
Abstract
Objectives
To assess the effect of gender, age and deprivation on key performance indicators in a colorectal cancer screening programme.
Setting
Between March 2000 and May 2006 a demonstration pilot of biennial guaiac faecal occult blood test (gFOBT) colorectal screening was carried out in North-East Scotland for all individuals aged 50-69 years.
Methods
The relevant populations were subdivided, by gender, into four age groups and into five deprivation categories according to the Scottish Index of Multiple Deprivation (SIMD), and key performance indicators analysed within these groups.
Results
In all rounds, uptake of the gFOBT increased with age (P < 0.001), decreased with increasing deprivation in both genders (P < 0.001), and was consistently higher in women than in men in all age and all SIMD groups. In addition, increasing deprivation was negatively associated with uptake of colonoscopy in men with a positive gFOBT (P < 0.001) although this effect was not observed in women. Positivity rates increased with age (P< 0.001) and increasing deprivation (P > 0.001) in both genders in all rounds, although they were higher in men than in women for all age and SIMD categories. Cancer detection rates increased with age (P < 0.001), were higher in men than in women in all age and SIMD categories, but were not consistently related to deprivation. In both genders, the positive predictive value (PPV) for cancer increased with age (P < 0.001) and decreased with increasing deprivation (P < 0.001) in all rounds and was consistently higher in men than in women in all age and SIMD categories.
Conclusions
In this population-based colorectal screening programme gender, age, and deprivation had marked effects on key performance indicators, and this has implications both for the evaluation of screening programmes and for strategies designed to reduce inequalities.
Introduction
In Scotland the pilot consisted of three biennial rounds of screening carried out between 2000 and 2006. 10 In order to monitor the effectiveness of this pilot a series of key performance indicators (KPIs) were developed and these have been described previously. 10 Here we describe the effect of gender, age and deprivation on seven of the KPIs.
Methods
The methods used to carry out the United Kingdom demonstration pilot of colorectal screening have been described in detail elsewhere. 6 Briefly, the Scottish arm of this pilot was carried out in NHS Grampian, Tayside and Fife Boards, using biennial gFOBT using the Hemascreen® test kit (Immunostics Inc., Ocean, New Jersey, USA). This kit consists of six windows on to which small samples of faeces (two each from three separate stools) are placed by means of a disposable spatula. Those individuals with five to six windows positive on the initial test (strong positive) were offered colonoscopy, but if one to four windows were positive (weak positive) participants were asked to complete a further gFOBT and if any of the windows were positive colonoscopy was offered. Minor variations in this algorithm between the three rounds have been described previously. 10
Invitees consisted of all men and women aged 50 to 69 living in the three pilot NHS Boards. They were identified by the Community Health Index (CHI) and sent a test kit and invitation to participate via the postal service from a single Screening Unit located in Dundee. The CHI is a unique identifying number for everyone registered with a general practitioner in Scotland and is made up of date of birth followed by four digits from which gender can be identified. Completed tests were sent back in the post to the Unit Laboratory for analysis using specially designed hygienic foil envelopes. Individuals with a positive test were contacted by a specialist nurse who organized colonoscopy after obtaining informed consent.
Data for the KPIs were accumulated by data collectors employed by the Screening Unit and analysed by Information Services Scotland, a Division of NHS National Services Scotland. For the purposes of this analysis, gender and age were identified by the CHI and deprivation was assessed by place of residence (identified by post code) using the Scottish Index of Multiple Deprivation (SIMD). 11 The version of SMID used for this analysis comprised six domains: income, employment, education, housing, health and access to facilities.
The study population was subdivided into two groups according to gender, into four categories according to age at invitation (50-54, 50-59, 60-64 and 65-69 years) and into five categories according to the quintile of deprivation (1: least deprived quintile, 5: most deprived quintile). Pivot tables were then created to allow scrutiny of the KPIs according to gender, age and deprivation category and the results are presented here. In all cases the statistical significance of the observed trends was estimated by means of tests for linear trend using binomial regression. These tests were used to determine whether observed correlations were reliable. No correlations between age, gender and deprivation were found, and therefore adjusted analyses were not carried out.
Results
Associations between the study categories (gender, age and deprivation) and screening uptake, uptake of colonoscopy, positivity rate, cancer detection rate and positive predictive value (PPV) for cancer were sought, and the results are described below under these headings.
Uptake
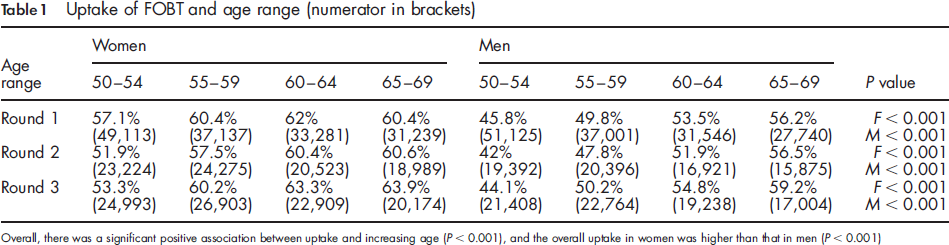
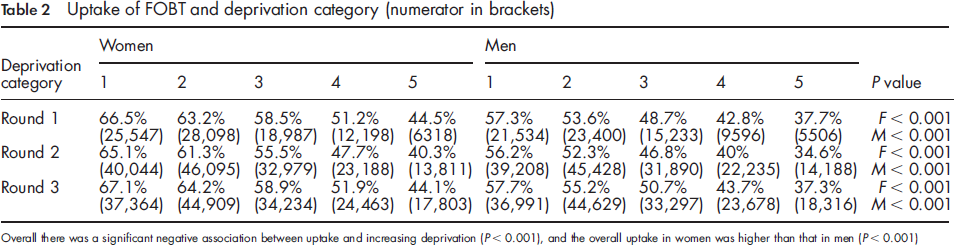
In the first round 304,245 people were invited and a gFOBT test result was obtained in 167,415; in the second round these figures were 309,803 and 164,077; and in the third round they were 317,864 and 175,853. This gives a first round uptake of 55.0%, a second round uptake of 53.0% and a third round uptake of 55.3%. In all three rounds uptake increased with increasing age (Table 1) and decreased with increasing levels of deprivation (Table 2). Uptake by women was consistently higher than by men in all age groups and in all deprivation categories.
Uptake of FOBT and age range (numerator in brackets)
Uptake of FOBT and deprivation category (numerator in brackets)
Uptake of colonoscopy
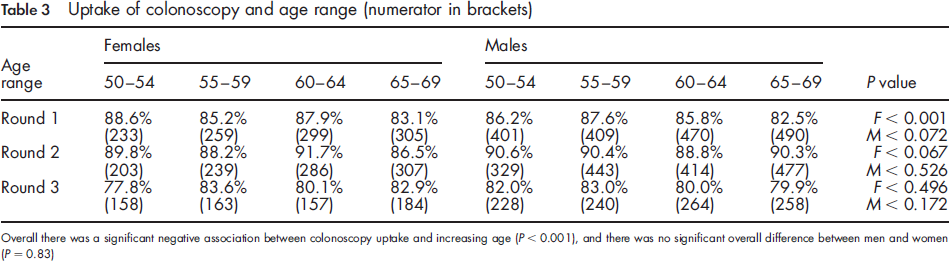
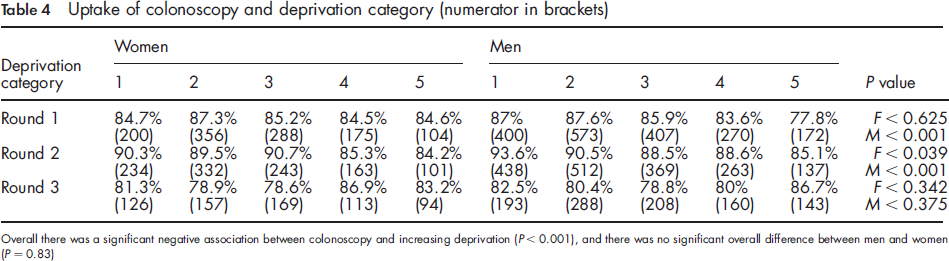
Among those with a positive gFOBT who were invited for colonoscopy 85.5% accepted in the first round, 89.5% in the second round and 81.3% in the third round. Although there was a negative association between uptake of colonoscopy and increasing age, this was only significant for women in the first round (Table 3). In the first and second rounds, there was decreased colonoscopy uptake with increasing deprivation although this was confined to men in the first two rounds and women in the second round (Table 4).
Uptake of colonoscopy and age range (numerator in brackets)
Uptake of colonoscopy and deprivation category (numerator in brackets)
Positivity
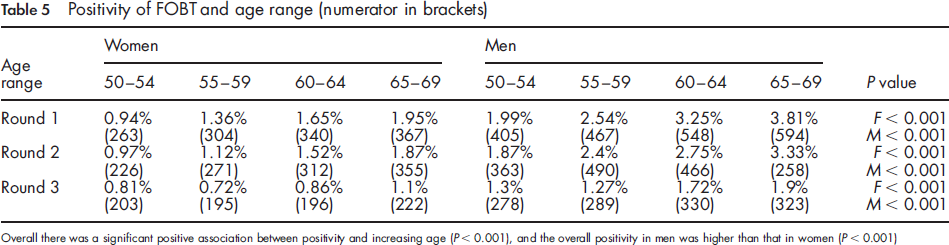
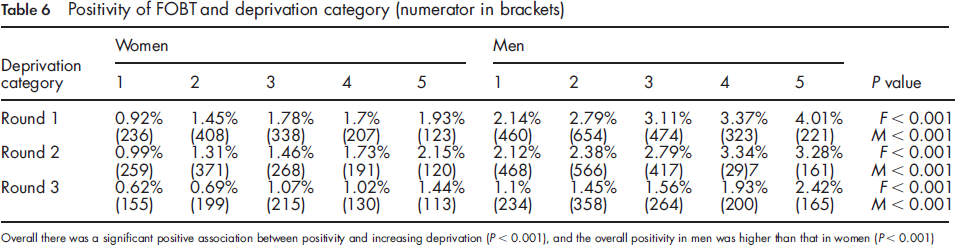
The percentage of individuals completing the gFOBT who had a positive result was 2.07% in the first round, 1.9% in the second round and 1.16% in the third round. Positivity increased with age (Table 5) and increased with increasing deprivation (Table 6) in all three rounds. Men had consistently higher positivity rates than women.
Positivity of FOBT and age range (numerator in brackets)
Positivity of FOBT and deprivation category (numerator in brackets)
Cancer detection rates
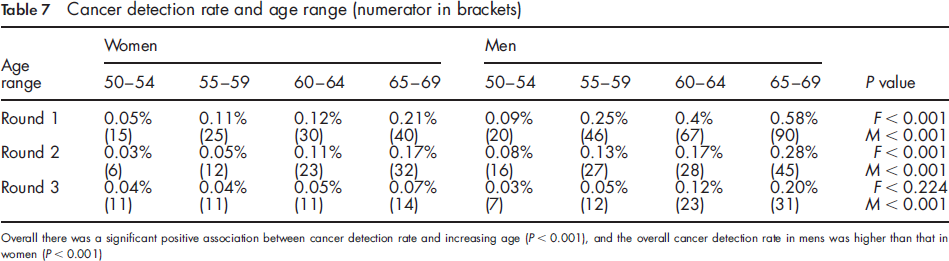
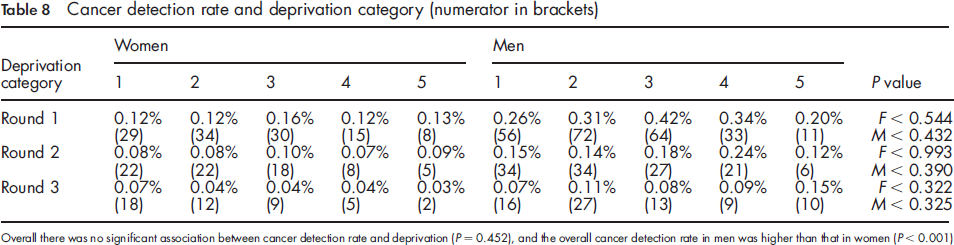
A diagnosis of cancer was made in 0.21% of those with an evaluable gFOBT result in the first round, 0.127o in the second round and 0.07% in the third. The cancer detection rate increased with increasing age in all three rounds and was consistently higher in men than in women (Table 7). There was no detectable association between cancer detection rate and deprivation (Table 8).
Cancer detection rate and age range (numerator in brackets)
Cancer detection rate and deprivation category (numerator in brackets)
Positive predictive value
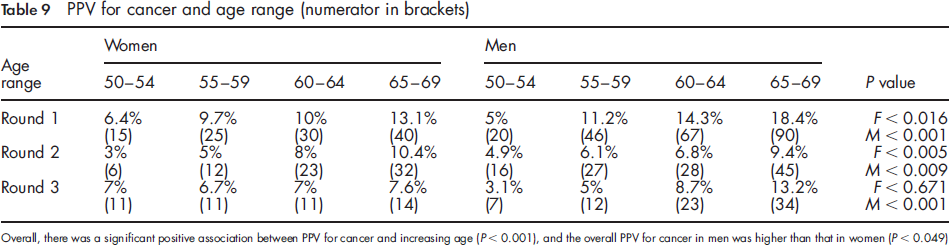
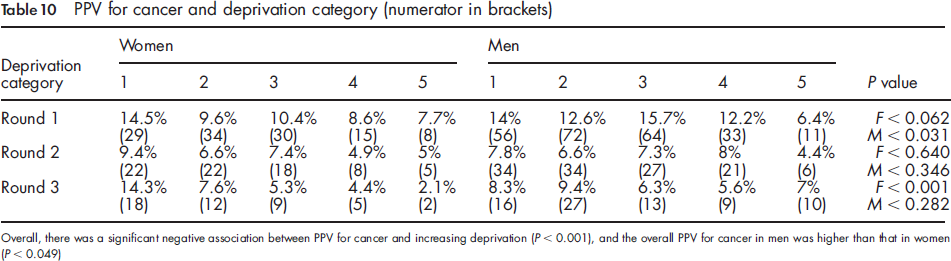
The PPV of a gFOBT for cancer was 12.0% in the first round, 7.0% in the second and 7.5% in the third; the corresponding figures for the PPVs for adenoma were 36.5%, 30.3% and 29.1% respectively. The PPV for cancer increased with increasing age (Table 9), decreased with increasing deprivation (Table 10) and was higher in men than in women in the first round, although this was not seen in the subsequent two rounds.
PPV for cancer and age range (numerator in brackets)
PPV for cancer and deprivation category (numerator in brackets)
Discussion
Population screening, where eligibility is defined solely by a fairly wide age range (in this case 50-69 years), by necessity embraces a heterogeneous group of individuals. Existing evidence suggests that gender, age and deprivation may influence the uptake of screening, and it is important to know if this and other key indicators of the performance of a specific screening programme are affected by these variables as this will influence the interpretation of such indicators. In addition, knowledge of how population variables affect the performance of a screening programme can inform methods of delivering the programme.
Uptake
Relatively little is known about the effect of gender on uptake of screening in general since, until recently, population screening for men has not been available. From the results of this study it is clear that, in Scotland at least, uptake of gFOBT colorectal screening is higher among women for all ages and deprivation categories, irrespective of round. This is in keeping with previous observations from the combined UK demonstration pilot 7 and from the second round of the pilot in England, 12 and also reflects the finding in the Nottingham randomized trial where the uptake of the first invitation was 51% in men and 55% in women. 2
Paradoxically, evidence from the United States suggests that men are more likely to undergo screening endoscopy than women 13 although, in some studies at least, the reverse seems to be true of gFOBT. 14 In addition, a large trial of flexible sigmoidoscopy screening carried out in the United Kingdom found that men were more likely than women to accept the invitation to be screened. 15 Although interesting, this body of evidence must be treated with caution as there are no population-based studies of gender-related acceptability of endoscopic colorectal screening from the US and the UK study was not strictly population-based. A recent population-based trial of flexible sigmoidoscopy screening from Norway 16 found that women were more likely than men to accept the invitation to be screened, lending weight to the concern that confounding factors had affected the other observations.
A higher uptake of gFOBT screening in UK women is not unexpected, given that cancer screening programmes have only recently been available to the female population and there is abundant evidence that men are less likely than women to seek health advice or make use of medical services. This makes the observations relating to the uptake of endoscopic screening all the more surprising. A subset questionnaire study from the UK flexible sigmoidoscopy trial has indicated that the higher attendance by men in this trial may be explained, at least in part, by lower levels of deprivation, higher levels of marital status and less in the way of perceived barriers to screening. 17 However, the hypothesis that men are more likely than women to accept endoscopic screening is not supported by the Norwegian experience and needs further testing in an unselected population.
Age is another important variable with respect to uptake, and in the 50-69 year range there was a steady increase of uptake with increasing age in the Scottish pilot. 10 A similar finding was reported from the English arm of the pilot,7,12 and in the United States, uptake of any form of colorectal screening seems to be higher in those over 65 years. 13 Of the randomized trials of colorectal screening, only the Nottingham study reported on this parameter and showed very little variation in uptake with age category other than a slight drop in the group aged over 70 years. 2 This difference may relate to a heightened degree of health awareness amongst older people in recent years.
The underlying reasons for an increased willingness for older age groups to engage with colorectal screening are not clear, but it is possible to speculate that more free time and increasing concern with health matters might contribute.
That deprivation adversely affects uptake of screening is well known from both breast18,19 and cervical screening. 20 The striking decrease in uptake of colorectal screening with increasing deprivation observed in the Scottish pilot is in keeping with the English pilot findings,7,12 and has been demonstrated previously for both FOBT screening 21 and flexible sigmoidoscopy screening. 22 The reasons for this are likely to be multiple, but there is good evidence that low health literacy is associated with perceived confidence to participate in screening 23 and literacy declines with increasing deprivation. 24 This is a particular problem with the UK FOBT screening programmes which rely heavily on printed information delivered by post.
Uptake of colonoscopy by those with a positive FOBT is a separate but related topic about which much less is known. From the present study it would appear that this is not related to gender and that the effect of age is small. Although higher deprivation is associated with lower uptake, at least in men, this is not nearly so marked as the effect of deprivation on uptake of the FOBT itself. Nevertheless, it is concerning that the uptake is so low, given that a positive FOBT defines a group that is at high risk of neoplasia. Previous work has shown that once verbal contact has been made with a health professional, uptake of colonoscopy is high, and the offer of a telephone consultation to discuss and arrange colonoscopy has been associated with a significant increase in uptake. 25
Positivity
When effects on the positivity of the gFOBT are being considered it must be appreciated that the test used in the UK pilots was guaiac-based and therefore subject to dietary interference from peroxidase activity in plants and animal haemoglobin. 26 In the Scottish pilot positivity was consistently higher in men than in women in all age groups and deprivation categories, and a similar association with gender was seen in the English pilot.7,12 The same finding has been reported, although not in detail, in the previous randomized trials.1,3 This is consistent with the increasingly strong evidence that male sex is a risk factor for advanced colorectal neoplasia, 27 but the possibility remains that a gender difference in diet may have contributed.
Positivity also increases with increasing age as evidenced by the present study, the data from England7,12 and the randomized studies1,3 and, again, this probably relates to prevalence and incidence of advanced neoplasia, although other factors cannot be discounted. More interesting, however, is the increase in positivity with increasing deprivation. Although there appears to be a slight increase in colorectal cancer incidence with increasing deprivation in the Scottish population, 28 the cancer detection rate in the screened population does not vary with deprivation as evidenced by the present study. It is therefore likely that dietary factors account for this finding, and if this is the case, it highlights one of the limitations of the guaiac test.
Cancer detection and PPV
The cancer detection rate (i.e. the detection rate of cancer and adenoma in those screened) was higher in men than in women, reflecting the evidence that the disease has a higher incidence in men than in women, especially in the age group (50-69) offered screening in the Scottish pilot. 29 This observation is in keeping with the higher positivity observed in men, and although, as discussed above, it is impossible to exclude other causes such as diet, the higher PPV seen in men suggests that this is related primarily to a higher burden of disease.
Not unexpectedly, the cancer detection rate and the PPV of the gFOBT increased with increasing age. More surprising were the findings with deprivation. Although higher levels of deprivation were associated with increased positivity, there was no association with cancer detection rate and the PPV fell with increasing deprivation. Thus people from deprived communities are more likely to have a false-positive gFOBT and hence an unnecessary colonoscopy.
Conclusion
In summary, the main findings from the study of the Scottish demonstration pilot of gFOBT colorectal screening are that uptake and positivity and PPV are all affected by gender, age and deprivation, whereas neoplasia detection rates are affected by gender and age only.
An obvious implication of these findings is the need to improve uptake by targeting men and deprived communities, and the latter is particularly relevant given the evidence that the outcome in colorectal cancer patients is adversely affected by deprivation.28,30 It would seem appropriate to investigate alternative means of invitation or perhaps different test formats, and careful research is needed to identify the optimum methods of reducing inequalities in this area.
The findings related to age indicate that the older age groups are more likely to benefit from screening, at least as far as cancer detection is concerned, and are more willing to participate. It would therefore seem appropriate to consider setting the upper age limit of screening above 69 years, and indeed, for roll-out of the screening programmes throughout the UK this limit either has been or will be increased to 74 years.8,9
Finally, the issue of the PPV of the gFOBT is important as this determines the number of negative (and therefore unnecessary) colonoscopies that are carried out. While the relationship between PPV and both gender and age may largely be explained by differences in disease prevalence, this is not the case with deprivation. While more deprived populations have higher positivity rates, the test has a lower PPV, indicating a higher incidence of positive tests that are not caused by neoplasia. Although the reason for this is currently obscure, dietary habits offer a possible explanation. Previous research utilizing faecal immunological testing has shown that a substantial proportion of people with a positive gFOBT do not have detectable blood in their stool, 31 and it will be important to determine whether or not such human haemoglobin-specific testing circumvents this issue.