
Abstract
Objectives
To explore barriers to cervical screening attendance in a population-based sample, and to compare barriers endorsed by women who were up-to-date with screening versus those who were overdue. We also tested the hypothesis that women who were overdue for screening would be more generally disillusioned with public services, as indexed by reported voting behaviour in elections.
Setting
A population-based survey of women in England.
Methods
Face-to-face interviews were carried out with 580 women aged 26–64 years, and recruited using stratified random probability sampling as part of an omnibus survey. Questions assessed self-reported cervical screening attendance, barriers to screening, voting behaviour and demographic characteristics.
Results
Eighty-five per cent of women were up-to-date with screening and 15% were overdue, including 2.6% who had never had a smear test. The most commonly endorsed barriers were embarrassment (29%), intending to go but not getting round to it (21%), fear of pain (14%) and worry about what the test might find (12%). Only four barriers showed significant independent associations with screening status: difficulty making an appointment, not getting round to going, not being sexually active and not trusting the test. We found support for our hypothesis that women who do not attend for screening are less likely to vote in elections, even when controlling for barrier endorsement and demographic factors.
Conclusions
Practical barriers were more predictive of screening uptake than emotional factors such as embarrassment. This has clear implications for service provision and future interventions to increase uptake. The association between voting behaviour and screening uptake lends support to the hypothesis that falling screening coverage may be indicative of a broader phenomenon of disillusionment, and further research in this area is warranted.
Background
Rather than asking women to explain the reasons for their attendance or non-attendance for screening, as has been the case in much previous and especially qualitative research,12,14,15 we used a population-based survey and asked all participants about potential barriers to uptake. This methodology was chosen to reduce the likelihood of women feeling the need to justify or come up with post hoc rationalizations for their lack of attendance. This also allowed us to compare barrier endorsement among women who attend regularly for screening versus those who are intermittent or non-attenders.
Building on the previous literature, the aims of the study were to
Explore practical and attitudinal barriers to cervical screening participation in a population-based sample of women in the screening age-range;
Compare barriers endorsed by women who are up-to-date versus overdue for screening;
Test the hypothesis that women who are more disillusioned with public services (indexed by reported voting in elections) are less likely to attend for screening.
Methods
The study was approved by the UCL Research Ethics Committee. Data were collected as part of the Office for National Statistics (ONS) ‘Opinions’ survey in December 2008 and January 2009. The ‘Opinions’ survey is an omnibus social survey, carried out on a monthly cycle and includes questions from government departments, academic institutions and charities. It has the advantage that a wide range of topics is included in any given month, so self-selection on the basis of subject area is avoided. The ONS uses stratified random probability sampling to select 2010 addresses from the postcode address file for each survey. Across the two surveys, 4020 addresses were selected. Three hundred and seventy-three were ineligible, giving a total eligible sample of 3659. For each wave, the refusal rate was 30%. In addition, no contact was made with 10% of households in the first wave, and 8% in the second wave, giving an overall response rate of 61% (60% in December and 62% in January). The total sample size was 2216 people.
Sample
Our questions were only asked to women aged 25 years and over, living in England (as the screening recommendations vary between England and the rest of Britain). The sample size in this group was 797, of whom 648 were aged 25–64 years. Of these, 50 women who reported having a hysterectomy, seven who did not know their screening status and one who did not answer the question about cervical screening attendance were excluded from analyses. We also decided to exclude women aged 25 years (n = 10) as they might not have received their first screening invitation. This left an evaluable sample of 580.
The majority of the data collection used face-to-face computer-assisted interviews carried out at people's homes, although 4% of participants (n = 23) took part in telephone interviews, used when attempts to visit the household had been unsuccessful.
Measures
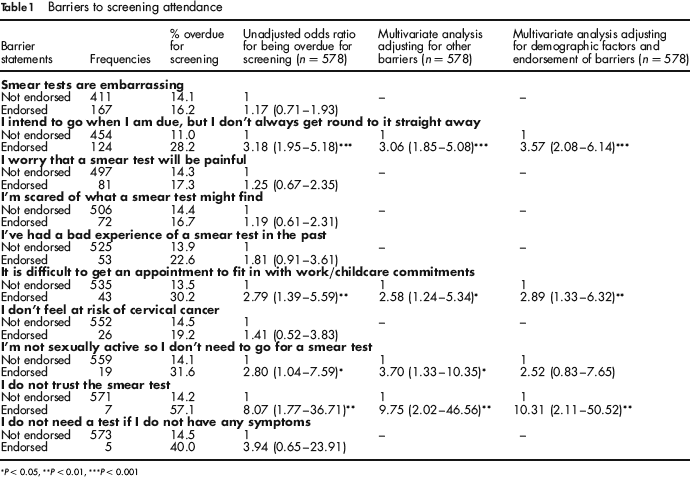
The cervical screening module was introduced with the sentence: ‘Some of the following questions refer to cervical screening, sometimes called the smear or Pap test’. Women were asked to choose from a list of statements the one that best described their cervical screening attendance. They were then asked to look at a list of 13 statements about cervical screening and to indicate all those which they agreed with (see Table 1). The statements were compiled to include a wide range of practical and attitudinal barriers to screening that have been identified in the literature. The order in which the statements were presented was reversed in the two halves of the sample to minimize ordering effects.
Barriers to screening attendance
p < 0.05
p < 0.01
p < 0.001
To explore the idea that screening non-attendance might be associated with more general social disillusionment, we also asked women about their voting behaviour. Each woman was presented with the following question: ‘Thinking about general, local or European elections, which of these statements best describes how often you have voted over the years’ with the response options: (1) I have never voted in any election; (2) I have occasionally voted but usually I don't; (3) I vote in some elections but not others; (4) I usually vote but occasionally I don't; (5) I always vote in every election; (6) I am not eligible to vote in this country. For analysis, we combined data from response options 1 and 2, and options 3 and 4. Those not eligible to vote were excluded from analyses.
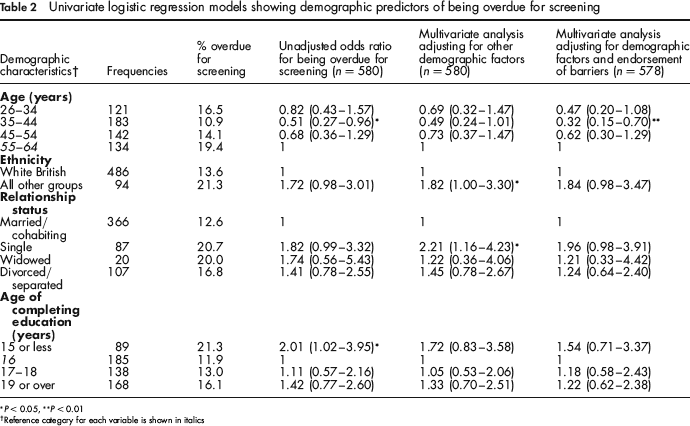
Demographic factors measured in the study included age, age of leaving full-time education, marital/relationship status and ethnic group (see Table 2 for groupings).
Univariate logistic regression models showing demographic predictors of being overdue for screening
p < 0.05
p < 0.01
Reference category for each variable is shown in italics
Analysis
Analyses were carried out using SPSS v14 (Chicago, 111, USA). We used logistic regression models to explore associations between demographic factors, voting behaviour, barriers and screening status. Associations between demographic factors and endorsement of barriers were tested using χ2 tests.
Results
Characteristics of the sample
As shown in Table 2, the majority of the sample was white British (84%) and married or cohabiting (63%), with a good distribution across the age groups (mean age was 44 years). Thirty-two percent of the sample reported leaving full-time education at the age of 16 years, and 29% reported leaving education at the age of 19 years or above. In terms of voting behaviour, 33% of women reported voting in every election, 39% said that they sometimes or usually voted, and 26% reported that they never or only occasionally voted. Just under 2% stated that they were not eligible to vote in the UK.
Overall, 80% of women reported attending regularly for cervical screening, mainly through the National Health Service (77%), but a few had smear tests privately (1%) or outside the UK (2%). About 12% said that although they had attended in the past, it was longer than three years (for women aged 26–49 years) or five years (for women aged 50–64 years) since their last test. A smaller proportion (5%) reported having delayed or missed a test in the past although they had attended recently. Only 15 women (2.6%) reported never having had a smear test. For the purposes of analyses, we compared women who were currently up-to-date with screening (n = 494; 85%), with those who had never had a smear test or were currently overdue for screening (n = 86; 15%)
Endorsement of barriers to screening
Just over 40% of women did not endorse any of the barrier statements. The most frequently endorsed barriers were embarrassment (29%), intending to go when due for a test, but not getting round to it straight away (21%), worrying that smear tests are painful (14%), being scared of what a smear test might find (12%), having a bad experience of a smear test in the past (9%), and difficulty getting an appointment that would fit with work/childcare commitments (7%) (see Table 1). Three statements are not shown in the table as they were endorsed by fewer than five women – ‘I've never heard of smear tests’ (n = 2), ‘I've never been invited to have a smear test’ (n = 3) and ‘I can't have a smear test as I'm not registered with a GP’ (n = 2).
Predictors of screening attendance
Demographic factors
Univariate logistic regression analyses were used to explore demographic predictors of being overdue for screening, using the binary screening outcome described above (see Table 2). Women in the 35–44 year age group were at lower odds of being overdue for screening compared with the 55–64-year-old reference group (P=0.04). Women who left full-time education before the age of 16 were at higher odds of being overdue compared with the reference group who left school at 16 years (P = 0.04). There was a trend towards single women being more likely than married women to be overdue for screening (P = 0.053), and a trend towards lower uptake in non-white British women (P = 0.057).
When age, age of leaving full-time education, ethnic group and marital status were entered into a multivariate logistic regression analysis, the pattern of associations changed slightly (see Table 2). Age group and age of leaving education no longer showed significant associations with uptake, although the P value for the 35–44 year group was close to significant at 0.052. The effects of being from an ethnic minority group (P = 0.05) and being single (P = 0.02) became significant.
Endorsement of barriers
We also examined the relationship between endorsement of barriers and screening attendance using univariate logistic regression analyses (see Table 1). Analyses were not carried out for the barriers that were endorsed by fewer than five women. Women who thought that the test was embarrassing or painful, who reported having a bad experience with screening in the past, being scared of what the test might find, or not feeling at risk of cervical cancer were not at higher odds of being overdue for screening. Being overdue was significantly associated with not getting round to going for screening straight away (P < 0.0001), finding it difficult to arrange a convenient appointment time (P = 0.004), not trusting smear tests (P = 0.007) and not being sexually active (P = 0.04). When these four barriers were entered into a multivariate model, they had significant independent effects (see Table 1).
We used χ2 tests to examine possible associations between endorsement of the four significant barriers and demographic characteristics. ‘I intend to go … but don't always get round to it’ was endorsed more by more non-white (30%) than white British (20%) women (P = 0.04) and by younger (26–34 years: 28%) than older (55–64 years: 8%) women (P < 0.0001). The pattern of association with education was non-linear, with higher endorsement among women who left full-time education at either 16 years or 19+ years than those who left before 16 or at 17–18 years (P = 0.04). There was no association with relationship status. Difficulty arranging a convenient appointment showed no association with ethnic group, education or relationship status, but was more commonly endorsed among younger (26–34 years: 14%) than older (55–64 years: 1%) women (P < 0.0001). Lack of trust in smear tests did not show any demographic associations, although the analyses were under-powered, as very few women endorsed the statement. Endorsing the statement I'm not sexually active so I do not need to go for smear tests’ was more commonly endorsed by women who were widows (20%) than any of the other relationship status groups (2%, 7% and 3% for married, single and divorced/ separated respectively) (P < 0.0001). There were no significant associations with ethnic group or age, but women who left school before age 16 years were more likely to endorse this statement (10%) than women who left at older ages (2%, 1% and 4% for women who left education at age 16, 17–18 and 19+ years respectively) (P < 0.0001).
Demographic factors and barriers
In a final multivariate model (see Tables 1 and 2), age, age of leaving education, ethnic group, marital status and the four barriers showing a significant association with uptake were entered into a logistic regression analysis to identify independent effects. Women aged 35–44 years were less likely than the oldest women to be overdue for screening (P = 0.005) but the other demographic factors did not show significant independent effects in the model. Endorsing the statement ‘I am not sexually active so I don't need to go for a smear test’ no longer had a significant effect in this model, but the other three barriers did (‘I intend to go…but don't always get round to it’ (P < 0.0001); ‘It is difficult to get an appointment…’ (P = 0.008); and ‘I do not trust the smear test’ (P = 0.004)).
Voting behaviour
We used logistic regression models to examine the association between voting behaviour and screening status. Women who reported that they never or only occasionally voted in elections were significantly more likely to be overdue for screening compared with women who always voted (OR: 1.87, 95% CI: 1.05–3.34, P = 0.03). This effect persisted when adjusting for age, ethnic group, marital status and education (OR: 2.07, 95% CI: 1.09–3.92, P = 0.03), and when the four barriers showing significant associations with screening uptake were added to the model (OR: 2.17, 95% CI: 1.12–4.23, P = 0.02).
Discussion
With coverage of cervical cancer screening in England at an all-time low since the UK call-recall system began, this study was timely in exploring predictors of uptake in a population-based sample. We found that although emotional barriers that have been identified in other studies (embarrassment and fear of discomfort) were fairly commonly endorsed, they were not predictive of uptake. Rather, attendance was predicted by more practical barriers including ‘not getting round to it’, difficulty arranging a convenient appointment and by trust in the smear test. Consistent with previous studies, we found some evidence of lower uptake among single women, those from non-white ethnic backgrounds and in less educated women, but these effects disappeared in multivariate analyses, indicating that they were largely explained by barrier endorsement. This is encouraging as these practical barriers are more modifiable than demographic factors.
Our study highlights possible limitations of qualitative studies which ask women to explain why they do not attend for screening.12, 15 In these studies, women often cite negative attributes of the smear test (e.g. it is embarrassing or uncomfortable) as a way of justifying their behaviour. Our findings suggest that actually these negative attitudinal factors may be endorsed equally by women who attend regularly, indicating that they do not provide a true explanation for non-attendance. Psychologists have long known that people are not always able to access their true motivations for behaviour, 16 and more sophisticated methods may be needed to better understand non-attendance.
To our knowledge, this is the first study to test the hypothesis that low uptake could be associated with broader disillusionment, using voting behaviour as a marker. Consistent with the hypothesis, women who reported that they rarely or never voted in elections were at increased odds of being overdue for screening compared with women who always voted. In line with Lancuck et al.'s 11 suggestion, this effect appears to be stronger in younger women. When we stratified the sample by age, we found that never or rarely voting was associated with being overdue for screening in women aged 26–44 years (OR: 3.29, 95% CI: 1.07–10.16), but the effect did not reach significance in the 45–64-year age group (OR: 2.22, 95% CI: 0.99–4.97). Further work is needed to explore this association, and to gain a better understanding of what social disillusionment really means. An alternative explanation for the finding is that both voting and attending for screening require a degree of organization, and women who do not manage to vote because of busy and chaotic lives might also be unlikely to attend for screening.
Strengths and limitations
The study benefited from the use of a population-based sample, recruited using ‘gold-standard’ methods. But although the sample was broadly representative of the general British population, the overall response rate was lower than ideal at 61%, and in addition, 85% of women were up-to-date with screening, which is higher than the nationwide figure of 78.6% 1 and indicates that women who do not attend regularly for screening were under-represented in our sample. It should also be noted that the current study might not have had sufficient statistical power to detect effects of some of the variables, e.g. ethnic group. Although our sample in fact had a slightly lower proportion of people identifying themselves as white British than would be expected from 2001 census data (84% compared with 87%), population-based samples such as this do not allow detailed exploration of ethnic differences. Future research might benefit from using alternative methods (e.g. quota sampling) to recruit larger numbers of ethnic minority participants and explore specific attitudes and barriers across ethnic groups. Finally, cervical screening behaviour was measured by self-report, and women's answers might have been affected by self-presentation and memory biases. 17
Implications
Our findings suggest that overcoming practical barriers may be the most important factor in maximizing uptake of cervical screening. This might include running evening or weekend clinics to allow women with work or childcare commitments to attend at times that are convenient for them, and trying to address public concerns about the screening programme to build public trust. The high endorsement of the statement ‘I intend to go when I am due for a smear but don't always get round to it straight away’ indicates that interventions to help women translate their intentions into actions might be appropriate. Health psychologists have used so-called ‘implementation intentions’, which encourage people to plan how, when and where they will carry out a health-related behaviour, to address this problem of intention translation. One study found that asking women to form an ‘implementation intention’ about making a screening appointment increased levels of attendance among women who intended to go for screening, indicating that this could be a useful approach. 18
Conclusions
Emotional factors such as concern about embarrassment and pain may be less predictive of attendance for cervical screening than has previously been suggested. This is encouraging, and points to the need for interventions aimed at minimizing practical barriers to attendance.
Footnotes
JoW.
JoW, JW and MB designed the study. All the authors contributed to the analysis. JoW and MB wrote the first draft of the paper. All the authors contributed to the final manuscript.