
Abstract
Objective
To investigate the influence of children in the household on the likelihood of reporting cancer screening among adult men and women living in the United States.
Methods
2004–2006 Medical Expenditure Panel Surveys (MEPS) were used to calculate the probability of self-reported cancer screening by number of children for adult men and women with adjustment for age, sex, marital status, race, education, current smoking status, obesity status, health insurance and having a usual health-care provider.
Results
The largest percentage of persons who had cancer screening was among respondents with no children in the household. In multivariate results, the probability of endoscopy was lower for persons with one child (24%) and two or more children (21%) in comparison with persons with no children living in the household (30%). Prostate-specific antigen (PSA) testing was lower among men with one child (17%) and two or more children (14%) in comparison with no children (22%). Pap smears were lower for women with two or more children (50%) but not different for women with one child (55%) in comparison with no children (56%). Mammograms were lower for women with one child (48%) and two or more children (42%) in comparison with no children in the household (55%).
Conclusion
Across several different cancer screening modalities, the probability of screening is lower as the number of children in the household increases. Children may be an additional barrier to screening beyond factors such as socioeconomic status and access to care.
Introduction
Parents may be more likely to screen and maintain a healthy lifestyle because children depend on them for economic and emotional security. For example, a study on smoking cessation found that parents were more likely to quit smoking after having a baby. 10 By staying healthy, the parent is role modelling healthy behaviour and more likely to provide for the child's future needs. Conversely, other studies have found that the stress of parenting may have a deleterious effect on health and wellbeing.11, 12 These studies have argued that although the parenting role comes with enhanced sense of gratification, these positive benefits are cancelled out with the numerous demands of the parenting role, particularly with young children. Therefore, the demands of childcare may prohibit one from prioritizing preventive health screenings, making it less likely for adults living with children to get preventive screening. Given the lack of empirical evidence and the potentially important implications for interventions aimed at improving screening rates through family support,6,9, 13–15 this study investigated the influence of children on cancer screening of adult men and women.
Methods
This study used publicly available data from the Agency for Healthcare Research and Quality. The 2004–2006 Medical Expenditure Panel Surveys (MEPS) are a series of longitudinal surveys that capture a nationally representative sample of individuals, families, their medical providers and employers across the USA. The sampling frame for MEPS is drawn from the preceding year's National Health Interview Survey. In addition to self-reported data from the respondents, MEPS data also include a medical provider component that serves to supplement and verify information provided by respondents in the household component. Further details on MEPS design and content have been published elsewhere. 16 Respondents that were missing information for cancer screening or number of children were excluded from the final analysis.
American Cancer Society guidelines were used to determine age categories for cancer screening. 17 Male and female respondents 50 years of age and older reported if they had ever had a sigmoidoscopy or colonoscopy. Men 40 and older reported if they had had a prostate-specific antigen (PSA) test in the past year. Pap smear test in the past year was asked of women 18 years of age and older. Mammogram in the past year was asked of women aged 40 and older. In MEPS, the question for cancer test was presented as whether the respondent had been administered the test in a given time period. Therefore, it was not possible to ascertain whether the cancer tests were performed for screening or for diagnostic purposes. The presence of children 18 years of age or younger in the household was originally coded in the survey as a continuous variable ranging from 0 to 11. However, this variable was highly skewed so it was recoded as categorical variable of none, one child, and two or more children. Control variables included age in years, female versus male sex, married versus unmarried marital status, white versus non-white race, years of education, current smoking versus non-smoker, obesity classified as a body mass index of 30 kg/m2, having any health insurance versus no health insurance, and reporting a usual source of care versus reporting no usual source of care.
All analyses were performed with STATA version 10.1 SE (StataCorp, College Station, TX, USA) to adjust for the survey weights, population sampling units and strata. Descriptive statistics for all study variables are presented by number of children. Multivariate models use random effects logistic regression and adjust for year of interview, age, education, race, marital status, health insurance, usual provider, obesity and smoking. The estimates for cancer screening from the multivariate logistic regression models were then converted into probabilities and presented by the number of children in the household.
Results
Table 1 presents descriptive statistics for all of the study variables. Overall, 60% of respondents reported no children aged 18 years or younger living in the household, 17% reported one child and 23% reported two or more children in the house-hold. Over half of respondents reported a Pap smear (56%) and mammogram (56%), while less than half reported a PSA test (40%) and endoscopy (49%). In comparison with persons with no children in the household, persons with any children in the household were less likely to have reported cancer screening within recommended guidelines. For example, 89% of persons with no children in the household reported an endoscopy, 82% reported a PSA test, 74% reported a mammogram and 55% reported a Pap smear. In contrast, 25% of respondents with two or more children in the household reported having a Pap smear within the past year.
Weighted percentages by number of children living in the household: Medical Expenditure Panel Surveys (MEPS), 2004–2006
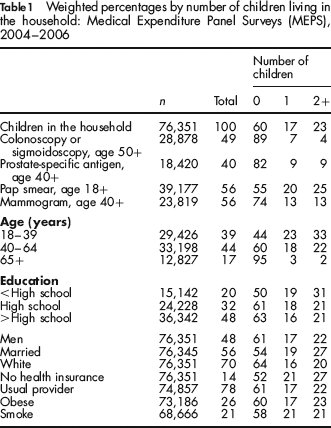
Table 2 presents the multivariate adjusted odds ratios of cancer screening. To determine whether the association between endoscopy and number of children varied by gender, an interaction variable was created (gender × number of children). This variable was then entered in a multivariate logistic regression. The interaction effect was not statistically significant, suggesting that the association between endoscopy and number of children was similar for men and women. In comparison with persons with no children living in the household, the likelihood of endoscopy was lower for persons with one child (0.72) and two or more children (OR = 0.62). PSA testing was loweramong men with one child (OR = 0.72) and two or more children (OR = 0.57) in comparison with no children. Pap smears were lower for women with two or more children (OR = 0.78) but not different for women with one child. Mammograms were lower for women with one child (OR = 0.75) and two or more children (OR = 0.60) in the household in comparison with no children.
Multivariate odds ratios (95% confidence interval) of cancer screening
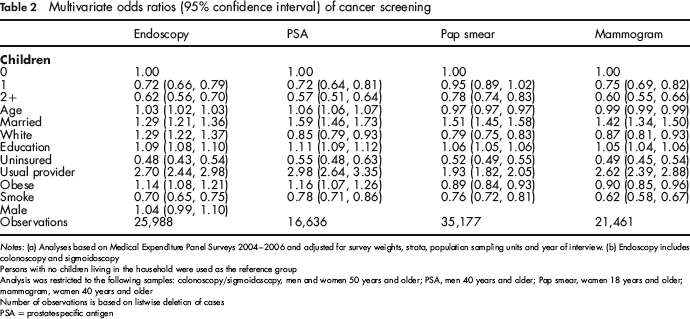
Notes: (a) Analyses based on Medical Expenditure Panel Surveys 2004–2006 and adjusted for survey weights, strata, population sampling units and year of interview, (b) Endoscopy includes colonoscopy and sigmoidoscopy
Persons with no children living in the household were used as the reference group
Analysis was restricted to the following samples: colonoscopy/sigmoidoscopy, men and women 50 years and older; PSA, men 40 years and older; Pap smear, women 18 years and older; mammogram, women 40 years and older
Number of observations is based on listwise deletion of cases
PSA = prostate-specific antigen
Table 3 shows the multivariate adjusted probabilities of cancer screening by number of children in the household. These percentages are adjusted for the mean levels of age, sex, marital status, education, health insurance, obesity, smoking and access to a usual provider. Across several different screening modalities, the probability of screening was lower as the number of children in the household increased. For example, 55% of women over the age of 39 years with no children living in the household reported a mammogram, but only 42% of women with two or more children reported a mammogram after accounting for other factors.
Predicted probabilities (95% CI)∗ of cancer screening by number of children in the household: Medical Expenditure Panel Surveys 2004–2006
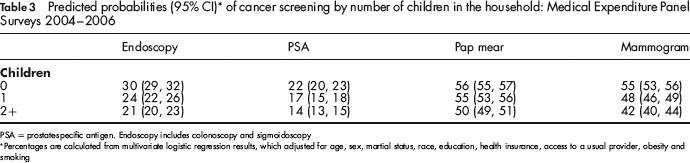
PSA = prostate-specific antigen. Endoscopy includes colonoscopy and sigmoidoscopy
*Percentages are calculated from multivariate logistic regression results, which adjusted for age, sex, martial status, race, education, health insurance, access to a usual provider, obesity and smoking
Discussion
This study set out to ascertain differences in cancer screening by number of children. No previous study had examined the influence of children on cancer screening. The results suggest that the presence of children under 18 years of age in the household is associated with a lower likelihood of cancer screening. For most types of cancer tests, any children in the household reduced the odds of cancer screening. However, there was no statistically significant difference for Pap smear when comparing women with one child in the household with women without children in the household after accounting for other factors.
These findings suggest support for the hypothesis that children increase the opportunity cost of screening. Parents may have less time to get screened, and probably prioritize the needs of the children over their own health. Many forms of cancer screening require significant time commitment, particularly endoscopy, which requires time at home for bowel preparation and time recuperating from the drugs after the procedure. With more children comes less disposable income available for health tests. Given the high cost of childcare, parents may be less willing to spend more money for this service for the purpose of screening. Even many forms of health insurance require a copayment for testing, which may not be seen as a necessary expense in larger families that have other immediate needs such as food and clothing. Further explanation for the finding that children may lower screening rates comes from recent evidence suggesting that the numerous demands and stressors associated with being a parent overwhelm the positive, emotional rewards, resulting in a net loss of wellbeing.11, 12
It should be noted that the findings from this study should be viewed as preliminary and in need of replication. The principal limitation of this study was that data for cancer testing were self-reported and could not clearly identify whether the purpose of the test was for screening or diagnosis. However, most mammograms, PSA and Pap smears performed in the community are usually for the purpose of screening rather than diagnosis. 18 Therefore, the assumption was made that most of these tests were performed for the purpose of screening, but the results should be viewed cautiously in light of this limitation. Another limitation of the study is that MEPS does not provide the age of the children in the household. The barriers for screening would likely vary significantly depending on the age of the child. Children attending school present less of a barrier than children who are not yet in school full time. Furthermore, given that a criterion for inclusion in this study was that children needed to be less than 18 years of age and living in the household, then persons with more than one child in the household were more likely to have younger children in the household than parents with only one child.
Conclusion
Preliminary evidence suggests that children living in the household may lower the likelihood of cancer screening for adults. Future studies should attempt to replicate the finding that children may be a barrier to screening. Although this study was not able to elucidate the reasons that adults with children living at home are less likely to be screened, we might speculate that screening could be improved by reducing the cost of the tests, lowering the cost of childcare or by decreasing the time and effort needed to schedule and travel for screening.