
Abstract
Objective
To investigate an association between seasonal changes in temperature and the prevalence of congenital hypothyroidism (CH) in the Southwest of Iran.
Methods
A prospective two-year study conducted from March 2007 to March 2009 during the nationwide screening programme for CH in Ahvaz, the biggest city in southwest Iran. Blood samples were taken from almost all newborns by heel-stick and used in a thyroid-stimulating hormone (TSH)-enzyme-linked immunosorbent assay (ELISA). Serum thyroxine (T4) and TSH were measured if the ELISA-TSH was >5 mlU/L (suspicious cases). Infants were considered to have CH with T4 <6.0μg/dL and TSH > 10 mlU/L, or with normal T4 values and persistent high TSH values for >2 months (subclinical hypothyroidism). Date of birth and sex were recorded. Detailed temperature data were obtained from the meteorological organization. The relationship between the monthly incidence of CH and the average monthly temperature was investigated.
Results
From 47,075 (50.92% male) newborns, 1131 were referred (recall rate = 2.4%) and 142 infants (51.4% male) were confirmed to have CH. The seasonal distribution of CH cases was 32.4% in the warm period and 67.6% in the cold period of the year (19%, 13.4%, 32.4% and 35.2% in spring, summer, fall and winter, respectively; P = 0.001). A statistical difference was seen between mid-summer (2.8%, warmest time) and early winter (15.5%, coldest time). The above-mentioned difference was the same for suspicious individuals (P < 0.001). The odds of being affected were increased by 4% for each fall of 1°C.
Conclusion
The prealence of CH has a significant negative correlation with the temperature in the tropical area of Iran.
Introduction
Patients and Methods
Patients
During the scheduled nationwide screening programme for CH, this two-year prospective study was performed from March 2006 to March 2008 (two full solar years) in Ahvaz, the biggest city in the southwest of Iran. Every month of the solar calendar starts on the 21st day of the previous Christian month; thus, our fifth month would be from 21 July to 20 August. We considered the number of screened infants instead of the number of live births because nobody could get an identification card without being screened. All analyses were carried out with the mean of the data.
Methods
We collected heel-stick blood samples and took dry spots on standard filter paper between the third and fifth day of life to assess TSH levels by enzyme-linked immunosorbent assay (ELISA) using an ELISA reader (Stat Fax-2100; Awareness Technology Inc, Palm City, FL, USA). The measurements were conducted in the Newborn Screening Laboratory of Ahvaz Department of Health. The staff, laboratory technicians and the settings for screening and confirmatory tests remained unchanged during the study. Screened patients were referred for a confirmatory test if the TSH level was >5mlU/L; these subjects were classified as the suspicious group. For this group, blood samples were taken by venepuncture in the second to third week. Evaluation of the thyroid function test (TFT), including thyroxine (T4), TSH and triiodothyronine resin uptake was performed using an ELISA kit (Monobind Inc, Lack Forest, CA, USA) and an ELISA reader (ELx800, Bio-Tek Instruments Inc, Winooski, VT, USA). Newborns who were reported to have T4 <6.0 μg/dL and TSH >10 mlU/L, or a normal T4 level and persistent high TSH >6.0 mlU/L (subclinical hypothyroidism) beyond the 60th day were assigned to the CH patient group. Data regarding sex, laboratory results and birth date (month and year of birth) were recorded for all screened newborns, suspicious and CH subjects. Data concerning the average monthly temperature (AMT) and absolute minimum and absolute maximum temperatures of each month were obtained from the meteorological station in the Khuzestan province, a branch of the Iran Meteorological Organization (http://www.irimo.ir/english/statistics/index.asp).
Statistical analysis
The χ 2 test was used to assess the association between variables. P values < 0.05 were regarded as statistically significant. We used logistic regression to analyse the occurrence of a case of CH compared with the mean temperature at birth.
Results
Seasonal distribution for all live births, suspicious infants and confirmed CH cases
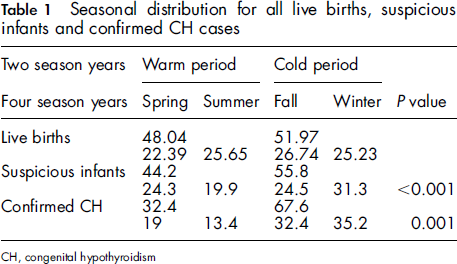
The suspicious and CH groups both had their nadirs in summer with 19.9% and 13.4%, and their highest frequencies in winter with 31.3% and 35.2%, respectively. The traditional warmest (July/August) and coldest (January/February) months were the exact time of nadir (2.8%) and peak (15.5%) for occurrence of CH. Meteorological data revealed the fifth month (July/August) as the warmest month at 28.3-50°C (AMT = 38.9°C), which correlated with the lowest incidence of CH. The tenth month (January/February) was the coldest month at -0.2 to 23.9°C (AMT = 11.15°C), which correlated with the highest incidence of CH. Both sexes had their nadir in July/August and their peak in January/February. Figure 1 reveals a linear relationship between the occurrence of CH and the average temperature at the time of birth (Spearman's rho correlation method, r = 0.87; P < 0.001).
Linear relationship of occurrence of congenital hypothyroidism and average temperature (°C) at the time of birth (Spearman's correlation method; r = -0.87; P < 0.001)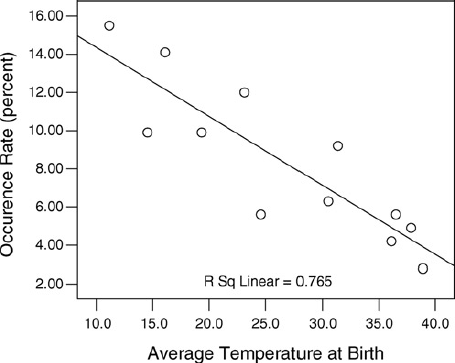
We performed a logistic regression of the occurrence of a case compared with the mean temperature at the time of birth. For each 1°C increase in temperature at the time of birth, infants were 4% less likely to be a case of CH (odds ratio 0.96, 95% confidence interval 0.94-0.98; P < 0.001). Separate regressions were also performed for males and females, but no associations were found accordng to sex (males: odds ratio 0.95, 95% confidence interval 0.93-0.98, P < 0.001; females: odds ratio 0.96, 95% confidence interval 0.94-0.99, P < 0.01). Figure 2 shows the different distribution of CH cases in two warm and cold periods of the year (P = 0.001) while no difference was found by sex (P = 0.55).
Distribution of male and female infants with congenital hypothyroidism in two warm (spring and summer) and cold (fall and winter) periods of the year (for all patients: χ
2
= 35.9, P = 0.001)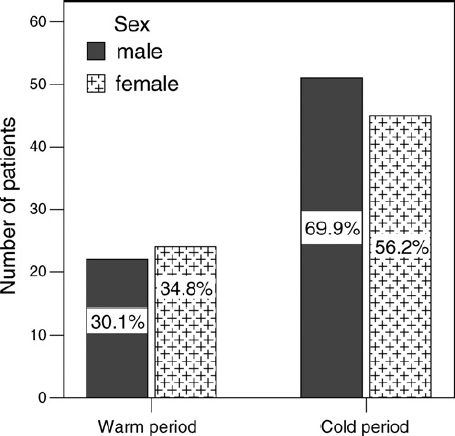
Discussion
The aetiology of CH is well known. It can be caused by genetic factors, e.g. dysgenesis or dyshormonogenesis, and by nutritional and environmental factors, e.g. iodine deficiency, maternal autoantibodies and anti-thyroids. The numbers of referred and CH cases were not equal in the different seasons. We hypothesized that the occurrence of CH is related to seasonal variations, which is supported by some reports. Several studies have reported a high prevalence of CH in Iran (nearly 3/1000).6,9 This finding has been explained by our particular gene pool dictating dysgenesis or dyshormonogenesis, high rate of consanguineous marriage and mild-to-moderate iodine deficiency. 10
Waller et al. 5 and Henry et al. 11 disproved an association between the time of birth and the incidence of CH, but many others have reported an association in different ways. Hashemipour et al. 7 reported a seasonal difference in the occurrence of CH in Isfahan (the centre of Iran); however, it was not statistically significant. Interestingly, they reported that CH was more common in summer than in winter. We were surprised that it was the opposite in our first review. Our area is different from other parts of Iran (e.g. Isfahan has 4 seasons); our region experiences only two seasons - warm and cold. We have tropical weather and the temperature varies from >50°C in August to <0°C in February. This large difference would help us identify possible factors that change with or due to temperature. The solar year starts on 20 March, coinciding with the beginning of spring and the warm season. The recorded data of the meteorology station of our province confirmed that the temperature rises slowly until the fifth month (July/August) and then decreases gradually until the coldest month (January/February).
Our study showed that there was no significant difference in the number of live births during the year. The screening revealed a clear trend of more abnormal TFT results in the cold season of the year in both suspicious and CH cases. The gradual and continuous increase in the number of infants with CH from July to February shows that it was not an accidental finding.
The linear relationship between the occurrence of CH and temperature (Figure 1) denoted that the risk of delivering an infant with CH (no difference by sex) was significantly higher during the cold season and lower during the warm season. This finding is contrary to that obtained by Hashemipour et al. 7 whose study showed a higher prevalence of CH during the warmer months.
Several studies have found mild-to-moderate seasonal variations similar to our result. 12 16 Japanese, British and Finish researchers suggest that the cold season is a high risk factor for the occurrence of CH.12,15,16 Miyai et al. 2 proposed a relationship between the number of newborns with CH and intrauterine viral infection. Hall et al. 15 also has shown a higher frequency of CH (but much less than in our study) in Pakistani immigrants living in England; they suggested that this was due to the system of consanguineous marriage.
Previous studies have not provided any explanation for this variation and have only presented it as a descriptive finding. Our policy was exclusion of all transient cases by follow-up; only two cases with TSH >50 mlU/L after the 20th day and two other cases with TSH between 10 and 50 mlU/L progressed to the euthyroid stage before 12 months of age. This strategy ensured that the CH cases under consideration would include those due to dysgenesis and dyshormonogenesis in the majority of patients. This hypothesis was confirmed by scintiscanning, which was performed for many CH cases that passed the critical period of brain development (1.5-2 years of life). Regarding the aetiology, we did not find any specific pattern for time-related occurrence. Theoretically, permanent cases should be due to inheritance, which is not affected by changes in the temperature. However, the effect of seasonal epidemics of particular viral infections, regular seasonal agricultural food products and possible influences of temperature changes (due to exposure to different environmental factors) on the gene expression pattern or on a particular human leukocyte antigen background should be considered as the causes of this trend. We were unable to explain the significant association between the incidence of CH and changes in the temperature in this area. The measurement of urinary iodine in newborns and pregnant women in such areas during different times of the year may solve the problem.
The limitation of this study was that maternal data were not studied. Furthermore, we did not look for specific causes of CH (for example, maternal autoantibodies, thyroid ultrasonography).
Footnotes
Acknowledgment
We thank staff at the Department of Health in Ahvaz for their cooperation during screening, and the meteorological centre of Khuzestan, a branch of the Iran Meteorological Organization, for providing their valuable data.