
Abstract
Introduction
Mortality from colorectal cancer has been shown to decrease by repeated screening using faecal occult blood (FOB) testing in randomized screening trials. This report presents coverage and performance of organized screening among the general population in Finland.
Methods
In 2004-2007, people aged 60-69 years were randomized into biennial screening and control arms. The screening test was a guaiac-based FOB test (Hemoccult®) with dietary restriction and three test cards for six consecutive samples. Test positives were referred for full colonoscopy. The programme was launched in 2004 and subsequently it expanded over regions and age-cohorts.
Results
In 2007, the programme covered one-third of the target population and 74,592 people had been invited for screening, of them 26,866 for the second round. Uptakes for the first and second rounds, respectively, were 62% and 68% in men and 77% and 80% in women. The proportion of test positives increased from 2.4% to 2.9% from the first to the second round and the positive predictive value for cancers decreased from 7.5% to 4.3%.
Conclusions
By 2007, organized colorectal cancer screening covered one-third of the target population in Finland. Implementation of screening measured with response rate was successful and met the criteria for a public health programme, but performance in terms of positive predictive value needs monitoring.
Introduction
Several randomized screening trials have demonstrated a reduction in colorectal cancer mortality by repeated faecal occult blood (FOB) testing followed by colonoscopy for test positives. 2 5 All studies used a three-day guaiac-based FOB test as the primary screening test and the magnitude of the reduction was about 16% when the four trial results were combined. 6 The follow-up time in these trials varied from 11 years 3 to 18 years. 7 Screening with sigmoidoscopy once in a lifetime has also been studied in randomized trials. 8 11 The Norwegian study found no significant reduction in colorectal cancer mortality 9 but the UK study found a significant 31% reduction in colorectal cancer mortality in the screening group compared with the control group over a median follow-up of 11 years. Thus, there is currently evidence for reduction in mortality from colorectal cancer with repeated FOB testing and once in a lifetime flexible sigmoidoscopy.
In Finland, an organized colorectal cancer screening programme as a public health policy was started in 2004. The health services are the responsibility of local municipalities. Therefore, joining in the programme was decided at the level of individual municipalities. The screening programme was implemented using individual level randomization into screening and control groups and a gradually expanding invitation scheme over the final target age group of 60-69 years. 12 The screening started in those aged 60-64 years and by 2007 it was extended over the age group of 60-67 years. Invitations were repeated in the screening group every second year. The control group has not been offered screening during the follow-up period and is planned to be screened only after the implementation phase is completed.
The aim of this report is to present coverage and performance of the organized screening programme in Finland run as a public health policy in the first four years since launch.
Methods
The screening programme was launched in September 2004 in 22 municipalities out of 444. By 2007, the programme expanded to include 175 municipalities out of 431 in total (the number of municipalities was decreasing due to merging of small municipalities), and it will expand further both in the number of municipalities involved and in the age-cohorts offered screening. Final evaluation for effectiveness will be based on the comparison of colorectal cancer mortality among the group invited for screening with the control group. Meanwhile, the programme will be monitored with various process indicators like uptake of screening (number screened/number invited), proportion of test positives (number of test positives/number screened), and referrals to and findings of colonoscopy in test positives.
Identification of individuals in the age group of 60-67 years in participating municipalities, as well as the invitation procedure, were centralized. The Population Register Center (PRC) keeps records including a unique personal identifier and address for every resident in Finland. This identifier can be used to link individuals with various health registers, e.g. the Finnish Cancer Registry and the Statistics Finland for causes of death. Individuals in the target population of the participating municipalities were randomly allocated into two equal groups by municipality, gender and year of birth. One group was subjected to an invitation for screening while the other remained a control group and was not contacted.
One national screening centre was established in the city of Tampere at the local Cancer Society to run the programme. The faecal test-kits (Hemoccult®) with advice on how to take the sample and information on consent were mailed to the screenees. They sent the test-kits back to the screening centre by regular mail. Dietary restrictions three days before and during sampling included avoiding raw meat, liver or blood dishes and large amounts of supplemental vitamin C (>250 mg/day). If there was any indication of blood (change of colour to blue) in any of the three test cards the sample was classified as a test positive and a notification letter was sent to the municipal contact for referral for full colonoscopy, as well as to the person in question. Thereafter, diagnostics, treatment and follow-up of the screen positives followed current national guidelines (normal care) and were no longer directly a responsibility of the screening programme. However, the screening programme took care of active surveillance in terms of collecting data on all individuals referred for colonoscopy and compiling the findings of diagnostics and treatment.
Individuals with inadequate test cards (e.g. too old a sample, wrong side of the card used) were sent a new set of test cards. New cards were sent maximally twice per individual and screening round. If the cards were still inadequate the person was classified as a non-responder and asked to contact the regional health provider in case symptoms of colorectal cancer were present.
Data on colonoscopy findings, cancers and adenomas were obtained by collecting detailed colonoscopy charts, information on surgery and data on pathological findings of removed lesions and surgical material. All colorectal cancers and adenomas were based on histological classification. Colorectal cancers were carcinomas of the colon and rectum as well as adenocarcinomas of the anal canal. The neoplastic polyps were classified as tubular, tubolovillous or villous adenomas. The size of adenomas was primarily obtained from the colonoscopy report (the biggest one taken) and in some cases data from the pathology report were used.
Results
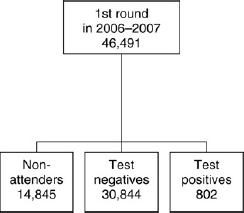
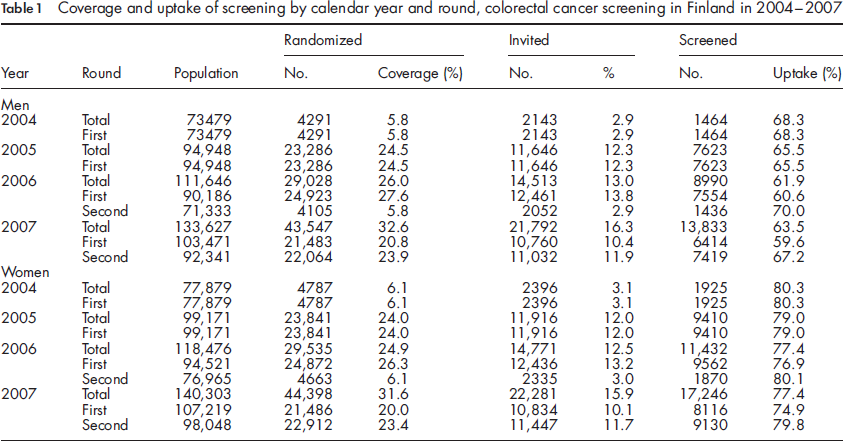
In 2007, close to 500,000 people (243,717 men and 258,061 women) belonged to the target age groups of screening (born between the years 1940 and 1947) and about 32% of the target population was covered by the screening programme (Table 1). At the end of 2007 about 16% of the individuals in the entire target population were invited for screening. All individuals who were invited for the first screening round in 2004 and 2005 and were still alive and residents of municipalities taking part in the programme (n = 26,866, 95.6%) were invited for the second screening round two calendar years later (Figure 1). Thus, the invited population was two years older at the second screening round compared with the age at the first round. The second round invitations were sent to all 26,866 individuals eligible for the second round whether or not they had responded to the first round invitation, and to test negatives and test positives alike. Those invited for their first screening round in 2006 or 2007 were not invited for the second round by the end of 2007, the closing date of this study (Figure 2). The number of annual invitations increased between the years 2004 and 2007 from 2143 to 21,792 in men and from 2396 to 22,281 in women, respectively.
Invitation procedure for the first and second rounds of screening in municipalities where colorectal cancer screening started in 2004 or in 2005 in Finland Invitation procedure for the first round of colorectal cancer screening in municipalities where screening started in 2006 or in 2007 in Finland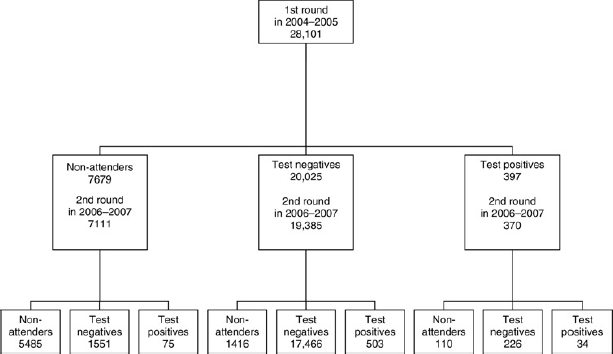
Coverage and uptake of screening by calendar year and round, colorectal cancer screening in Finland in 2004-2007
The screening test detected blood in 1811 faecal samples of 1777 individuals who were subsequently referred for full colonoscopy by their local healthcare providers. Of them, 34 individuals had a positive finding twice, both at the first and at the second screening round. Colonoscopy was done in 90% of those referred, i.e. of all test positives. The most common reason for no colonoscopy after a positive test result was a recently performed colonoscopy elsewhere.
Number of those screened, test positives, detection proportions/1000 (DP) and positive predictive values (PPV) for confirmed cancers and adenomas by age and screening round in the colorectal cancer screening programme in Finland in 2004-2007
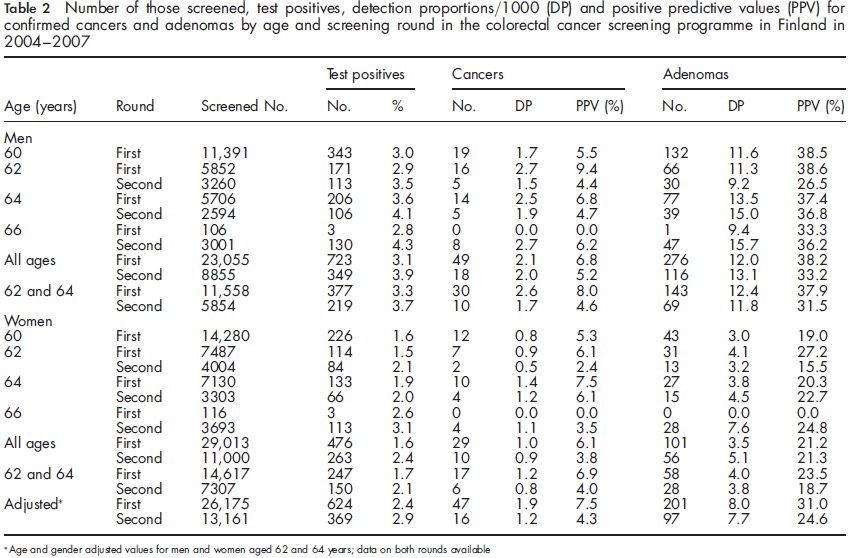
Age and gender adjusted values for men and women aged 62 and 64 years; data on both rounds available
Among the test positives, 106 colorectal cancers (67 in men and 39 in women) were diagnosed and 549 individuals with at least one adenoma (392 men and 157 women). The detection proportion of cancer (number of cancers found per 1000 participants) was the same at both screening rounds and higher in men (2.1 and 2.0 at the first and second rounds, respectively) than in women (1.0 and 0.9 at the first and second rounds, respectively) (Table 2). However, crude proportions for the first and second rounds were 2.6 and 1.7 for men and 1.2 and 0.8 for women, respectively, when only those aged 62 or 64 were included. Additionally, proportions adjusted for age and gender in those aged 62 and 64 years were 1.9 at the first round and 1.2 at the second round, indicating a decreased detection proportion of cancers at the second round. The positive predictive value for cancer (PPV, calculated as the number of cancers found per number of 100 test positives) decreased from 7.5% at the first round to 4.3% at the second round when proportions were adjusted for age and gender (Table 2).
We observed a nearly three-fold detection proportion of adenomas in men compared with women both at the first and the second screening rounds (Table 2). The detection proportions were similar for the first and second rounds, 8.0/1000 and 7.7/1000, respectively, after adjustment for age and gender. In men, the PPV for adenomas was higher at the first round (38.2%) than at the second round (33.2%), whereas in women there was no difference between the rounds (21.2% versus 21.3%). After adjustment for age and gender, the respective PPVs were 31.0% at the first round and 24.6% at the second round.
Numbers and detection proportions per 1000 (DP) of adenomas at the first screening round (n = 377) and second round (n = 172) by size, grade of dysplasia and morphology; colorectal cancer screening programme in Finland in 2004-2007
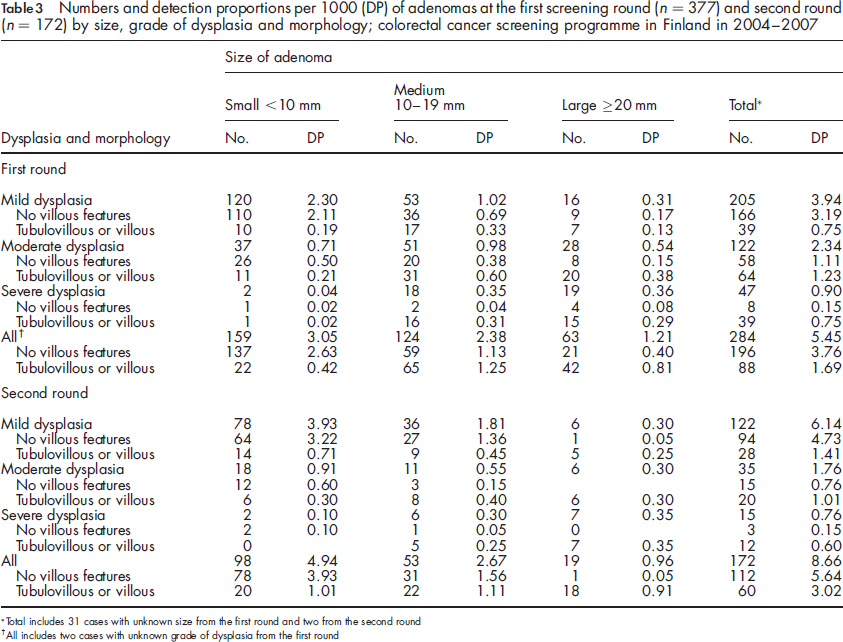
Total includes 31 cases with unknown size from the first round and two from the second round
All includes two cases with unknown grade of dysplasia from the first round
Discussion
So far, only FOB testing 6 and sigmoidoscopy screening has been studied in randomized trials with results available on mortality reduction.9, 13 The evidence for a reduction in mortality with FOBT comes from several randomized screening trials2,3,5,7 and from a large-scale feasibility study in the UK 14 16 while the evidence for reduction in mortality with sigmoidoscopy screening was recently published. 11 Routine colorectal cancer screening using FOBT has been discussed or planned in many countries and was recommended by the European Council in December 2003.17,18
Any new service screening programme should be introduced in a controlled way to ensure unbiased evidence on effectiveness. In Finland, this was done earlier when breast cancer screening was implemented in 1987 as a public health policy using cluster randomization by age-cohorts. 19 Non-randomized studies, such as time trend analyses and regional comparisons, cannot distinguish between the effects of screening and other factors, e.g. improved treatment. Thus, the evaluation has to be built in with proper design of the implementation phase. For example, the expected effect of screening with FOBT is less than a 20% reduction in mortality from colorectal cancer in those who have been offered screening compared with those who have not been offered screening. 6 This kind of small difference cannot be detected in non-randomized studies or in routine statistics. Originally our programme was planned to have a six-year implementation phase with randomization, and it was estimated to accumulate a sufficient number of colorectal cancer deaths in 10 years for an expected mortality effect of 20% (with 90% power) if the programme coverage had reached 50% of the target population. 12 In 2009, the randomization phase was extended by five more years because it seems possible to achieve the expected power in 2015 if the coverage stays at the 30% level reached by 2007.
In different regions of Finland, there were substantial differences in the availability of colonoscopy services. One main concern in the early implementation process was the anticipated shortage of colonoscopy resources. This however has not been a problem in the municipalities taking part in screening. A step-wise start with a steadily increasing proportion of the target population offered screening allowed municipalities to meet the needs for diagnostic resources. On the other hand, the participating municipalities may have initiated the programme due to good colonoscopy resources possibly causing selection of regions ready to launch. However, since the mortality evaluation will be based on random allocation of the population within a municipality, the estimation of effectiveness will be valid.
Participation proportions at the first screening round have been reported to vary from 53% to 67% in the randomized FOBT-based screening trials on colorectal cancer. 6 As a rule, routine application results in lower uptake than that achieved in trial conditions. Participation in Finland was very high already at the first round (62% in men and 77% in women), and the second round showed improved participation proportions in both genders. This was partly because the invited population at the second round was two years older than at the first round. In women, the participation proportion for breast cancer screening is high in Finland, about 85% of those invited are actually screened. 1 In men, however, the expected uptake was unknown, only a small regional pilot was available from 1980 where the response proportion reached 69% overall. 20 We have also previously reported marital status to be an important factor in increasing uptake especially in men; among married men the participation proportion was close to 70%. 21 In Scotland, results on participation proportions have been reported from the first three rounds of a demonstration pilot and they were close to 55%. 16 In any case, monitoring of participation and its determinants with proper actions is crucial for the success of any routine screening programme.
In general, test positivity proportions and detection proportions are found to be high at the prevalence screen of the first round. This was not observed in our programme for adenomas but was true for detection proportions of cancer. The low sensitivity of the FOB test in general and in Finland, 22 approximately 50%, may account for some of the high number of test positives at the second round. It is also unlikely that new adenomas originating between the rounds would explain the high positivity proportion at the second screen. Rather, the results imply poor sensitivity of the FOB test in detecting adenomas as most of them do not bleed. In addition, an improved sensitivity of the laboratory after the first learning period cannot be ruled out.
The observation of a decrease in the PPV of cancers from the first to the second round with the simultaneous higher positivity proportion causes concern about the programme performance. The PPV was higher in the younger age groups and was reduced by age at the first round. At the second round, however, the opposite was observed. The question of increasing the screening interval may become relevant in the future to allow for a higher PPV for accumulating the number of bleeding cancers after the entry screen. Other potential changes to the programme include the modification of the faecal test to, for example, an immunochemical test option and the possibile consideration of flexible sigmoidoscopy as the primary test. These modifications can be considered after the current implementation phase, thus not before the year 2015.
The implementation of colorectal cancer screening in Finland assessed by coverage of the guaiac-based FOB test has been successful. The performance as to testing procedures and referrals for colonoscopy has been adequate but the decreasing PPV for cancers causes concern, and should be monitored carefully in the near future. The programme meets the criteria both for a randomized trial and for a public health programme producing unbiased data from the implementation period, and ultimately allowing an unbiased evaluation of its effectiveness in terms of mortality.