
Abstract
Background
Computed tomographic (CT) colonography (or ‘virtual’ colonoscopy) has become an increasingly popular tool for colorectal cancer screening. Colonic perforation, an uncommon complication, is a risk that has not been widely reported.
Methods
A systematic review of the literature was undertaken to identify all reported risk factors for colonic perforation following CT colonography. In addition, a retrospective multicentre study was undertaken, evaluating all CT colonographies in 10 major metropolitan tertiary referral centres. All colonic perforations were assessed for risk factors.
Results
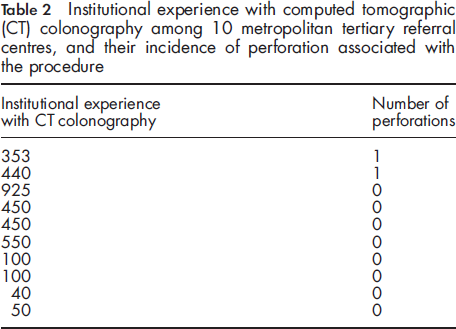
A range of ‘patient’-related and ‘procedure’-related risk factors were identified in the literature. Among 3458 CT colonographies, there were two cases of colonic perforation contributing to an incidence of perforation of 0.06%. There was no statistical correlation between the incidence of perforation and institutional experience (P = 0.66). Risk factors common to both cases and the literature included age, recent colonoscopy and manual colonic insufflation. Diverticular disease and recent colonic biopsy were also notable factors.
Conclusion
There is a small but real risk of perforation following CT colonography. Patient selection and preventative procedural measures may reduce this risk. The importance of the consent process is emphasized.
Background
While sporadic reports of perforation have enabled some analysis of the risk factors involved in perforation, a thorough series and review of the literature has not been performed. We recently reported one such case of colonic perforation following CT colonography, 5 and have since sought to review a wider experience, with a particular view to identifying the risk factors involved.
Methods
A thorough literature review was undertaken, evaluating reports of colonic perforation following CT colonography, with studies of any kind included in this review. Any evidence regarding patient factors or procedural factors that were identified as risk factors for perforation were recorded. An electronic and manual search undertaken included PubMed, Cochrane databases and Ovid-MEDLINE.
A retrospective study was subsequently undertaken, comprising all CT colonographies taking place in the preceding five-year period among the major metropolitan tertiary referral centres throughout the state of Victoria, Australia (population 4 million). The retrospective nature of the study and potential for non-identified cases is acknowledged. The number of cases per institution and specifics of each case of perforation were assessed, with the risk factors identified upon review of the literature to evaluate for the presence of these factors in each case of perforation.
Two main outcome measures were thus assessed: firstly, an evaluation of the risk factors for perforation in both the literature and clinical series, and secondly a comparison between each institution in the clinical series to evaluate the effect of institutional experience with CT colonography on the incidence of perforation. Statistical significance was calculated with the one-way analysis of variance test, with statistical significance considered at P < 0.05.
Results
Reported risk factors for colonic perforation following computed tomographic (CT) colonography
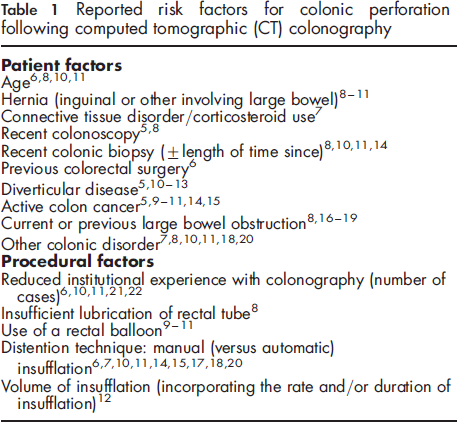
In terms of factors related to the CT colonoscopy itself, several procedural factors have been shown to be contributors to perforation, the most important of which has been shown to be institutional experience with the procedure.6,10,11,21,22 The procedure itself requires cannulation of the rectum; however, insufficient lubrication of the rectal tube, 8 or the use of a rectal balloon, 9 11 put the patient at higher risk. The insufflation technique is also important. The use of manual insufflation (rather than with an automatic insufflator) can increase colonic distension, with its associated increased risk of perforation,6,7,10,11,14,15,17,18,20 and similarly an increased total volume of gas insufflated can potentiate perforation, whether this is due to too high an insufflation rate (higher than 2 L/minute) or for too long a period of time. 12
Institutional experience with computed tomographic (CT) colonography among 10 metropolitan tertiary referral centres, and their incidence of perforation associated with the procedure
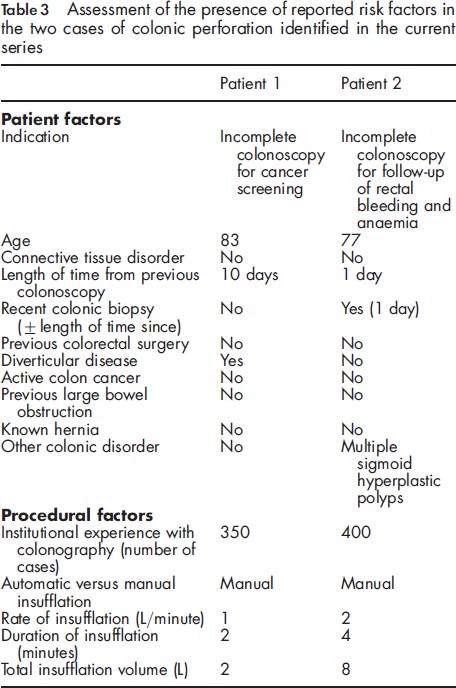
Each case of perforation was specifically assessed utilizing the risk factors identified during the review of the literature (see Table 3), with a range of risk factors evident and some notably absent. Both patients were elderly and had undergone recent colonoscopy. Notably, one patient had diverticular disease, and one had recent colonic biopsy, both potentially contributing to a weakening of the colonic wall. Procedurally, both cases involved manual insufflation, but while one case had a very low insufflation volume (2 L), one had a very high volume (8 L). Both cases presented with only moderate abdominal pain, were diagnosed with CT imaging, and both resolved with conservative management, comprising bowel rest, antibiotics, frequent clinical review and a short inpatient stay.
Assessment of the presence of reported risk factors in the two cases of colonic perforation identified in the current series
Discussion
CT colonography has been widely reported as a safe procedure with low reported rates of complications; however, it has become clear that there is a small but definite incidence of colonic perforation. As the procedure itself is relatively new and there have not been vast numbers of reported cases, estimations of the frequency of this complication are difficult to make and have not been widely reported. However, in several series this rate has been reported at between 0.05% and 0.1%, which is similar to that reported with conventional colonoscopy.4,6,10,23,24 As many patients progress to CT colonography after failed colonoscopy, this comparison may be somewhat biased; however, the current series supports the rates reported in the literature, with a similar perforation rate of 0.06%.
The combined literature review and clinical series highlighted several key causative factors for colonic perforation post CT colonography. Patient factors were shown to be pertinent, and may help to select patients who are either not suitable for the procedure or may require optimization of co-morbidities or modification of the procedure itself. Such factors include age, diverticular disease and recent colonoscopy, especially in the setting of recent biopsy. In terms of the procedure itself, manual insufflation may be suboptimal, but this may well be confounded by the need to closely monitor insufflation pressures. Low volume insufflation is an important factor, as shown in both the literature review and case series, and close monitoring of such pressures is essential. As such, techniques to minimize barotrauma are recommended, such as the use of an automated insufflation device, which monitors rectal pressure and automatically ceases insufflation if pressures exceed a nominated pressure, often 25 mmHg, or if nominated volumes are reached.
In our series, accurate diagnosis of colonic perforation was made with the combination of symptomatic abdominal pain and CT findings of pneumoperitoneum. Rapid diagnosis was able to potentiate surgical review and the instigation of management with antibiotics, bowel rest and admission to hospital. Given the rapid response to conservative management, it is also likely that any intra-abdominal leakage of contrast is minimal, compared with the severe peritonitis that occurs secondary to leakage of barium or other contrast agents. Notably, the onset of abdominal pain in both of our reported cases was rapid and of substantial intensity, which is an important finding given that there has been the suggestion in the literature that asymptomatic pneumoperitoneum following CT colonography may be a common and benign event. 25
Conclusion
The current study, although limited by retrospective study design, has highlighted that there is a small but real risk of perforation following CT colonography, and while it has been widely claimed that virtual colonoscopy is safer than conventional colonoscopy, we suggest that colonic barotrauma and risk of perforation may be more comparable with both techniques than previously suggested. Patient selection, preventative measures and the importance of adequate consent are thus emphasized.