
Abstract
Introduction
International studies on the effect of false-positive mammographic screening results on subsequent re-attendance at screening are inconsistent.
Setting Breast
Check, the national breast screening programme for the Republic of Ireland, screens women two-yearly. Re-attendance for subsequent screening is approximately 90%.
Objectives and Methods
The aim of this research was to quantify the impact of false-positive mammographic screening results on subsequent re-attendance, using the BreastCheck clinical database with a decade of screening and to determine if age group, assessment procedure, initial or subsequent screening, location of appointment for next screening round and time from recall to non-malignant diagnosis predicted re-attendance.
Results
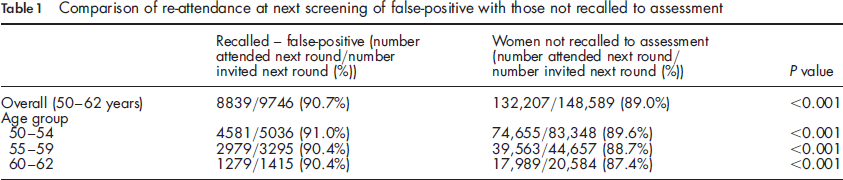
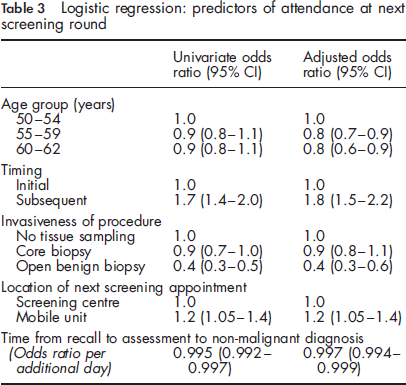
From programme commencement in 2000 to the end of 2007, 13,352 screening tests resulted in assessment; 11,765 participants were aged 50-62 years and of these 9746 received false-positive results (positive predictive value 17.2%). Following a false-positive recall to assessment, re-attendance at subsequent screening differed significantly by procedure type (open biopsy 80.3%; core biopsy only 90.2%; no tissue sampling 91.4%; P < 0.0001). Re-attendance differed significantly by timing of false-positive assessment in a woman's screening history (first versus subsequent screening, 89.5% versus 93.5%, P < 0.0001) and by location of next screening appointment (screening centre 89.8% versus mobile unit 91.3%, P < 0.01). The longer the period between recall to assessment and non-malignant diagnosis the less likely women were to re-attend. After logistic regression, first screening, older age, open surgical biopsy, re-invitation to screening centre and a longer period between recall and non-malignant diagnosis were significant negative predictors of re-attendance.
Conclusion
Since April 2008 BreastCheck has employed full field digital mammography throughout the programme, with a resulting increase in recalls; re-attendance will be closely monitored.
Introduction
BreastCheck, the National Breast Screening Programme, screens women aged 50-64 years throughout the Republic of Ireland every two years. 3 Screening is carried out at four screening units, each located in a major hospital campus, and at a number of associated mobile units. The overall positive predictive value for mammographic screening between 2000 and 2007 was 17.6%. Since April 2008 BreastCheck has employed full-field digital mammography (FFDM) only; this has been followed by an increase in cancer detection rate, but also an increase in recalls to assessment.3,4
While several papers have addressed the psychological effect of false-positive assessment, less is known about the predictors of re-attendance at next screening round. The aim of this research was to quantify the impact of false-positive mammography on subsequent re-attendance, using the BreastCheck clinical database with a decade of screening, and to determine if age group, the invasiveness of the assessment procedure, whether the woman was attending for a first screening or subsequent screening appointment, the time between recall to assessment and non-malignant diagnosis, and location of next screening appointment were associated with re-attendance in the next screening round two years later.
Methods
This was a retrospective cohort study, using the BreastCheck clinical database (2000-2009) focusing on a cohort of eligible women aged between 50 and 62 years, who attended screening from 2000 to 2007 and who were still eligible for screening in the subsequent screening round(s). The cohort of women selected allowed sufficient time for all to be invited for screening two years postassessment, to receive a reminder letter if necessary, and for the attendance to be determined.
Re-attendance is compared between those with a false-positive recall to assessment and those not recalled to assessment. In those with a false-positive recall to assessment, the effect of age group (50-54, 55-59 and 60-62 years), timing of false-positive assessment (initial or subsequent screening), invasiveness of assessment procedures (open surgical biopsy, core biopsy or no tissue sampling), time (in days) between recall to assessment and confirmation of non-malignant diagnosis, and location of next screening appointment (mobile unit or one of four screening centres) on subsequent re-attendance was determined.
The chi-square test was used for comparison of proportions and the t-test and analysis of variance used to compare means. Procedure type at assessment, age group, timing of screening (first or subsequent), screening appointment location (mobile unit or one of four screening centres) and time (in days) between recall and diagnosis were entered into a logistic regression model to determine independent predictors of non-attendance. SAS (version 9, SAS, Cary, NC, USA) was used for statistical analysis.
Results
From programme commencement in 2000 to the end of 2007, 13,352 women underwent screening mammography which resulted in recall to assessment. A total of 11,765 women were aged 50-62 years and of these 9746 (82.8%) received false-positive results (positive predictive value 17.2%).
Comparison of re-attendance at next screening of false-positive with those not recalled to assessment
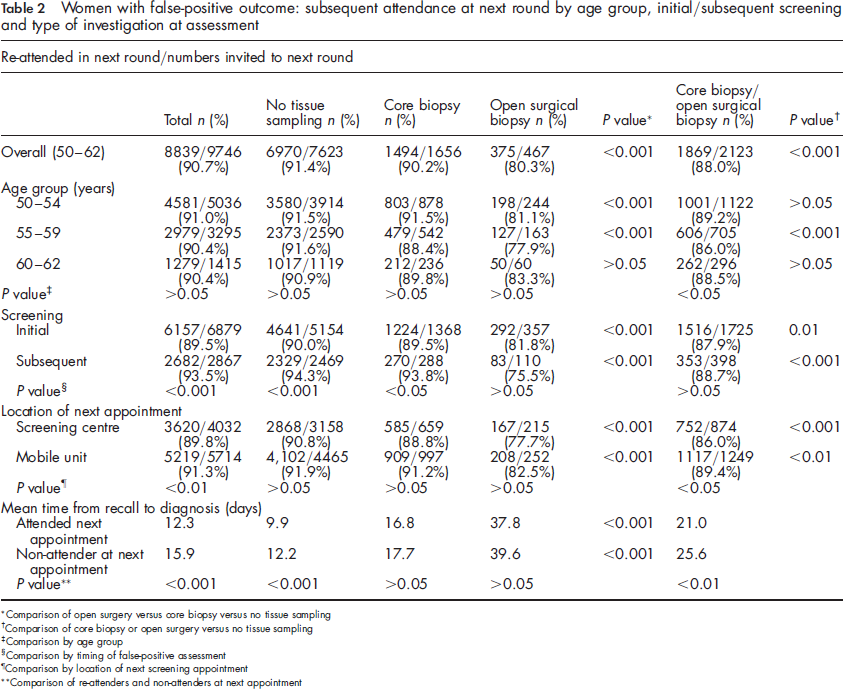
Women with false-positive outcome: subsequent attendance at next round by age group, initial/subsequent screening and type of investigation at assessment
Comparison of open surgery versus core biopsy versus no tissue sampling
Comparison of core biopsy or open surgery versus no tissue sampling
Comparison by age group
Comparison by timing of false-positive assessment
Comparison by location of next screening appointment
Comparison of re-attenders and non-attenders at next appointment
The proportions that attended after core biopsy, open surgical biopsy and after no tissue sampling were similar in each of the three age groups (Table 2).
Re-attendance at next screening round differed significantly by timing of false-positive assessment in a woman's screening history; those women who had a false-positive recall to assessment at their first screening were significantly less likely to re-attend in the next round compared with those women who had a false-positive recall to assessment at a subsequent screening visit (Table 2). This difference was seen in those who had no tissue sampling or had a core biopsy.
On univariate analysis age group did not have a significant impact on re-attendance, with just over 90% attending the next round in each of the three age groups.
Overall women who were invited post false-positive assessment to a mobile unit were more likely to attend for their next screening appointment than those invited to one of the four screening centres. The difference in proportions was small but significant (Table 2).
The average time in days from recall to assessment to confirmation of the non-malignant diagnosis was shorter for women who attended their next screening appointment. The time was significantly longer for those who had an invasive procedure compared with those who had no tissue sampling (Table 2).
Logistic regression: predictors of attendance at next screening round
Discussion
This study shows a clear distinction in re-attendance rates for women with a false-positive assessment depending on invasiveness of assessment, age at screening, and whether the assessment occurred at a first or subsequent screening visit. Older women, those women with a false-positive assessment at first screening and those who had a benign open surgical biopsy were significantly less likely to return for screening in the next round.
Previous studies have examined re-attendance rates and psychological consequences of false-positive mammography results, but we could find no previous study that has explored the effect of specific demographic and assessment variables on re-attendance in this way in a large screening population. Currence et al. 5 studied 170 cases and 176 controls and concluded that undergoing a biopsy, cyst aspiration or six-month follow-up after a positive mammogram does not deter women from undergoing screening mammography in the future. Our results concur but also show the effect of timing of the false-positive assessment in the screening history of the woman and the effect of age.
Women with a false-positive recall to assessment at initial screening were significantly less likely to return in the next round compared with those with false-positive recall to assessment at a subsequent screening. This suggests that women who have attended a number of times have a greater allegiance to the screening programme and perhaps have a greater understanding of mammography as a screening tool, with the inherent imperfections of screening versus diagnostic testing. In a comparative study of re-attenders and non re-attenders in the UK breast screening service (without recall to assessment) half of the women who failed to return implicated their initial visit in this decision. 6
The introduction of digital mammography in BreastCheck has led to a recent increase in cancer detection rates but also in recall rates. In a study of 188,823 screening examinations of women aged 50-64 years with 18.6% of mammograms obtained using FFDM, FFDM resulted in significantly higher cancer detection (6.3 versus 5.2 per 1000) and recall rates (4.0% versus 3.1%) than screen-film mammography. 4 The positive predictive values of FFDM and screen-film mammography were comparable. 4 Over 95% of cancers in BreastCheck are detected preoperatively with core biopsy. 3 Core biopsy is also the most common invasive procedure among those women found to be false-positive; in this study core biopsy of false-positive recalls was not an independent predictor of non-attendance at the next screening round, whereas those with an open biopsy were least likely to return.
There was a very small but significant difference in return to the next screening appointment if invited to one of the four regionally located screening centres as opposed to a mobile screening unit, which probably relates to distance or ease of access. We also found that women with a longer time between recall to assessment and final confirmation of non-malignant diagnosis were less likely to return at the next screening round; this finding is probably related to the longer associated period of anxiety.
We found that women who had a false-positive recall to assessment were more likely to attend in the next screening round; this difference was small but significant. Previous studies have shown inconsistent findings regarding re-attendance in the next round. Several studies in the UK and Canada have shown that women undergoing false-positive mammography were less likely to return for a subsequent screening appointment.1,7-9 However a systematic review of 23 studies found that US women who received a false-positive result were more likely to return for routine screening than those who received a normal result; 2 there was no difference among European women, and among Canadian women those with a false-positive assessment were less likely to return for screening.
It is considered that regional variations in handling of assessment procedures and false-positive cases may explain differences in uptake of screening re-invitations.1,10,11 Such findings suggest that the figures may be amenable to improvement through a change in practice. 1
BreastCheck has employed FFDM throughout the screening programme since April 2008, with a resulting increase in recalls to assessment. Although at present our figures do not suggest that, overall, those recalled to assessment and found not to have cancer are any less likely to return for screening at the next round, we have found clear differences depending on invasiveness of intervention and the timing of screening, and a smaller effect of longer time to diagnosis from recall and location of screening appointment. Re-attendance will be closely monitored to ensure the high rate of return of women for subsequent screening is not compromised.