
Abstract
Objectives
Evidence from existing UK screening programmes indicates disparities in uptake rates between UK ethnic minorities and the white majority population. The aim of this study was to explore barriers to the uptake of flexible sigmoidoscopy (FS) screening among UK ethnic minority populations. Specifically, beliefs about bowel cancer, perceived barriers to the test and ideas about ways to increase uptake were investigated.
Methods
Nine focus groups were conducted with a total of 53 participants from African-Caribbean, Gujarati Indian, Pakistani and white British communities. The topic guide was based on the Health Belief Model. Discussions were subject to framework analysis.
Results
Most participants expressed limited awareness of bowel cancer and cited this as a barrier to screening attendance. Anxiety regarding the invasiveness of the test, the bowel preparation and fear of a cancer diagnosis were common barriers across all ethnic groups. Language difficulties, failure to meet religious sensitivities and the expression of culturally influenced health beliefs were all discussed as specific barriers to uptake. Ethnically tailored health promotion and general practitioner involvement were recommended as ways of overcoming such barriers.
Conclusions
The study was the first attempt to qualitatively explore barriers to FS bowel cancer screening in UK ethnic minorities. Most barriers were shared by all ethnic groups but health educators should supplement approaches designed for the majority to incorporate the specific needs of individual minority groups to ensure equitable access.
Introduction
In a recent UK pilot study that assessed the feasibility of a nurse-led FS screening programme, 55% of individuals invited to have screening accepted. 3 This figure is similar to the second round of FOBt screening across England, where 51% of participants returned a kit. 4 While these figures are low compared with the higher uptake rates of other screening services (e.g. breast screening, 75% 5 ), they can be seen as positive in the light of the limited publicity bowel screening has had. 4 However, it is likely that these overall uptake rates mask lower participation among ethnic minority communities. Evidence suggests that screening participation in existing programmes (breast, cervical and bowel) is lower among ethnic minority groups.6–9 Indeed, a recent study noted lower FS screening attendance among Asian communities compared with white and African-Caribbean participants, despite equal initial interest (54%, 69% and 80%, respectively). This difference could not be explained by socioeconomic status (SES) or poor health. 10
One study has specifically explored barriers to FS screening in UK ethnic minority groups, adding open-ended questions to a nationwide survey of the main ethnic minority groups, known as the Ethnibus Survey. 11 While there was high interest in screening, ethnic minority groups had lower levels of CRC awareness than white British adults and embarrassment was identified as a key barrier in the ethnic minority respondents. This study provided some suggestions about barriers to FS screening but was limited by the small number of questions and relatively few respondents were within the target age range for screening.
Much of the research assessing screening behaviour has drawn upon the Health Belief Model (HBM).12, 13 Research in the FS screening literature has supported the tenets of the HBM demonstrating that threat, barriers and benefits of the test can predict approximately 47% of the variance in interest to FS attendance. 14 Also, a recent review of factors associated with participation in CRC screening showed that perceived benefits and barriers of screening are consistently related to uptake. 15
The aim of the present study was to explore perceived barriers to FS screening among UK ethnic minority groups using a qualitative methodology. With the Health Belief Model as a framework the present study also examined lay recommendations to increase FS screening participation.
Method
Participants and procedures
Participants (n = 53) were from African-Caribbean, Gujarati Indian and Pakistani communities with white British participants included for comparison. All participants were recruited through community groups in London. Organizations were identified through the Internet, Yellow Pages or through contacts made in other centres. Participants self-selected from interested community groups responding to posters, a group address at a regular meeting or through an invitation sent to the organization's mailing list. Participants’ ages ranged from 50 to 78 years reflecting the target age group for FS screening.
A total of nine focus groups were conducted between February 2007 and July 2008. The groups tended to be single sex, unless participants requested both men and women be invited to the group (e.g. the African-Caribbean groups). A bilingual interpreter was used for some groups to ease communication (Indian Women's group).
The topic guide, based on the Health Belief Model, covered four core domains – perceptions of risk and severity of bowel cancer, benefits of the FS test, barriers to screening uptake, and recommendations to increase test attendance. Groups were given background information about bowel cancer and a description of the FS procedure, including a graph, a figure showing the location of the bowel in the body, a picture of the equipment and pictorial images of polyp removal 16 to ensure consistent baseline knowledge across groups (see Box 1). Participants also completed a demographic questionnaire assessing age, gender, religious status, country of origin, length of residence in the UK, education and employment.
Topics included in the focus group presentation
Bowel cancer incidence and cause
Timeline of cancer development
The flexible sigmoidoscopy test:
Is a preventive tool, aimed at stopping the development of cancer Uses a small camera inserted into the back passage to locate and remove polyps found in the bowel Is hospital-based and takes five minutes to complete Requires that an enema be conducted at home before the test is performed
Data analysis
Focus groups were tape-recorded, transcribed verbatim and checked twice to ensure accuracy. Transcripts were examined using ‘Framework analysis’ 17 – a matrix-based approach, whereby a priori issues, emergent themes and recurrent attitudes are organized into a thematic framework. Acceptability of themes was independently assessed.
Results
Demographic characteristics
Demographic details of the participants are summarized in Table 1.
Demographic characteristics of the sample
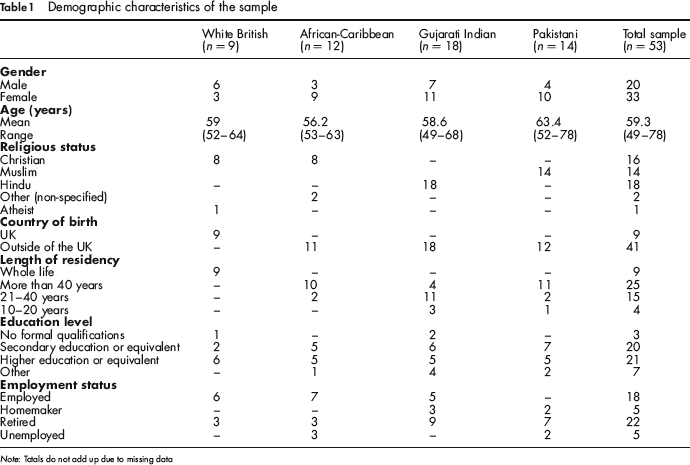
Note: Totals do not add up due to missing data
Beliefs about CRC
Perceived severity
Participants across all ethnic groups commented that bowel cancer was serious, although neither the white British nor the Pakistani men felt they could give an informed answer because of their lack of knowledge on the subject. The African-Caribbean, Pakistani and white British groups held a general model of cancer in which ‘all cancers are serious’ (African-Caribbean woman) regardless of type.
Perceived susceptibility
Few groups talked about their personal susceptibility to bowel cancer; two of the Pakistani focus groups felt they did not know anything about susceptibility, and lack of awareness about bowel cancer also led the white British men to infer it was rare. While bowel cancer was thought to be common in the UK, both the Indian and African-Caribbean groups considered it to be less common among their communities: ‘I'm still a little bit not aware that it is prevalent, especially in these ethnic groups, Asians’ (Gujarati Indian man). It was suggested that communities with different food habits would be more affected: ‘we are different because our diet is predominantly fibre-based,… so maybe there isn't a lot in our community’ (Gujarati Indian man).
Interestingly, both Pakistani and African-Caribbean women commented they thought it was a disease that affected men only.
Perceived benefits of FS screening
Participants across all ethnic groups reported that the major benefit of FS screening was its ability to prevent the occurrence of CRC. It was described as a ‘definitive’ test, removing the ‘potential’ for pre-cancerous polyps to become malignant:
‘If you can pick this [bowel cancer] up at a much earlier stage and prevent something nasty, a killer disease basically at a later date, then surely it would make sense to go through a bit of discomfort’ (Gujarati Indian man).
Another commonly quoted benefit of the test, cited by all ethnic groups, was the ‘peace of mind’ provided by getting results immediately. The Pakistani groups also commented upon the reduction of invasive treatment:
‘Obviously if things are picked up earlier they are much easier to handle and you don't have to go through that drastic treatment system that you need to when things get so bad’ (Pakistani woman).
Perceived barriers
Procedural barriers
Views about the test itself were mixed. Gujarati women were not deterred by the nature of the procedure:
‘The FS test is only putting a tube in your back passage and testing you, so there is nothing that can put you off (Gujarati woman).
All other groups expressed concerns regarding the invasiveness of the test and the area of the body under investigation:
‘Well it is a bit of a private area I suppose that is the thing and having people invading that would make me think twice about it’ (white British man).
The risk of bowel perforation, discomfort and the likelihood of missing polyps were discussed by African-Caribbean, white British groups and Gujarati Indian men, although were not thought to be a barrier to attendance.
In the FS pilot programme participants carry out the bowel preparation (enema) at home and this was identified as a barrier to taking part. Gujarati Indian men described using the enema at home as ‘bad’, white British participants said they would ‘probably be quite dramatic about the enema’ (white woman) and one African-Caribbean participant described it as ‘self harm’. Lack of confidence in completing the enema was a barrier across all groups except Gujarati Indians, for example: ‘I just have never done anything like that so I would be frightened of it getting lost up there or something’ (African-Caribbean woman).
Psychosocial barriers
Overall, embarrassment was not considered a major obstacle, especially if a female doctor was present.
Across all ethnic groups except the Pakistanis (who did not comment), fears centred on the results of the test and what they might mean. This was described in terms of ‘…a fear of the unknown…’ (African-Caribbean woman), that one would not be able to cope with the fear that surrounds a diagnosis and ‘…the word cancer…’ (white British man).
‘I feel like that sometimes and that keeps me from going for a test, you are afraid of the results even though you might have nothing to worry about, the fact that it is still up there, you suppose it is bad news and you would rather not want to know about it’ (African-Caribbean woman).
The female Pakistani group also talked about their attitudes to cancer treatment. Some women in the group were reluctant to seek treatment believing that the treatment itself would cause the cancer to advance: ‘So they believe that it was better without treatment and once you start treatment it gets worse’ (Pakistani woman).
Lack of symptoms
Gujarati Indian and Pakistani groups were reluctant to attend the test without experiencing symptoms, even though they understood its preventive nature:
‘I do not like screened without any reason…. Why should I get something put in my body if there is nothing wrong with me?’ (Gujarati Indian woman).
This was a common theme, with Pakistani participants stating they only attended other screening services (cervical and breast) when they noticed symptoms:
‘I used to get appointment through that the doctor sent me about the smear test and I always just ignored it, then when there was a problem I rushed and I insisted I want to have a smear test’ (Pakistani woman).
Culturally influenced barriers
Both Pakistani men and women expressed the need for women to have a female endoscopist, in accordance with their religious beliefs. Concerns over whether this could be guaranteed and the attitudes of staff in accommodating this requirement contributed to feelings of reluctance about attending screening:
‘They just make you feel uncomfortable [for requesting a female nurse]. So that is why I don't go, if I got the test I would say no I don't want to go because of this thing’ (Pakistani woman).
In addition, the Pakistani group held a very biomedical view of the health-care system, refusing to attend the test unless told to go by the general practitioner (GP):
‘It is up to the medical profession what they do, it is not up to the public to tell them what to do, it is the medical profession who suggests it and to tell them what to do’ (Pakistani man).
Language difficulty was the only culturally specific barrier raised by the Gujarati Indian participants. Discussions among African-Caribbean groups included the problem of machismo among men in their community citing their dislike of ‘anything up their rectum’ (African-Caribbean woman) and: ‘They say they are all man, especially if it was a man, they would say you are not pushing anything up there’ (African-Caribbean woman). The test was also considered to be a threat to masculinity: ‘an attack on your armour’ and ‘If you go to the doctor you are considered more feeble than other men, because other men don't have to go and do that’ (African-Caribbean man).
Gender
African-Caribbean men were considered less likely to attend screening than women due to their beliefs about the health service noted above. This gender difference was also discussed by both the Indian and white British men who suggested men would be ‘more embarrassed’ and more likely to ‘suffer in silence’ than women.
Lack of awareness
Lack of awareness about screening was considered to be a barrier to attendance: ‘if you don't have much knowledge people may not attend’ (Pakistani woman). Gujarati Indian participants thought that lack of knowledge was associated with more fear:
‘Without little knowledge on what is going to happen, if no one explained then I do not want to go for the test, there is a little bit of fear and whether it is safe, but after explanation you might consider having it done’ (Gujarati Indian man).
The lack of publicity of cancer was commented on in the African-Caribbean group who discussed cancer as a ‘taboo’ within their community:
‘You ask people to tell you all the things, the health issues that they'd want to promote and cancer never ever came up’ (African-Caribbean woman).
Recommendations to increase attendance to the FS test
The recommendations to increase participation are presented in Box 2.
Recommendations to increase attendance to flexible sigmoidoscopy screening
Discussion
The results of this study broadly fit within the constructs of the HBM, with participants elaborating in detail on the barriers to attendance and the cues to action that could overcome them.
In line with previous work, 11 there was limited understanding of CRC in any group, and this was considered a barrier to participating in FS screening. Although there was agreement among groups that CRC is a serious disease, both the Gujarati Indian and African-Caribbean groups considered themselves to be at low risk, and the white British men considered it to be rare.
The majority of reported barriers were shared by all participants, with fear of the results a commonly cited deterrent. All groups, except the Pakistanis (who did not mention it explicitly), expressed concerns on how they would cope with a cancer diagnosis. Fear is frequently cited as a barrier to screening uptake and cancer awareness,13, 18 and fatalistic attitudes to cancer were associated with lower test attendance among African-Americans. 19 Emphasizing the preventive nature of FS screening may help to counter these fatalistic beliefs.
Contrary to previous work, 11 embarrassment about the screening procedure was not considered to be a significant deterrent. This conflicting result could be due to differences in the recruitment strategies used by the two studies. The self-selecting nature of the focus groups may have excluded those who find the idea of bowel screening embarrassing compared with those participants opportunistically approached by the Ethnibus Survey, 11 a nationwide survey of the main ethnic minority groups living in the UK. In addition, relatively few participants in the Ethnibus survey sample fell within the target age range for screening and it is possible that the older participants in the focus groups may have had more experience of invasive medical procedures over the years and have come to find them less embarrassing.
Few ethnic-specific differences were raised as barriers to the test. This is surprising given the evidence of ethnic differences in uptake across many types of cancer screening in the UK.10, 20 However we believe that perceived barriers were comprehensively explored among all the groups and they were conducted in such a way that participants felt comfortable expressing their views, so any ethnic-specific differences would have emerged. Pakistani participants raised concerns about having a male health-care professional conduct the test on women and a lack of trust in the hospital's ability to meet their religious needs. Gujarati Indian women expressed difficulties due to language barriers both in the hospital and in understanding promotional material. Perceptions of cultural insensitivity and language problems echo barriers expressed in breast and cervical screening research, indicating a need for greater engagement on this issue among health practitioners and staff and possible change at the practice level.21, 22
African-Caribbean participants also highlighted the reluctance of some men in their community to have the test because they regarded it as a challenge to their masculinity. However, a recent study examining screening uptake figures indicated no significant difference between African-Caribbean men and women and research has suggested this reluctance is not exclusive to African-Caribbean men.10, 23
Pakistani women discussed the belief that receiving cancer treatment made the cancer spread. Data from a more representative sample would be needed to confirm whether this is a commonly held belief within the community.
All ethnic groups thought that discussion forums were the best form of communication, although a national campaign including ethnic media channels was also necessary. Respondents suggested promotions should include both a ‘hard-hitting’ message followed by information on the importance of the test. This is in line with the Extended Parallel Process model 24 which proposes that threat messages should be followed by high-efficacy statements to motivate action to change.
Also of note was the widespread desire for GP involvement either in the form of referral letters or as the screening location. A recent qualitative study assessing GP attitudes towards the UK FOBt pilot reported their patients often looked to them for endorsement of the test. 25 More extensive work is needed to consider GP acceptability and the feasibility of conducting the test at a health centre.
The study has a number of limitations. Recruitment and facilitation of the Pakistani men's group had limited success. Men were older than the target age-group and were reluctant to discuss the subject of bowel cancer or screening. Training an age-matched community leader to run the group may have resulted in more in-depth responses. The self-selection recruitment method may have reduced how representative the sample was and barriers could be different on a population wide basis. This may also be pertinent considering that the majority of participants had achieved a higher level of education and were employed. While the representativeness of the sample is a concern, past research 10 has suggested that SES did not explain ethnic differences in FS screening uptake. Furthermore, not all participants in the groups said they would have the test, suggesting that a range of views was achieved.
The findings have several implications for increasing uptake of screening among ethnic minority groups. Reflecting on the invitation strategies used in the UK FS Trial and the Nurse-led Feasibility study,3, 26 several adaptations could be made to encourage attendance from ethnic minority subgroups should FS screening be introduced. The need to address different language needs was cited as a barrier by the Indian participants and therefore the use of language-appropriate information aids could be beneficial. Further endorsement from the GP and the use of ethnic media to promote the test may complement the invitation process and could be used to address issues surrounding test stigma and lack of awareness. The results also suggest attempts should be made to allay fears surrounding religious sensitivities. Across all ethnic groups there was overwhelming support for the use of discussion forums to inform communities about the test. Training community facilitators to act as advocates could raise test awareness. This would also provide community endorsement, which was suggested to be important by African-Caribbean, Indian and Pakistani groups.
These results are the first attempt to qualitatively assess the barriers to FS screening facing UK ethnic minority groups. Quantitative work from representative samples, including participants from a wider socioeconomic background, is needed to determine the generalizabilty of the barriers discussed. Building a broad picture of the barriers to FS screening will help ensure equitable access and participation should FS bowel screening be added to the National Cancer Screening Programme.