
Abstract

Duffy et al. 1 estimated that between 2 and 2.5 lives are saved for every overdiagnosed case, which is 20-25 times more favourable than the estimate from the Cochrane review of the randomized trials. 2 They used a 38% reduction in breast cancer mortality from the Two-County trial, which is 2.5 times higher than the estimate based on all the trials.2,3 They also used UK data but contradict themselves. They consider the mortality stable in the unscreened age groups, but also report a significant 18% decline in breast cancer mortality in women aged under 50 years. The decline in the age group 50-69 years was 27%, and by using an unclear method described in a footnote, they concluded that screening conferred a further 28% mortality reduction. 1 This disagrees starkly with data from Cancer Research UK: women aged 40-49 (who were never invited to screening) had the same decline in mortality (44%) as those aged 50-64. 4
The graphs are misleading. Data for women below 50 years were lumped together, but as deaths from breast cancer before age 30 are extremely rare (12 cases in 2008), 4 the graph is close to the x axis, which conceals the huge decline in mortality in young women.4,5 Data from the age group 50-64 years were combined with 65-69 years, although screening of older women did not start before 2001, which conceals that breast cancer mortality in the age group 50-64 years began to decline before the UK programme started in 1988.4,5
Duffy et al.
1
substantially underestimate overdiagnosis. Firstly, they excluded carcinoma in situ, which was not stated in their paper. One of us asked Duffy on national radio whether he only included invasive cancer,
6
which he confirmed. Secondly, they used an unverified model with incorrect assumptions. It is wrong to assume that essentially all incidence increase with screening represents earlier diagnosis. Thirdly, they adjusted for a compensatory decline in breast cancer incidence in women no longer screened, which did not exist for the years they examined.7,8 More updated numbers show an abrupt increase when screening was extended to the age group 65-70 years in 2001 (Figure 1 below), which is far bigger than any possible recent compensatory decline. We estimated 57% overdiagnosis in England and Wales.
7
Duffy et al.
1
estimated that only 12% of cancers are overdiagnosed.
Incidence rates of invasive breast cancer in the UK per 100,000 women. Data from Cancer Research UK. Hatched lines: expected trends without screening. Screening introduced in 1988 in women aged 50-64 years, and in 2001 in women aged 65-70 years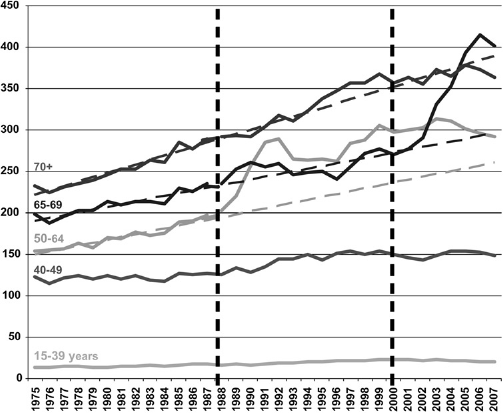
Duffy et al. 1 say they estimated the benefit directly from empirical data and looked at women actually screened, which they consider partly explains the disagreement with us about the benefit-to-harm ratio. They seem to imply that our data from the randomized trials are not empirical. Furthermore, it is not important for the ratio whether one looks at invited or attending women, as both benefits and harms increase among attendees.
Duffy et al. 1 claim that only 37% of breast cancers are screen-detected, based on a 200-word conference abstract where the sum of the relevant percentages is only 72%. They conclude that our estimate 7 implies that virtually all screen-detected cancers are overdiagnosed, which they consider ‘absurd and frankly incredible’. However, it is well known that between one-half and two-thirds of cancers are detected through screening, e.g. 68% of cancers were screen-detected in the relevant age groups in the UK in 2006,8,9 not 37%.
Duffy et al. 1 substantially overestimate benefits and underestimate harms. We also note that no conflicts of interest were declared. Tabár founded Mammography Education Inc, Arizona in 1980, which still exists, 10 and in 1999, he declared an income of five million SEK in Sweden, which is an extraordinary amount according to Nordic standards. We believe that such an important conflict of interest should be declared.