
Abstract
Objective
The UK Newborn Screening Programme has standards to facilitate the early identification and treatment of five specific diseases to prevent lifelong impairment or death. This audit aimed to assess the newborn bloodspot screening programme in an inner London borough and to make recommendations for service improvement.
Methods
Data on babies registered with a general practitioner in the borough between April 2008 and March 2009 were obtained from the borough's health database and the laboratory result systems and compared with national screening standards. Interviews were conducted with the leads of each service providing components of newborn screening.
Results
A total of 292 (8%) out of 3636 babies registered within the audit period had no result on the database (average 1 in 13). Regional reports revealed that over the previous three years the borough, like many others, had consistently failed to achieve the core standards for newborn bloodspot screening. Major areas of concern identified by this audit pertained to the quality of the bloodspot sample, response to requests for repeat samples, timely identification of untested babies and communication of results to parents.
Conclusion
The audit revealed that for the majority of children registered in the borough, screening was successfully carried out. However, gaps in the service meant that with current practice one affected child could be missed every seven years. Recommendations include staff training, frequent data reviews, and providing a coordinating officer to oversee the programme and follow up missing results.
Introduction
The National Newborn Screening Programme is one of the largest screening programmes in the UK with approximately 750,000 newborns screened each year. It originated in the late 1950s with locally organized screening programmes for phenylketonuria (PKU) using ferric chloride solutions to test babies’ urine for phenylpyruvic acid, a characteristic metabolite of the disorder. 4 With the advent of the Guthrie Card in 1969, the Department of Health recommended changing to a blood-based screen for PKU by the early 1970s. The use of this more sensitive and specific approach, the development of radioimmunoassay and subsequently tandem mass spectrometry, made screening for a further range of disorders possible. 5
The UK National Screening Committee (NSC) 6 has recommended that all babies in the UK are offered screening for PKU, congenital hypothyroidism (CHT), sickle cell disease (SCD), cystic fibrosis (CF) and more recently medium-chain acyl-CoA dehydrogenase deficiency (MCADD). 5 7
PKU affects approximately one in 10,000 babies in the UK and about 80 affected babies are born each year. There is a congenital absence or deficiency of the enzyme phenylalanine hydroxylase which converts the dietary amino acid phenylalanine to tyrosine. The build-up of phenylalanine leads to the formation of neurotoxic levels of its byproducts and subsequent development of irreversible learning disability if left untreated beyond 21 days of age.8,9
Congenital hypothyroidism affects one in 4000 babies in the UK, an average of 185 births each year. There is a lack of thyroid hormones at birth. Early detection and treatment by 21 days of birth with thyroid hormone replacement is vital to prevent profound learning disability.10,11
Sickle cell disease affects one in 2000 babies in the UK. Abnormal haemoglobin is produced, which becomes sickle shaped under certain conditions, predisposing to pain, tissue damage, infection and even death. Early treatment by two months of age through immunizations, antibiotics and parent education is advised.12,13
Cystic fibrosis affects one in 2500 babies in the UK, about 300 births each year. Affected babies produce thicker mucus and secretions, largely affecting the respiratory and digestive systems, leading to failure to thrive. Nutritional benefit of early intervention was demonstrated in a large randomized trial involving over 650,000 newborn infants. 14 However a suggestion of possible selection bias has been raised to question the validity of the study's conclusion. 15 There remains a lack of evidence to support early intervention in cystic fibrosis, particularly regarding the main clinical outcome, respiratory failure. Much of the current guidance for management of these infants is based on expert consensus. 16
Medium chain acyl-CoA dehydrogenase (MCADD) deficiency affects one in 10,000 to 20,000 babies born in the UK. There is an inability to break down fat easily to make energy for the body. Serious life-threatening metabolic crisis with 25% mortality can be avoided with early detection and treatment.17,18
Although these conditions have devastating clinical manifestations, there is evidence that their effects may be preventable with early intervention. 9 15 Screening offers this early disease detection system. To be successful, however, the screening service must have adequate coverage, an effective system for following up on missing results and clear standards to guide practice.
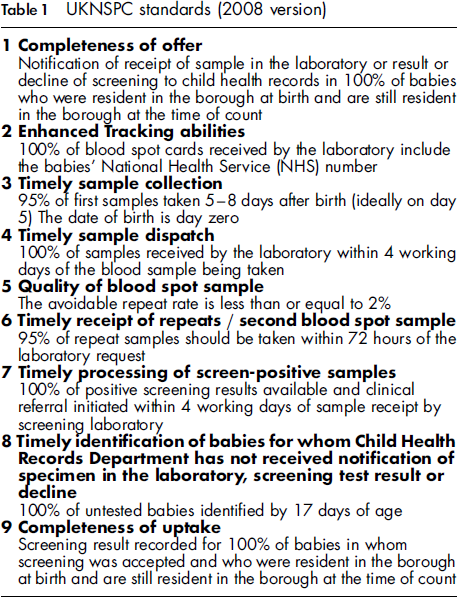
UKNSPC standards (2008 version)
The newborn bloodspot screening programme is a three-stage process, as illustrated in Figure 1. Each stage encompasses a defined set of roles, delegated to specific professional teams. The efficient implementation of the screening programme relies heavily on the diligence and skill of these respective teams.
A three-stage process of newborn screening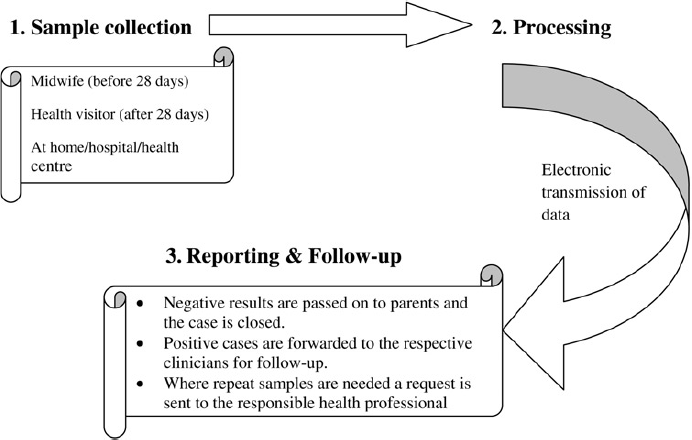
Regional reports highlight that standards are not being met nationally. This audit examined neonatal bloodspot screening in one borough and aimed to make recommendations on how to improve the service. This borough has higher than average levels of sickle cell carriers and cases, as well as a highly mobile, diverse, and deprived population.
Methods
Data on babies registered with a general practitioner (GP) in an inner London borough between April 2008 and March 2009 were obtained from both the borough child health database and the laboratory result systems in April 2009. The results obtained were compared with the national standards to determine performance. The borough in this study is a defined area (population approximately 300,000) that has one NHS coordinating body (primary care trust) for all the newborn services in this area. Data providing a comparative analysis of the performances of each hospital in this London region against national standards over the previous three years (2005-2008) and the first quarter of 2008-2009 were also reviewed.
Face-to-face interviews with individual stakeholders in each stage shown in Figure 1 were conducted. Four key stakeholders were interviewed: the leads of midwifery, screening laboratory, database team (Child Health Records) and health visitors. Consultations were also held with staff members directly involved in the respective screening tasks. Various issues were highlighted as potential precipitants of gaps in respective roles and ideas on how to address these were discussed. Meetings were also held with commissioners (who allocate the contracts and budgets for health services) to facilitate implementation of recommendations necessary for service improvement.
A re-examination of the database in July 2009 was conducted to identify any late results that were not available in April 2009.
Results
Newborn screening data in the borough for 2008/2009
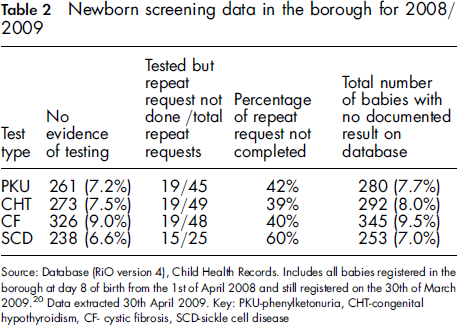
Analysis of data from the four screening tests shows that approximately 292 (8%) out of 3636 babies registered in the borough between April 2008 and March 2009 inclusive had no result recorded on the central data collection system. This implies that in the year to March 2009, one in 13 babies registered in the borough may not have benefited from the screening programme. There was no evidence that testing was carried out in about 275 (7.6%) newborns and the numbers without screening results increased further due to a large number of requests for repeats not being completed. The database did not clearly indicate whether results had been communicated to the parents of the child.
Further analysis of the records of babies with no results in April 2009 (Table 2) conducted in July 2009 revealed that some of the results reported as missing were now available, partly due to delays in data upload and late returns of repeat requests. The final percentage without results is therefore less than the national data illustrate (Table 2) but the opportunity for early intervention may have been missed if any had been disease cases.
Performance against national standards
Data providing a comparative analysis of the performances of hospitals in this region against national standards were recently made available.
20
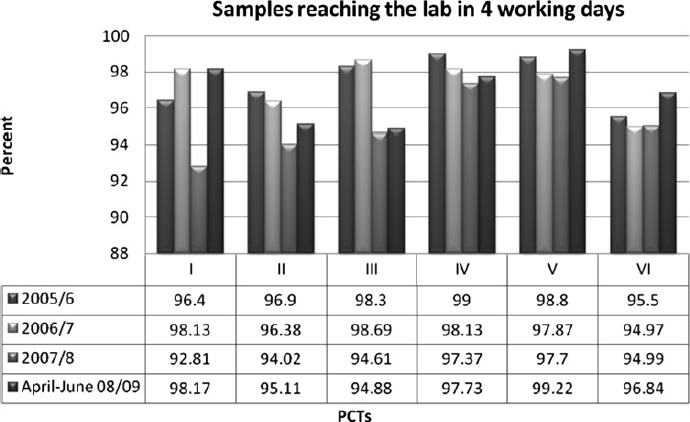
Data based on performances against UKNSPC 2008 standards 2 and 4 over the last three years (2005-2008) and the first quarter of 2008-2009 are illustrated in Figures 2 and 3 respectively.
18
The hospitals in this borough are designated roman numerals I and II, while those of the neighbouring boroughs are III-VI.
Region performance against standard 2 for April 2005-June 2009. Key: Standard 2 is 100% of bloodspot cards received by the laboratory including the babies’ NHS number Regional hospitals performance against standard 4 for April 2005-June 2009. Key: Standard 4 is 100% of samples received by the laboratory within four working days of the blood sample being taken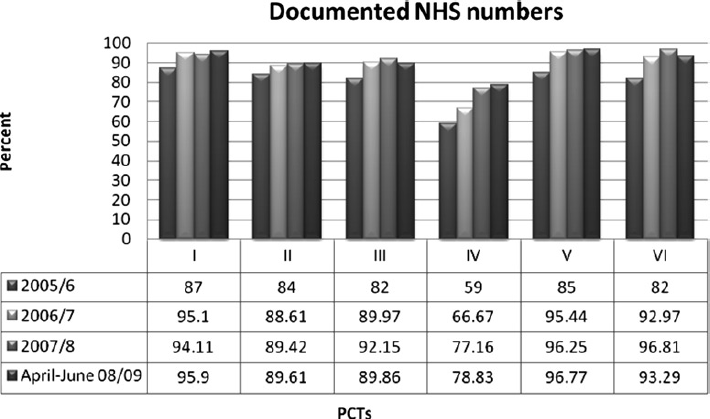
No hospital in this region was achieving the standard set: possible confounding factors put forward include discharges from areas where the NHS number (unique patient identifier) was not part of the discharge summary, or births transferred from private maternity units.
None of the hospitals in the region was achieving standard 4 despite the provision of pre-paid pre-addressed envelopes.
These findings show the need for implementation of new processes aimed at improving current practice. In order to identify the underlying issues in the service, the key stakeholders responsible for each stage illustrated in Figure 1 were consulted. The outcome of these meetings is described under the respective stage in the pathway.
Sample collection
This stage in the pathway comes under the jurisdiction of the midwife looking after the newborn in question up until the 28th day of birth, after which it becomes the responsibility of the health visitor to whom the baby is assigned.
Six of the UKNSPC standards illustrated in Table 1 come under the role of the midwife.
Midwife's role
Offer all new parents bloodspot screening;
Once consent is granted, obtain a heel-prick sample between 5-8 days after birth, ideally on day 5;
Ensure adequate blood sample is obtained on the bloodspot card;
Ensure that all details of the newborn are clearly written onto the card including NHS number;
Bloodspot card to reach the lab within four working days;
Obtain repeat samples or samples on babies identified to have no result whilst under 28 days of age.
Data presented in Table 2 show that for some children, test results were not available on the database. In addition, data from across this region further illustrated that performance in all the local hospitals fell short of the required UKNSPC standards. 18 Discussions with midwives revealed varied levels of experience and competence with regards to carrying out the heel-prick procedure. The issue of re-emphasizing the importance of NHS numbers being written on every bloodspot card to aid enhanced tracking was highlighted. The forthcoming bar code labels should help to make this less of a problem.
Health visitor's role
Obtain results from the database and inform parents either in person during visits or via the post;
Obtain bloodspot sample in a timely manner when requests for repeats are made after day 28 of birth.
During interviews with the lead health visitor, the key area of concern was around which health visitor dealt with requests for repeats in babies over the age of 28 days. Repeats could be a legitimate request for a second sample or avoidable due to samples being:
Taken whilst the baby was too young (taken on or before day 4);
Taken too soon after transfusion;
Unsuitable specimens (expired card, contaminated, transit time > 14 days);
Insufficient sample.
In addition, there appeared to be no easily identifiable section on the database where evidence that results have been communicated to parents could be entered.
Processing
The screening laboratory is solely responsible for this stage in the pathway. Upon receipt of samples processing takes a maximum of two days, except where positive or inconclusive results are encountered when it might take an extra few days to confirm. Therefore, most results should be sent to the database in the Child Health Records Department (CHRD) within three days of sample receipt.
Laboratory role
Process samples and send a daily spreadsheet of results electronically to the CHRD;
Direct referral of positive results to the respective consultant paediatrician within four working days of sample receipt;
Phone and mail requests for repeat samples to the midwife who obtained the original bloodspot sample;
Alert the responsible public health consultant when three requests for repeat samples for one patient remain unanswered.
The main issues that arose from the interviews with the lead laboratory officer pertained largely to the quality of the samples received. Insufficient blood samples, inappropriately filled bloodspot cards and uncompleted repeat requests were identified as recurring problems.
Reporting and follow-up
This is a vital stage in the screening process because of the importance of good record-keeping, passage of accurate information to parents, and adequate follow-up and care of affected babies. It is, however, also a key stage because it could act as the focal point for the early identification of untested babies.
Child health records department role
Daily input of screening test results into the database;
Prepare weekly report of babies with no test results by day 19;
Contact the laboratory and other boroughs to determine if missing results are with either of them. If not, then refer babies without results by day 19 to the lead health visitor who should arrange repeats.
A cause of delays is that the CHRD is unaware of whether or not a child has been offered screening, has declined screening or has been tested until data come from the laboratory at the earliest time which at present is about day 20. The piloted National Failsafe System (described below) would be accessible to CHRD and should help curb this problem but local measures are needed to deal with issues arising in this borough.
Clinicians’ role
Receive referrals of affected babies by phone or mail or both in most cases;
Nurse specialist, health visitor or both depending on local practices visit the family to break the news and arrange a clinic appointment with the respective consultant paediatrician;
Nurse specialist and health visitor are contacted by the consultant or a member of his/her team to alert them of families that fail to attend clinic;
Health visitor tries to make contact with the family but where this fails reports the case to social services.
Follow-up and care of the affected child in this borough is very robust. There were no reported cases of affected children not being adequately followed-up. The only concern identified pertained to families who, on predominantly religious grounds, went to extreme lengths to avoid follow-up. They relocated without providing a forwarding address and, as in one reported case of SCD, only emerged when the child presented to hospital moribund. Involvement of GPs in the screening process should facilitate early identification of these families. However, better parent information strategies are necessary to encourage proactive participation of families in the screening process. 21
Overall, throughout each stage of screening, gaps were identified and methods to address these are discussed below.
Discussion
This audit revealed that the newborn bloodspot screening programme in this borough screened the majority of infants. However, service reporting or coverage did not seem to be ideal, and delays in the process predisposed to the risk of delays in treatment if a baby were to be positive for a disease. Reasons for the omission of data or delays in the process were suggested during the interviews with the staff involved in newborn screening. Reasons suggested included changes in responsible staff members, the shift to a single sample processing laboratory during the year, and delays in the early identification and reporting of each child without a set midwife. This last point is of particular significance because of the high patient mobility within the borough and inward flow from neighbouring boroughs. The mobility, high levels of diversity and language barriers in this borough mean that the service needs to adapt to account for the population characteristics.
Following data analysis and interviews with the staff involved in newborn screening, the following recommendations were proposed to improve coverage and timeliness of screening.
Recommendations regarding the role of midwifery
During discussions with the lead of midwifery there was an acceptance of the need for a set programme aimed at regularly updating midwives on appropriate techniques and re-emphasizing their roles in newborn screening. Ideally bloodspot training would be mainstreamed into professional standards and training. This could be made a requirement for new or agency employees.
Part of this borough is involved in a national pilot scheme called the Failsafe System. This is a web-based application put forward following a proof of concept exercise involving the NHS Sickle Cell and Thalassaemia Screening Programme, the UK Newborn Screening Programme and Northgate Information Systems. The exercise demonstrated clear benefits to the midwifery department in identifying delayed and missing samples which might otherwise have been overlooked and identified areas for improvement in terms of the software and the supporting systems and processes. 22 Midwives are advised to review the application regularly to identify babies on their caseload who have not been screened; in addition, a clerk at the Failsafe System's headquarters alerts the responsible midwifery team when a bloodspot card has not been received by the laboratory by day 10. Adequate implementation of this scheme would hopefully further improve patient coverage.
Recommendations regarding the role of health visitors
A trained lead community staff nurse or health visitor should be responsible for repeats in their area for babies over 28 days old.
With regards to communicating results to parents, a column has now been added onto the database where health visitors or their staff can tick a box and include their initials to confirm when exactly results were passed on to parents. This is now included in training for health visitors.
Recommendations regarding the database officers’ roles
A database officer designated with the role of overseeing the screening programme is advocated. 23 Their role would include daily identification of babies with no sample in the laboratory by day 10 and no results by day 17, contacting respective midwives (if child is less than 28 days old) or health visitors (if 28 days old or greater) for repeats, contacting neighbouring boroughs to locate families that have moved and reporting screening coverage back to lead midwives and health visitors. This could be employed where the Failsafe pilot is not currently in use, and in addition to Failsafe to help identify new locations of mobile families.
Additional recommendations
Highlighting the newborn screening targets in every baby's red book in order to involve parents in the process. The red book is a parent-held record of all the child's health care recommendations and appointments including screening;
Including GPs in the screening process. This borough has quite a mobile population with families moving in and out of the borough frequently, sometimes just after the birth of a child. GPs could play a very important role in ensuring that no such babies miss out on screening by checking that screening has occurred (using the red book);
Repeat audit in 12 months to evaluate impact of recommendations.
Conclusion
The newborn bloodspot screening service is a crucial part of the national child health programme. The goal of the programme is early identification of babies with a treatable disorder. Without newborn screening, these affected infants may not be diagnosed soon enough to prevent serious health problems, including severe learning disability or death.
Every child should benefit from this service. Whilst the overwhelming majority of babies will be free of these diseases, for the small number of affected babies, early diagnosis and treatment could reduce lifelong impairment.
This audit indicates that while extensive coverage is presently being accomplished by the screening team in this borough, with several affected babies being identified early and provided with vital intervention, there is the risk of up to one affected child missing screening every seven years. Therefore, improved coordination and tracking should be implemented to ensure coverage and timely screening.
Footnotes
Acknowledgment
The authors acknowledge the assistance of the Public Health Directorate and Commissioning of NHS Lambeth and NHS Southwark, Lambeth Community Health teams, hospital midwives, and the newborn screening programme and laboratory, with particular thanks to Dr Abdu Mohiddin, Consultant in Public Health at NHS Lambeth.