would apply to other preventive activities, such as colorectal cancer screening, remains an open issue in the context of extending current pilot experiences. 28
Footnotes
Acknowledgements
This project was partially funded by the Instituto de Salud Carlos III (Network of Cooperative Research on Cancer, RD06/0020/0089).