
Abstract
Objective
To illustrate regional changes that occurred in screening for Down's syndrome (trisomy 21) in England and Wales from 1989 to 2008.
Methods
The National Down Syndrome Cytogenetic Register has collected data on all ante- and postnatal diagnoses of Down's syndrome in England and Wales since 1989 (n = 27,954). The percentages of (i) diagnoses made antenatally, (ii) antenatal diagnoses that had nuchal translucency (NT) measured, and (iii) antenatal diagnoses in mothers aged 37 and over with advanced maternal age as the sole recorded indication for diagnosis are presented according to where the mother lived (Government Office Region), year of diagnosis (1989–1994, 1995–2000, 2001–2006, 2007–2008), and maternal age (<37 years, ≥37 years).
Results
The percentage of cases diagnosed antenatally has increased in younger women but varies between regions. It remained relatively constant at approximately 70% in older women. The use of NT measurement in antenatal screening has expanded rapidly but varies regionally, being most common in London and the South East where, in 2007–2008, over 75% of antenatal diagnoses in older women had NT measured. The sole indication of advanced maternal age has substantially reduced, and was less than 10% in older mothers in all regions in 2007–2008.
Conclusions
There are regional and maternal age variations in Down's syndrome screening and diagnosis. Some regions used NT measurements, and eliminated advanced maternal age as sole reason for antenatal diagnostic testing more quickly than others. The reasons for variations need to be identified and addressed to ensure that when new screening techniques become available, regional differences are minimized.
INTRODUCTION
Down's syndrome (trisomy 21) is strongly associated with maternal age. Prior to 1988 maternal age was used as a screening test in England and Wales, with ‘older’ mothers (usually those aged 37 and over) being offered an invasive diagnostic procedure to determine if the fetus had Down's syndrome. Screening for Down's syndrome using the double test and triple test was introduced shortly after 1988. These screening tests analyse serum levels in maternal blood, and combine them with maternal age to assign a risk of the pregnancy having Down's syndrome. Women with estimated risk above a cut-off (e.g. 1 in 250) are then offered an invasive diagnostic test. Further advances include the use of ultrasound nuchal translucency (NT) measurements in the first trimester in screening for Down's syndrome. In 2003 the National Institute for Clinical Excellence (NICE) first recommended that all pregnant mothers should be offered screening, and an NT measurement is a component of the combined test that is currently recommended by NICE. 1 Despite national guidelines about screening for Down's syndrome, there are known to be differences in the screening provided around the country. 2
This study maps the changes in percentage of cases diagnosed antenatally across England and Wales according to Government Office Regions (GOR) between 1989 and 2008. It also maps the use of NT measurements in pregnancies with antenatally diagnosed Down's syndrome, as an example of the spread of new screening technologies, and the decrease in diagnostic testing indicated solely by advanced maternal age, as an example of the decline in less effective screening strategies.
METHODS
The National Down Syndrome Cytogenetic Register (NDSCR) was established in 1989, and collects anonymous data on all cytogenetic diagnoses of Down's syndrome in England and Wales. 3 The information is derived from all clinical cytogenetic laboratories, which are requested to send a completed form for each diagnosis of trisomy 21 and its variants. The form contains details of the date, place of and indications for referral, maternal age, family history, maternal postcode, and home town. Most laboratories send a copy of this form to the referring physician for confirmation and completion. The outcome of the pregnancy is requested for all cases diagnosed antenatally. It is estimated that the NDSCR ascertains 93% of all cases. 4 It includes 27,954 antenatal and postnatal diagnoses recorded between 1989 and 2008, 15,164 (46%) of which were antenatal.
The data are presented by GOR for England, the primary classification for the presentation of regional statistics. They are: East of England, South East, London, South West, East Midlands, West Midlands, North West, North East, and Yorkshire and The Humber. Wales is separate. GOR is derived from mother's postcode or home town in 93% of NDSCR cases. For the remaining cases, GOR is assigned according to the hospital at which diagnosis took place. GOR cannot be identified for 0.3% of Down's syndrome diagnoses and these cases are excluded from the analysis.
Analyses are presented for the periods 1989–1994, 1995–2000, 2001–2006, and 2007–2008. The 2007–2008 data are based on smaller numbers and are therefore potentially less accurate; however they give the best indication of regions' recent performance and are unlikely to be biased, so are therefore considered important.
Because of historical differences in screening and diagnostic testing according to maternal age, analysis of the percentage of cases diagnosed antenatally and the percentage of antenatal diagnoses having NT measured is carried out separately for maternal age under 37 (‘younger’ mothers) and 37 and over (‘older’ mothers). In 5% of records maternal age is missing, so these are not included in the analysis. Advanced maternal age results are reported for maternal age 37 and over (‘older’ mothers) only.
The use of NT measurements is classified as ‘yes’ or ‘no’ according to whether there is any indication on the notifying form that NT was measured. More recent forms ask specifically whether NT was measured, but some earlier forms did not. NT is assumed to have been measured when (1) indication for karyotype was a screening test that included NT (e.g. combined, integrated, OSCAR, PRIMARK); or (2) there was a record in the notes of NT having been measured; or (3) ‘nuchal fold/oedema/thickening/translucency/cystic hygroma’ had been coded as an ultrasound finding (in an early version of the form) and gestation at sample or outcome was before 16 weeks; or (4) ultrasound scan was reported as the indication for karyotype and gestation at sample or outcome was before 16 weeks; or (5) absent nose or nasal bone was noted, since this is assessed in conjunction with NT measurement.
Forms without any mention of screening or ultrasound having been performed, and with ‘advanced maternal age’ recorded as the only indication for diagnosis from a list of options, or noted on the form, are classified as ‘advanced maternal age’ being the only indication for antenatal diagnostic testing.
Maps were created using the command ‘spmap’ in Stata, with outlines from Digitized Boundary Data (England and Wales). 5
RESULTS
Figure 1 shows that Down's syndrome pregnancies in younger mothers were less likely to be diagnosed antenatally than those in older mothers in each region in each time period (see Web-tables 1 to 3 for results used to produce Figures 1 to 3). Since 1989–1994 there have, however, been increases in the percentage of cases diagnosed antenatally in every region for younger women. In 2007–2008 the East of England antenatally diagnosed 68% of cases in younger women, and 79% of cases in older women, compared with 28% and 77% respectively in 1989–1994.
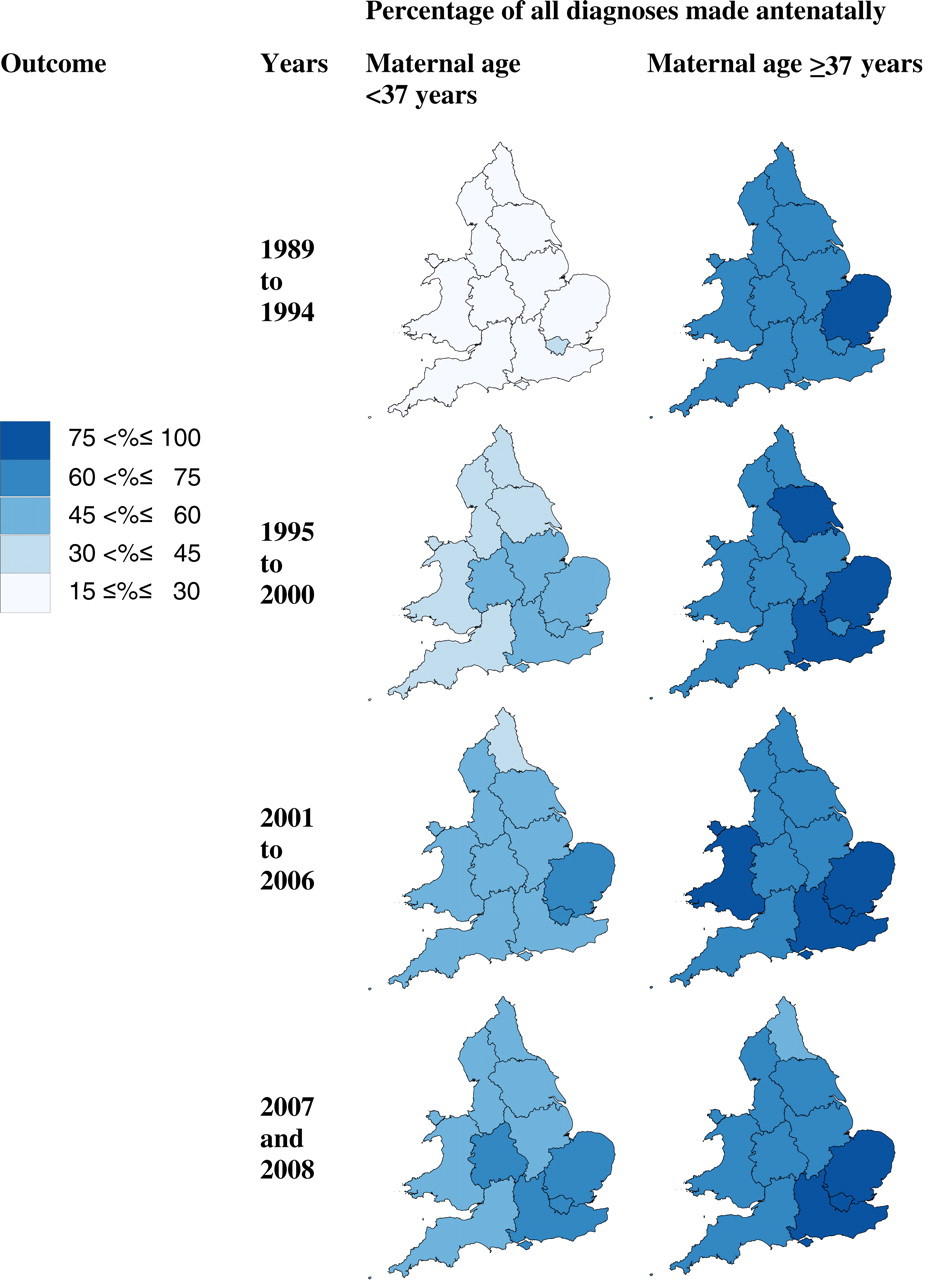
Percentage of Down's syndrome diagnoses made antenatally in England and Wales from 1989 to 2008 according to mother's area of residence and age
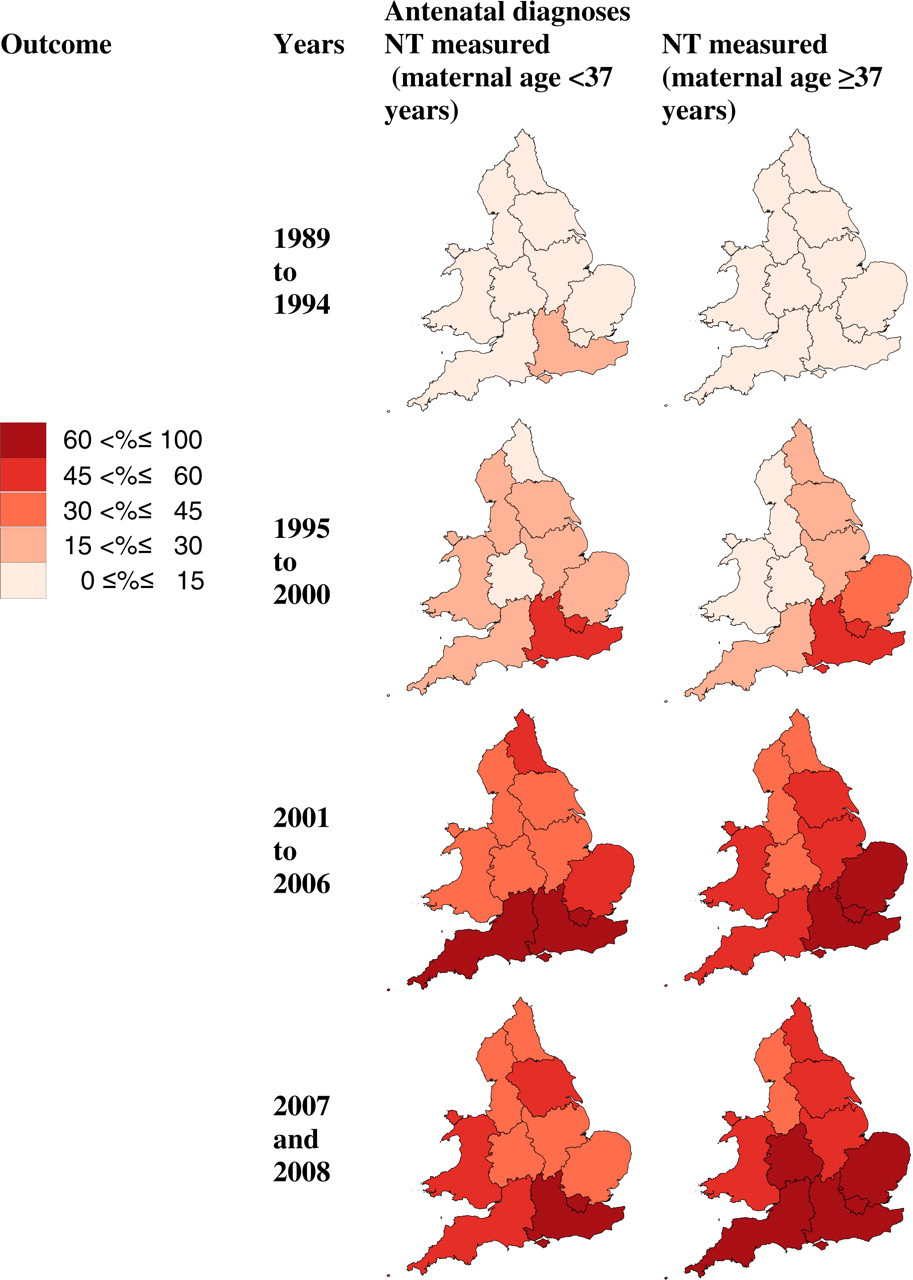
Percentage of antenatal diagnoses that had NT measured in England and Wales from 1989 to 2008 according to mother's area of residence and age
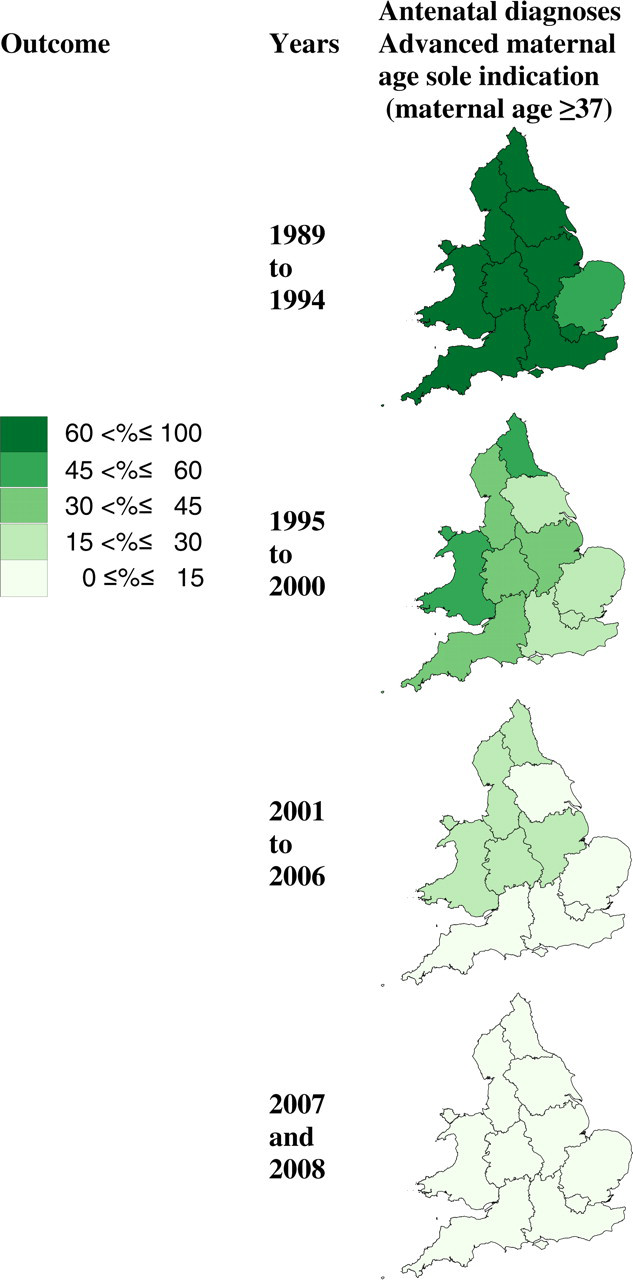
Percentage of antenatal diagnoses in women ≥37 years with advanced maternal age as the only reason for diagnostic test in England and Wales from 1989 to 2008 according to mother's area of residence
The East of England diagnosed the greatest percentage of cases antenatally in younger women in 2007–2008 (68% of 133 diagnoses), but other GORs lagged behind, for example Yorkshire and the Humber (45% of 133 diagnoses) and the North East (46% of 79 diagnoses). Regional variation was also evident in older mothers: in 2007–2008 the East of England diagnosed 79% of 211 cases antenatally, whereas the North East diagnosed 58% of 59 cases antenatally and the South West diagnosed 65% of 167 cases antenatally.
Figure 2 illustrates the rapid growth in the use of NT measurements in antenatally diagnosed cases of Down's syndrome, the slight difference in its use between younger and older mothers, and the clear difference in its use between regions.
In 2007–2008 the greatest difference between older and younger mothers within a region was in the East of England where 43% of 91 antenatal diagnoses in younger mothers had an NT measured, compared with 69% of 167 antenatal diagnoses in older mothers. Antenatally diagnosed mothers in London and the South East (where the Fetal Medicine Centre, pioneering the use of NT, is located) were the most likely to have had NT measured in every time period after 1989–1994: 77% of antenatal diagnoses in 333 and 222 older mothers respectively in 2007–2008, and 68% in 211 and 70% in 188 respectively in younger mothers. In 2007–2008, antenatally diagnosed mothers in the North West were the least likely to have had NT measured: 32% of 96 younger mothers and 45% of 110 older mothers.
Figure 3 shows the rapid decline in use of advanced maternal age as the sole indicator for antenatal diagnosis. It was the only indication recorded in over 55% of all antenatal diagnoses in older mothers in every region in 1989 to 1994. By 2007–2008, it was the sole indication in less than 10% of antenatal diagnoses in all regions.
DISCUSSION
These findings confirm improvements in antenatal diagnosis of Down's syndrome, but also expose persistent regional differences. The use of NT measurements in antenatally diagnosed cases of Down's syndrome has expanded rapidly and was most commonly used in London and the South East where, in 2007–2008, antenatal diagnoses in young women were more than twice as likely to have had NT measured than in the North West. In contrast, the indication of advanced maternal age in antenatal diagnosis of Down's syndrome has substantially reduced as better screening tests have become available.
The major strength of this study is the coverage and quantity of the data. The NDSCR has ascertained over 93% of Down's syndrome diagnoses made in England and Wales since 1989, 4 totalling more than 27,000, providing the opportunity to examine trends in the regions over time. The only other national dataset on Down's syndrome in England and Wales is that collected by the National Congenital Anomaly System, which is too incomplete to make meaningful comparisons. 4,6 Regional congenital anomaly registers collect data that enable monitoring of some regional trends, but these registers cover only around 55% of all births in England and 100% of all births in Wales. The percentage of cases excluded due to missing GOR or maternal age in this study is small.
For 7% of records, region was derived from hospital of diagnosis so it may not accurately reflect the region of mother's residence. Equally, some mothers whose region was derived from the home postcode may have travelled outside the region for screening and/or diagnosis. As the percentage is small there is no reason to expect this to have a major impact on results, particularly since the reason for missing postcodes/home towns is largely administrative.
Pregnancies in which Down's syndrome was postnatally diagnosed were excluded from the analysis of NT use because of poor completion of questions about methods of screening, which might be because obstetricians or paediatricians were unaware of whether or not the mother had been screened or, if she had been, of the method used. Data about Down's syndrome screening and, specifically, NT measurements in the general population of pregnant mothers are not available. Since the outcome of the pregnancy is not known when screening is carried out, it is reasonable to assume that the screening experience of mothers with an antenatal diagnosis of Down's syndrome is representative of all mothers having antenatal screening. However, the use of NT in the study population will somewhat exaggerate the use of NT measurement in the general population. This is because screening tests that include an NT measurement have higher detection rates than tests without an NT measurement, so the percentage of antenatal diagnoses (i.e. detected cases, the study population) that had an NT measurement will be larger than the percentage of all pregnant mothers who had an NT measurement. This bias will be consistent for all regions and time periods, and will not affect comparisons between them, so there is no reason to believe that the regional variations or trends over time for all pregnancies differ from those studied.
Before the widespread use of NT measurement in Down's syndrome screening there was no explicit ‘yes/no’ question on the NDSCR data collection forms about it, so NT measurement may have been under-ascertained in the early years. This is unlikely to have greatly affected time or regional trends, since there is no reason to expect clinicians' recording of the use of NT on NDSCR forms to be biased by calendar years or region.
The difference between antenatal diagnosis percentages in younger and older mothers in the early years reflected the use of maternal age screening (in which all women older than a specified cut-off age were offered a diagnostic test) and of early serum screening tests, which for a fixed risk cut-off had lower detection rates amongst younger women. For a 1:200 mid-trimester cut-off the detection rate for the triple test in women aged 25–29 is 61% versus 87% in women aged 35–39. 7 The increase in antenatal diagnosis percentages through time in younger women reflects the widespread introduction of and improvements in serum screening and, latterly, NT measurements in combination with serum. For a 1:200 mid-trimester cut-off the detection rate for the combined test in women aged 25–29 is 74% versus 88% in women aged 35–39. 7 Different percentages of Down's syndrome cases being detected will also be influenced by a different uptake of both screening and diagnostic tests.
The maps demonstrate the spread of the use of NT measurement in screening. There are genuine obstacles to the roll-out of NT measurement, and it is preferable that it is not introduced until the service can be of a high quality. There was initial concern about NT measurements being used to screen for Down's syndrome which, combined with the shortage of sonographers trained in NT, and the time and resources needed to gain that training, could explain the delay in implementation in some regions. 8–10 Also, NT has to be measured between 10 weeks 6 days and 13 weeks 6 days gestation, so if some regions have higher proportions of pregnant mothers initiating antenatal care late this would lower the percentage of antenatal diagnoses that had NT measured. Screening tests that include serum and NT measurements have, however, been shown to achieve higher detection rates than serum-only tests, 7,11 and should be a priority in every region.
The increases in antenatal diagnoses and in the use of NT measurements in screening observed in this study can be expected to continue as NICE currently recommends offering screening to all women using the combined test (serum and NT measurements). 1 Meanwhile the regional differences have important implications for pregnant women: not only their chances of having Down's syndrome diagnosed antenatally, but the timing of that antenatal diagnosis and therefore, if chosen, the timing of termination. Regions that continued to use advanced maternal age alone once better screening tests were available (and regions that have been slow at introducing NT into their screening tests) may have performed invasive diagnostic procedures that could have been avoided by using serum and NT screening tests.
The findings in this study have implications for the introduction of future screening advances. Pathways need to be in place to ensure that new techniques are implemented in a timely fashion (while ensuring high-quality performance) throughout the country, so that the regional differences still evident in the use of NT measurements are avoided. To this end, the obstacles to the introduction of new techniques need to be understood and minimized where possible.
Source and copyright of data used to create maps
Source: 2001 Census, Output Area Boundaries. Crown copyright 2003. Census output is Crown copyright and is reproduced with the permission of the Controller of HMSO and the Queen's Printer for Scotland.
Details of ethics approval
The National Down Syndrome Cytogenetic Register (as part of the British Isles Network of Congenital Anomaly Registers) has multicentre research ethics committee approval from Trent MREC. It was granted section 60 class support under the Health and Social Care Act 2001 for the collection of personal information without consent.
Funding
The NHS Fetal Anomaly Screening Programme funded the NDSCR to collect the data until March 2009.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.