
Abstract
Objective
To evaluate cervical cancer incidence among women born in different countries but residing in Italy.
Setting
Women aged 25-59 from a central Italian population-based cancer registry.
Methods
Invasive and in situ cervical cancer incidence rates from 2000-2004 were calculated. Standardized incidence rates were based on the European standard population. Places of birth were categorized by nine different areas.
Results
Within the resident population aged 25-59, there were 148 invasive cervical cancers (17.6% in women born outside Italy) and 501 (14.2% in women born outside Italy) cervical intraepithelial neoplasia grade III (CIN III) diagnoses. The incidence of invasive cervical cancer for women born in ‘Central & South America and the Caribbean’ was 60.5 per 100,000 and in ‘Central and Eastern Europe’ it was 38.3, statistically significantly higher than for women born in Italy (9.5 per 100,000). The CIN III rate was 35.0 per 100,000 for women born in Italy. The ratio between standardized rates for CIN III and invasive cancers was around 4 for women born in Italy and the ‘extended European Union’, and around 6 for those born in ‘Asia’. It was 1.64 for women born in ‘Africa’, 1.31 in ‘Central & South America and the Caribbean’ and 0.69 for those born in ‘Eastern Europe’.
Conclusions
Women who reside in Italy but were born in ‘Central & South America and the Caribbean’ or in ‘Central and Eastern Europe’ are at high risk for invasive cervical cancer. These groups are less inclined to participate in screening, and appropriate preventive strategies should be planned accordingly.
Introduction
A case-control study carried out in central Italy 8 showed that women born outside Italy were less likely to undergo a Pap test, in comparison with women born in Italy (56.8% versus 31.6%; P < 0.01).
Cancer registries collect data on newly diagnosed cancers among the resident population, without taking into consideration the place of birth. Place of birth may increase the risk of cervical cancer due to the higher prevalence of HPV infections and/or to a lower Pap test compliance. The aim of our study was to evaluate cervical cancer incidence in central Italy according to the areas of birth of resident subjects.
Methods
We considered cervical cancer incidence-both invasive and CIN III-during 2000-2004 and within the Tuscan Cancer Registry coverage area. The registry has been active since 1985 in the provinces of Florence and Prato in central Italy (around 1,200,000 inhabitants). This registry has been widely described elsewhere. 9 Cases of invasive cancer and CIN were identified through hospital discharge notes, pathology reports, death certificates, oncological archives (radiotherapy, screening, etc.) and general practitioner consultations. In estimating incidence rates, we used as denominator the official health archive of residents in Tuscany, kept by the regional public health system, which includes the variable city/state of birth. Further information about this archive can be drawn from the official Tuscany website (specifically in the health files section http://www.sanita.toscana.it/risorse/manuale-flussi.shtml, SAA). 10 The date of registration in the archive is updated whenever a patient changes general practitioner within a Local Health Unit, or moves from one Local Health Unit to another. Therefore, information about age at the time of registration and about time since registration are only a rough approximation of age at the time of migration and time since migration.
Places of birth were grouped into the following nine geographical areas:
Italy
Extended European Union: Austria, Belgium, Denmark, Finland, France, Germany, Greece, Ireland, Luxemburg, The Netherlands, Portugal, United Kingdom, Spain, Sweden, Switzerland, Iceland, Norway and Liechtenstein
New entries to the European Union: Czech Republic, Cyprus, Estonia, Latvia, Lithuania, Malta, Poland, Slovakia, Slovenia, Hungary
Central & Eastern Europe: Albania, Belarus, Bosnia-Herzegovina, Bulgaria, Croatia, Serbia and Montenegro, Macedonia (FYRoM), Moldova, Romania, Russian Federation, Turkey and Ukraine
North America
Central & South America and the Caribbean
Asia
Africa
Oceania
This classification refers to the period in study (2000-2004) and therefore does not include Romania and Bulgaria, which joined the EU in 2007.
In Italy, if provided by the public health system, emergency care, hospital admission and screenings are free of charge, whilst other healthcare services are partially subsidized. The analysis was restricted to the 25-59 year old age group, given the low proportion of elderly subjects among the immigrant population. In computing standardized incidence rates, we used the European standard population. 11
Results
During the period 2000-2004, the Tuscan Cancer Registry recorded 304 diagnoses of invasive cervical cancer: 27 (8.9%) cases were in women born outside of Italy and 277 cases were in women born in Italy. In the age group under study, the diagnoses were 26 among the cases born outside Italy (96.3%), whilst 122 (44.0%) among the cases born in Italy.
Tuscan Cancer Registry, 2000-2004, age 25-59 years
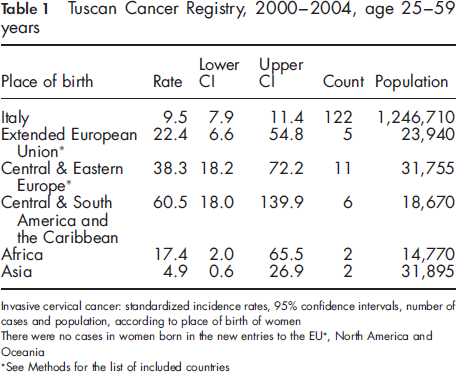
See Methods for the list of included countries
The incidence of invasive cervical cancer was 9.5 per 100,000 women born in Italy, statistically much lower than for women born in ‘Central & South America and the Caribbean’ (60.5), and in ‘Central and Eastern Europe’ (38.3). There were no significant differences between women born in Italy and women born in the ‘extended European Union’, ‘Africa’ and ‘Asia’. In the analysed period there were no cases in women born in ‘North America’, ‘Oceania’ and in the ‘new entries to the EU’. In the same period (2000-2004) there were also 501 registered cases of CIN III in the 25-59 year old age-group, of which 71 (14.2%) were in women born outside Italy.
Tuscan Cancer Registry, 2000-2004, age 25-59 years
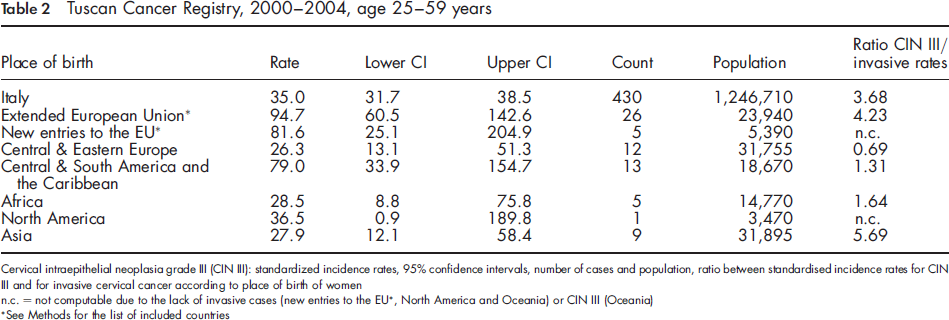
See Methods for the list of included countries
Table 2 also shows the ratio between standardized rates for CIN III and invasive cancers by area of birth. This ratio was around 4 (i.e. four times higher for CIN III than for invasive cervical cancers) for women born in Italy and in the ‘extended European Union’, and around 6 for those born in ‘Asia’. The ratio was just above unity for women born in ‘Africa’ (1.64), ‘Central & South America and the Caribbean’ (1.31) and lower than unity (0.69) for those born in ‘Eastern Europe’.
The age at registration in the Tuscan health archive of residents was not different for women born in and outside Italy (32.4 years versus 33.8, P = 0.22), either for invasive (35.6 versus 35.5) or for noninvasive neoplasms (31.6 versus 33.1). The mean time between registration and cervical neoplasia incidence was 8.0 years for women born in Italy, and 5.7 years (P = 0.007) for those born outside Italy.
Discussion
The present study, carried out in central Italy, shows that the risk of invasive cervical cancer in the resident female population varies according to geographical area of birth. In particular, the risk is significantly higher for women born in ‘Central & South America and the Caribbean’ and ‘Central and Eastern Europe’ than for women born in Italy.
This result is probably the consequence of two factors-reduced participation in screening, and higher prevalence of HPV infection. The first factor is confirmed by a recent survey on cervical screening carried out in Prato, 12 a municipality of about 185,000 inhabitants within the Tuscan Cancer Registry area. This municipality has the highest proportion of foreign resident citizens in Tuscany (13.0% versus 8.4% regional mean, according to the estimates at 1 January 2008). 1
The survey shows that the participation in cervical Pap test screening was markedly lower for women born outside Italy (28.4%) than for women born in Italy (62.6%). 12 As has been observed in studies from Canada, the area of birth may be a marker of cultural differences that explain the disparities in cervical cancer screening practices, with lower participation observed among those at higher risk of invasive lesions.6,13
A previous case-control study carried out in central Italy 8 observed that the odds ratio of having a Pap smear was higher in women born in Italy than in those born outside Italy. In the survey carried out in the municipality of Prato, 12 the detection rate for CIN II+ lesions was 8.3%o for foreign women and 2.2%o for Italian women, but numbers were small and the conclusions may not have been reliable. However, assuming that the prevalence of CIN III in our study was higher in women born in ‘Central & South America and the Caribbean’ and ‘Eastern Europe’ than in women born in Italy, or at least the same in the two groups, the low incidence of CIN III we observed may be an indication of low cervical screening attendance.
Although we do not have a direct measure of the second factor (higher prevalence of HPV infection), the study by Zappa et al. 8 concluded that women born outside Italy were less common among controls than among cases (invasive cervical cancer) (0.7% versus 3.4%, P = 0.002). This seems to indicate an increased baseline risk due to a higher prevalence of HPV. Such a prevalence (47.8%) has been increasingly detected in female immigrants to Italy from sub-Saharan Africa and Eastern Europe. 14
Overall the results of our study are consistent with the literature on the variation in prevalence of HPV infection across the world, which demonstrates that the highest values are in those areas where we have observed the highest cervical cancer incidence rates. Two recent Swedish studies confirmed that the risk of cervical cancer was particularly high for women born in Central America 15 and Eastern Europe, 16 and also established a relationship between the risk of cervical cancer and both age at the time of migration and duration of residence.15,16 We cannot confirm these latter findings for Italy because we do not have reliable data on age at the time of migration, or on the duration of residence.
As an approximate time of immigration we used the date of registration of residents in the Tuscan health archive. This information is unreliable because the registration date is amended whenever a resident changes address or general practitioner. Therefore, information on age at registration and on time since last registration are only rough markers of age at the time of migration and time since migration. With this caveat, it might be noted that the mean time since registration and cancer incidence is shorter for women born outside Italy than for those born in Italy. This discrepancy should be further investigated because of the unreliability of the data, but possible causes might include a higher migration rate within the area for immigrants than for those born in Italy and the fact that the registration in the official health archive is made upon a health issue.
To retrieve exhaustive information about the date of immigration is impossible, as many individuals enter the country illegally, and the Tuscan Cancer Registry only collects data regarding official residents. Therefore, nonresidents, including illegal residents, are not included in the registry. In Italy about 15% of immigrants are illegal. 17 We have not included these subjects in our study because it is difficult not only to identify incident cases, but also to estimate a suitable denominator. However, it is probably valid to assume that the risk is high among illegal immigrants, who tend not to attend health and preventive services.
Conclusion
Our results demonstrate that, within the resident central Italian population, women born in ‘Central & South America and the Caribbean’ and in ‘Central and Eastern Europe’ are at high risk of invasive cervical cancer, and are also less likely to participate in screening. healthcare providers and policy makers should plan culturally appropriate preventive strategies in order to bridge the gap between this group and the local health services.