
Abstract
Objective
The aim of this study was is to examine uptake of population-based, flexible sigmoidoscopy (FS) screening delivered by nurses in a socioeconomically and ethnically diverse area of London, England.
Methods
All adults aged 58 and 59 years registered at 34 general practices in North London (n = 2260) were mailed an invitation to attend FS screening at the local hospital.
Results
In total, 45% (1024/2260) accepted the invitation and attended, 5% (114/2260) accepted the invitation but failed to attend, 5% (111/2260) accepted the invitation but were unable to attend within the time-frame of the pilot study, 7% (165/2260) declined the offer, 27% (602/2260) did not respond, and 11% (244/2260) were ineligible or did not receive the invitation. Among those eligible to be screened, the uptake rate was 51% (1024/2016). Uptake did not differ by gender, but people living in the most affluent quintile of areas had a substantially higher uptake rate (63%) than those living in the most deprived quintile (38%).
Conclusion
Uptake of FS screening delivered as a population-based programme was over 50% among the eligible population in a socioeconomically and ethnically diverse area of London. Disparities in uptake should be addressed to avoid exacerbating health inequalities.
Introduction
Flexible sigmoidoscopy (FS) screening, which is one of the screening modalities offered in the US, 6 has the additional potential to reduce CRC incidence by removing the adenomas which are the CRC precursor lesions. FS screening is currently under evaluation in Italy, the USA, Norway and the UK. 7 10 Recent results from the UK FS Trial, in which adults aged 55-64 were given a single FS examination, show that CRC incidence was reduced by a third and mortality by 43% over the 11-year follow-up period among people attending FS screening. 11
Crucial to the success of any screening programme is achieving adequate uptake across the whole eligible population. In the USA, FS uptake rates are low (10% on self-report), 12 but it is only one of several CRC screening modalities that are recommended. Uptake rates were over 70% in the screening arm of the UK FS Trial, 10 but because of the two-stage invitation procedure, only individuals who had previously indicated that they would be likely to accept a screening invitation were randomized to screening versus control. This is likely to overestimate the uptake rates that could be expected if FS were offered to all eligible adults as part of a population-based programme.
A small feasibility study of nurse-led FS offered as a screening service was carried out in a sample of 510 adults in a relatively affluent area of London (Harrow). Uptake was 55% in the whole invited population and 67% in the eligible population (those with correct address information and not meeting any medical exclusion criteria). 13 This is lower than the uptake in the FS Trial, but comparable with the 52% uptake reported in the second round of the English FOBT Pilot Study, 14 and higher than the FOBT uptake rate in the London area as a whole in the first 30 months of the National Bowel Cancer Screening Programme (NBCSP). 15
The purpose of the present analysis was to examine uptake of nurse-led FS in a larger, more socioeconomically diverse population.
Methods
Participants and setting
All men and women aged 58 and 59 years old registered at 34 general practices in the Harrow and Brent areas of London (n = 2260) were invited to attend nurse-delivered FS screening at the local hospital. Because these individuals were less than 60 years old, they would not have previously been invited for CRC screening. General practices were selected based on the Index of Multiple Deprivation (IMD) 16 to ensure a wide range of socioeconomic deprivation in their constituent populations.
The study took place between November 2006 and May 2008, with Harrow residents being invited between November 2006 and August 2007, and Brent residents between November 2007 and April 2008. Harrow is a slightly more affluent borough than the English average, while Brent is the 53rd most deprived borough out of 354 in England. Both boroughs are ethnically diverse, with only 59% of residents in Harrow and 45% of residents in Brent from a White ethnic background, compared with 92% for the UK as a whole. Ethical approval was granted by the Harrow Research Ethics Committee.
Invitation procedure
Because there was no national publicity for the programme, we mailed a ‘flyer’ to eligible individuals informing them that ‘bowel screening using the Flexi-Scope Test’ would be starting in their local hospital. This was followed up with an invitation offering a dated and timed screening appointment approximately six weeks later. Participants were asked to return the reply slip at the bottom of the letter or call the ‘Flexi-Scope Office’. Enclosed with the invitation was an information leaflet about CRC and FS, a picture illustration showing how polyps transform to cancer and are removed during the FS test, 17 a prescreening questionnaire, and a freepost return envelope.
After two weeks, a reminder of the initial appointment and a leaflet addressing common barriers to FS screening 18 was sent to people who had not responded to the initial invitation. After this, a second invitation with a new appointment date was sent to non-responders. All communications included ‘return to sender if undelivered’ instructions on the reverse of the envelope.
Following acceptance of an appointment, participants were sent a confirmation letter along with a bowel preparation (enema) with instructions for self-administration and a map of the clinic location.
Assessment of uptake
Eligible participants were defined as those who did not meet the exclusion criteria and whose invitation letter was not returned undelivered. Exclusion criteria included: recent/pending bowel surgery; current active treatment for cancer, other serious illness (e.g. epilepsy, renal failure); diagnosis of colitis or Crohn's disease; mobility restrictions; away from home for duration of study; and deceased. Participants were classified as ‘attended’ if they underwent FS with one of the three specialist nurse endoscopists.
Gender and age were known from information obtained from the general practice, and socioeconomic deprivation was indexed by the IMD rank score for each individual's home address.
Statistical analysis
Data were analysed with SPSS version 17.0. T-tests were used to examine differences in IMD scores and univariable logistic regression to examine differences in uptake by gender, deprivation and location. Multivariable logistic regression compared uptake rates between men and women, across quintiles of deprivation, and between the two boroughs.
Results
Sample characteristics
Of the 2260 individuals invited to participate, 52% (n = 1176) were male and 48% female (n = 1084), and their average age was 59.2 years. The mean IMD rank score of the home addresses of individuals invited for screening was 14,016 (range 780-31,383), which represents slightly higher deprivation than the average for England. The mean IMD rank score for Brent residents (10,837) was significantly lower than for Harrow residents (18,106; t(2258) = 31.4, P < 0.001) reflecting Brent's greater deprivation.
Response to the different stages of the invitation procedure
Of the 2260 initial invitations sent, 27% (604/2,260) elicited an immediate response to accept (16%), rearrange (6%), postpone (2%) or decline (2%) the appointment. Two weeks later, a reminder was sent to the 1471 non-responders, which yielded a very similar pattern of responses, with 29% (664/2260) getting in touch with the ‘Flexi-Scope Office’ to accept (14%), rearrange (8%), postpone (3%) or decline (4%). A second invitation for screening on a different date was sent to 30% (690/2260) of non-responders, of whom 7% (150/2260) responded to accept (3%), rearrange (1%), postpone (1%) or decline (1%).
Uptake
Overall outcomes to the invitation process
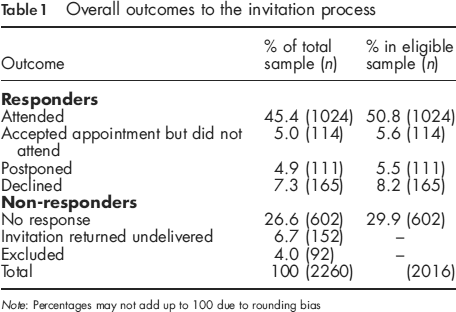
Note: Percentages may not add up to 100 due to rounding bias
Excluding the individuals for whom we had incorrect contact details or who did not meet the eligibility criteria resulted in an eligible sample of 2016 people. The uptake rate for the eligible sample was 51% (Table 1).
Uptake by gender, deprivation and location in the eligible sample
Uptake by gender, quintiles of the Index of Multiple Deprivation and location in the eligible sample (n = 2016)
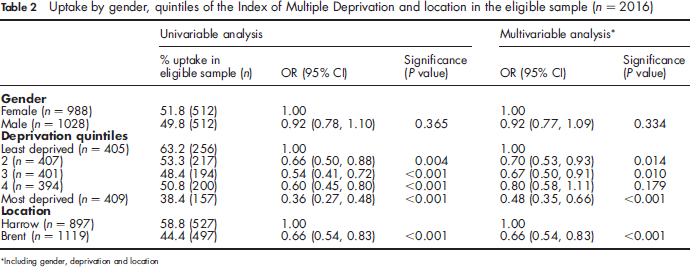
Including gender, deprivation and location
The IMD ranks of each individual's home address were divided into quintiles of deprivation. Analysing uptake by quintile of deprivation showed an uptake rate of 63% for those living in the most affluent quintile compared with 38% for those living in the most deprived quintile, with an almost linear gradient in uptake across intermediate quintiles.
Uptake rates also differed significantly in the two boroughs, with 59% of participants living in Harrow attending compared with 44% of those living in Brent.
In multivariable analysis (Table 2), Including gender, deprivation and area, there was no gender effect and no interactions between gender and either deprivation or area. As with the univariable analysis, there was an almost linear relationship between deprivation and uptake, with the most deprived quintile having the lowest uptake. Uptake remained significantly lower in Brent, suggesting that factors other than deprivation explained the difference between the boroughs.
Discussion
The aim of the present study was to assess FS uptake rates when the screening test was delivered as if in a population-based programme, in an area of London with considerable socioeconomic and ethnic diversity. The unadjusted overall uptake rate for FS was 45%, rising to 51% after exclusion of individuals for whom the invitation letter was returned because the address was incorrect or who were ineligible on medical grounds. This was lower than the 55% (67% in the eligible population) observed in our previous feasibility study, but that was conducted exclusively in the more affluent Borough of Harrow. 13 The unadjusted uptake rate in Harrow alone in the present sample was 53%-very close to the previous feasibility study results.
Across both boroughs combined, uptake was almost twice as high in the least deprived than the most deprived quintile of addresses (63% versus 38%). This echoes results showing a striking socioeconomic deprivation in FOBT uptake both in the pilot programme 14 and in the first 30 months of the national rollout of the NBCSP in London. 15
There was evidence for an effect of geographic area even after controlling for socioeconomic deprivation, with Brent residents being significantly less likely to attend FS screening than those living in Harrow. One possible explanation was the greater ethnic diversity in Brent. We did not have ethnic information on the participants in this study, but ethnicity has been shown to be a significant independent factor in CRC screening uptake in previous studies.15,19
The present study found women's uptake to be marginally (2%) higher than men's, although the difference was not significant. This contrasts with previous research which has observed higher uptake of FS in men.8,10,20 One explanation could be that the screening examinations in the present study were described as delivered by ‘nurses’, who are often assumed to be female. Women may perceive the procedure to be less embarrassing if conducted by a woman, and their preference for a female endoscopist has been noted previously. 21
The present study also made some interesting observations on the invitation procedure. In response to the first invitation, 22% of participants accepted or rearranged the appointment, and the reminder yielded the same response (22% accepting or rearranging). But a second invitation with a new appointment time elicited only a 5% acceptance. This suggests either that further contact yields diminishing returns or that an alternative appointment date does not tackle the appropriate barriers.
Comparisons with FOBT uptake in the NBCSP are interesting because both tests screen for CRC; but whereas FOBT is done at home, FS requires a visit to the hospital for an intrusive and uncomfortable examination. The most recent data from the London Screening Hub show a return rate of 47% for FOBT kits in Harrow and 40% in Brent. 22 These figures are close to the unadjusted FS uptake rates of 53% in Harrow and 39% in Brent. This close match for uptake of the two forms of screening is striking given the differences in the procedures. Interestingly, both procedures also show a strong socioeconomic gradient. London-wide, the gradient in FOBT uptake across quintiles of deprivation (at the postcode sector level) was from 32% to 49%, 15 while within Harrow and Brent the gradient across IMD quintiles in FS uptake was from 38% to 63%. Regardless of whether CRC screening is a simple home-based procedure-albeit somewhat distasteful-or an intrusive medical test done in a hospital, lower socioeconomic status individuals are much less likely to participate.
Recent data from the UK FS Trial have shown an impressive 33% reduction in CRC incidence and 43% reduction in mortality in the screened sample. However, delivery of this benefit in a population-based screening programme depends on adequate uptake rates. This analysis shows that in a socioeconomically and ethnically diverse area of North West London, uptake of nurse-led FS was at least comparable with FOBT return rates and appeared to be as acceptable to men as women. However, socioeconomic deprivation remains a pervasive barrier to CRC screening regardless of modality. Research to address socioeconomic disparities in screening participation is urgently needed to ensure that implementation of bowel cancer screening does not increase inequalities in cancer mortality.
Footnotes
Acknowledgements
Support from the Department of Health and Cancer Research UK is gratefully acknowledged.