
Abstract
Objective
To evaluate the attitudes and practices related to prostate-specific antigen (PSA) screening for prostate cancer (PC) among Finnish physicians in 1999 and 2007.
Materials and Methods
The first questionnaire survey was conducted in 1999 with a mailing to 102 urologists, 679 community physicians and 684 occupational health physicians identified from the membership files of three medical associations. The area of residence was divided into the study area of the Finnish PC screening trial and the rest of Finland. The second survey was carried out in 2007 targeting 168 urologists, 1039 community physicians and 938 occupational health physicians.
Results
The response proportion was 48% in 1999 and 50% in 2007. In both rounds, urologists regarded PC as a more important public health issue than other physicians. On the other hand, the non-urologists considered early diagnosis and screening more important than the urologists PC was rated by all physicians as a less important public health problem in 2007 than in 1999. A smaller proportion of urologists found routine PSA testing indicated for asymptomatic men, compared with other physicians (40% versus 74-60% in 1999, P < 0.001 and 35% versus 44-37% in 2007, P = 0.005). The proportion of physicians reporting regular PSA screening in asymptomatic men was reduced from 1999 to 2007 (from 18% to 9%, P < 0.0001).
Conclusion
Based on reported practices of Finnish urologists, community physicians and occupational health physicians, popularity of PSA testing declined between 1999 and 2007. Urologists found PSA testing among asymptomatic men justified less frequently than the other physicians.
Background
Major international organizations including the World Health Organization and International Union against Cancer have emphasized the importance of randomized trials before starting large-scale screening programmes, but some organizations, e.g. the American Cancer Society (ACS) and American Urological Association, have encouraged PC screening. 8 In 2010, the ACS updated its guidelines for testing for early PC detection with the recommendation that asymptomatic men who have less than a 10-year life expectancy based on age and health status should not be offered PC screening. 9
Recently, the European Randomized Study of Screening for Prostate Cancer (ERSPC) showed that PSA-based screening reduced the rate of death from PC by 20%, but was associated with a high risk of overdiagnosis. 10 Another randomized screening trial in the USA, the Prostate, Lung, Colon, and Ovarian Cancer Screening Trial, however, failed to show any mortality benefit. 11
The Finnish component of the ERSPC was started in 1996 in the Helsinki and Tampere metropolitan areas, with more than 80,000 men randomized. 12 The diagnostic examination of the screen-positive men and treatment of all cases in the screening trial (including screen-detected as well all other PC) are the responsibility of the public health system (primarily urology departments of the Helsinki and Tampere university hospitals) in accordance with standard practices.
We evaluated the attitudes and practices regarding PSA screening among Finnish physicians in two surveys conducted in 1999 and 2007. Such information is useful for evaluating contamination within the trial, i.e. prevalence of screening within the control arm.
Materials and Methods
The survey questionnaire was mailed to Finnish physicians identified from the membership files of three medical associations: the Finnish Society of Community Physicians (general practitioners), the Finnish Association of Industrial Medicine (occupational health physicians) and the Finnish Urological Association. These professional societies were chosen because their members were considered the physicians most likely to perform opportunistic screening for PC.
All primary care physicians with addresses in the Helsinki and Tampere metropolitan areas, and a randomly selected one-third of both community physicians and occupational health physicians from the rest of the country were selected. All members of the Association of Urology were included.
A questionnaire with 14 questions was mailed in 1999 to 102 urologists (all active members), 679 community physicians (452 residing in the trial area and 227 elsewhere) and 684 occupational health physicians (480 living in the Helsinki and Tampere metropolitan areas, and 204 in other parts of the country). No reminders were issued. In 2007, a similar questionnaire was mailed to 168 urologists, 1040 community physicians (545 and 495 with similar selection criteria as in 1999) and 938 occupational health physicians (679 and 259). Statistical significance of the differences in frequencies was evaluated using the chi-square test. Confidence intervals for proportions were calculated using the binomial distribution.
Results
In 1999, 703 questionnaires out of 1465 (48%) were returned, a response rate of 64% among urologists, 61% in community physicians and 44% for occupational health physicians. Excluding answers from the retired persons (n = 31), the material in the final analysis consisted of 645 questionnaires returned by 65 urologists, 316 community physicians and 264 occupational health physicians. Of these, 382 were from the screening study areas and 198 from other areas. In 2007 the response proportion was slightly higher, with 1066 questionnaires out of 2145 (50%) returned. Retired persons (n = 55), physicians not having adult male patients (n = 180) and questionnaires with no answers (n = 11) were excluded. The response proportion was 67% for urologists, 51% in community physicians and 46% among occupational health physicians. The analysis of the second survey included questionnaires returned by 96 urologists, 412 community physicians and 394 occupational health physicians.
In 1999, 90% of the physicians regarded PC as an important or very important public health issue and in 2007 the proportion was 82% (P < 0.0001). Correspondingly, the proportion of physicians who did not consider PC very important increased from 8% in 1999 to 17% in 2007 (P < 0.0001). Active treatment was perceived as important or very important by 93% of the respondents in 1999 and 87% in 2007 (P < 0.0001). The proportion reporting early diagnosis and screening important or very important also decreased from 83% to 67% (P < 0.0001). In 2007 a slightly lower age was thought to be appropriate for starting PSA screening (40-60 years versus 50-60 years).
The proportion of physicians reporting systematic use of PSA for early detection of PC among asymptomatic men during the past 12 months was nearly 20% (95% CI 0.16-0.23) in 1999 and only 10% (95% CI 0.08-0.12) in 2007. However, approximately nine out of 10 physicians indicated having used it occasionally at both surveys. In addition to screening, at least nine out of 10 physicians considered that a PSA test was indicated for men with urinary symptoms and for those requesting a test.
Attitudes toward prostate cancer and PSA testing in 1999 and 2007 by medical specialty
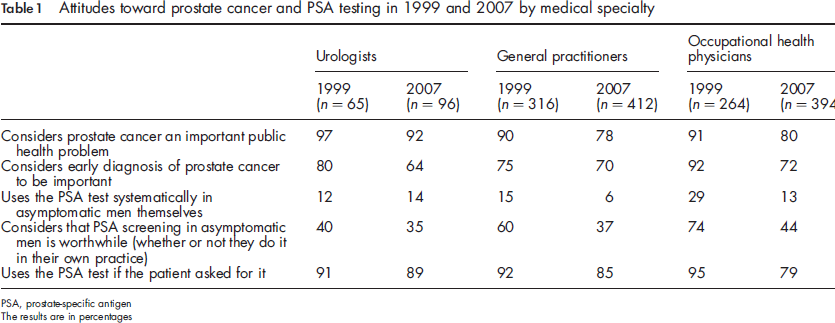
PSA, prostate-specific antigen
The results are in percentages
Physicians’ gender did not substantially influence screening practices in 1999 (18% of female and 19% of male physicians were using the PSA test systematically, P = 0.76). In 2007 male physicians were slightly more likely than female physicians (12% versus 6%, P = 0.004) to report systematic PSA testing and more frequently found screening of asymptomatic men justified (42% versus 35%, P = 0.28). Female physicians considered early diagnosis and screening somewhat more important than male physicians in 1999 (86% versus 80%, P = 0.004), but this difference disappeared in 2007 (68% in both groups, P = 0.54).
Geographical differences were not as striking as those between specialities. Physicians in the Helsinki and Tampere metropolitan areas reported a slightly higher use of the PSA test than physicians elsewhere. The primary care physicians in the study areas were more likely to use PSA testing in asymptomatic men than the other specialists: 44% versus 12-29% (P = 0.02) in 1999 and 20% versus 14-18% (P = 0.82) in 2007.
Discussion
Our study assessed the opinions and practices in the three groups of physicians primarily involved in the early detection of PC. The survey was repeated twice with similar methods to evaluate changes over a time period of eight years. Our main findings are a substantial decline in the popularity of PSA testing and considerable differences between medical specialities.
We obtained information from only half of the target group, which is suboptimal but not uncommon in questionnaire surveys.13, 14 The response rate was probably higher among those physicians who are involved in issues related to PC. The likely direction of possible selection bias is to overestimate the prevalence of PSA test use, if those most actively involved were over-represented among the participants.
Most earlier surveys on PSA use were published in the first half of the 1990s, when the use of PSA testing was still relatively new. 15 17 During those years, men were rarely aware of the possibility of PC screening, and the physicians’ advice was probably a major determining factor in their decision to be tested. 18 Increasing public knowledge of PSA screening has been reflected in a demand for testing in the population;8, 9 however, the adverse effects of screening such as risk of overdiagnosis and consequent overtreatment have also received attention.19,20
Our results show that attitudes among physicians changed considerably during the eight years between the first and second survey. PC was still considered an important public health issue by three-quarters of all physicians in 2007. More than 90% of urologists considered it important both in 1999 and 2007. The attitudes among the community and occupational health physicians did not change considerably between the surveys.
Only 9% reported using the PSA test systematically among asymptomatic men in 2007, which is half of that in 1999 (18%). In the late 1990s, evidence from surveys in ERSPC centres suggested an increasing rate of unorganized PC screening over time. 21 In the Rotterdam section of the ERCPC, which was reported in 2003, effective PSA contamination (routine PSA examination followed by biopsy, as indicated in the regular screening programmes) was low. Over a four-year rescreening interval, PSA contamination rates increased both in screening (13% to 24% in men aged ≥ 55 years) and control (9% to 14%) groups. 22 In the period 1998-2001 the estimated PSA contamination was 7% in a Spanish industrial area. 23
The proportion of physicians regarding the PSA test as important for detecting PC in asymptomatic men also decreased (approximately 75% in 1999 versus approximately 45% in 2007). However, the proportion of physicians who considered a man's own request to be sufficient to perform a PSA test remained very high (91-95% in 1999 and 79-89% in 2007).
Opportunistic screening is practised by some Finnish physicians, but only 18% of the physicians in this study reported using PSA screening systematically in asymptomatic men, although an additional 70% used the PSA test under some circumstances. This indicates that contamination is unlikely to seriously diminish the statistical power of the Finnish component of the ERSPC. The sample size calculations of the ERSPC have been performed under the assumption of 20% of the men in the control arm being screened 24 and the Finnish situation appears to match this assumption.
A survey on computerized databases from the UK shows that the rate of PSA testing of asymptomatic men doubled from 1.4% in 1994 to 3.5% in 1999, 3 but as the authors point out, the estimate may be too low, because it is possible that normal values are not always recorded on their database. A survey of 400 UK GPs carried out in 2003 showed that 76% had performed a PSA test on an asymptomatic man during the past three months. 25
The decreasing frequency of unorganized screening is consistent with the incidence trends of PC, which have turned downward after a strong increase in the 1990s and first years of the 2000s in Finland as in several other European countries.
Based on reported practices of Finnish urologists, community physicians and occupational health physicians, routine PSA testing among asymptomatic men was not very common in Finland in 1999 and 2007. The popularity of screening for PC decreased during the early 2000s.
Footnotes
Acknowledgements
The authors thank Anni Pehkonen for data entry. The Finnish randomized prostate cancer screening trial was financially supported by the Academy of Finland (grant no. 123054), Competitive Research Funding of the Pirkanmaa Hospital District and the Finnish Cancer Organisations.