
Abstract
Objectives
To assess the value of ductus venosus blood flow (expressed as pulsatility index, DVPI) in antenatal Down's syndrome screening when used with the Combined and Integrated tests.
Methods
DVPI measurements between 10 and 13 weeks’ gestation in 66 Down's syndrome and 7184 unaffected pregnancies were collected from women attending the Hospital Clinic, Barcelona, for antenatal care from 1999 to 2007 and combined with the Serum Urine and Ultrasound Screening Study (SURUSS) data to model screening performance, safety and cost-effectiveness of the screening tests with and without DVPI.
Results
The median DVPI multiple of the normal median in Down's syndrome pregnancies was 1.55 (95% CI 1.36–1.73). As a single screening marker without using maternal age, DVPI has a 62% detection rate for a 5% false-positive rate. At a 90% detection rate (first trimester measurements at 11 weeks’ gestation) the addition of DVPI reduced the false-positive rate of the Combined test from 8.5% to 4.6% and the Integrated test from 2.0% to 1.1%, with a corresponding reduction in fetal losses from diagnostic procedures. There was no material loss of cost-effectiveness.
Conclusion
Addition of DVPI measurements to the Combined and Integrated tests substantially improves the efficacy and safety of antenatal Down's syndrome screening.
Introduction

A typical example of DVPI in a pregnancy without Down's syndrome measured around 10–13 weeks’ gestation is
and a typical example of DVPI in a Down's syndrome pregnancy, where flow of blood is reversed is
Because DVPI is a ratio of two velocities, the index is unitless.
DVPI has previously been assessed together with the late first trimester Combined test (measuring nuchal translucency [NT], pregnancy-associated plasma protein A [PAPP-A] and free β human chorionic gonadotrophin [free β-hCG], at about 10–13 weeks’ gestation). 6 We here use a larger dataset on DVPI measurements (which include the previous data 6 ) combined with results from the Serum, Urine and Ultrasound Screening Study (SURUSS), 7 to estimate the effect of including DVPI with the first trimester Combined test and with the Integrated test (measurements of NT and PAPP-A in the late first trimester integrated with measurements of alphafetoprotein, unconjugated oestriol [uE3], free β-hCG and inhibin-A from the early second trimester [15–20 weeks]). We also present a cost and safety analysis, with and without a DVPI measurement added to these tests.
Methods
Two patient samples were used to determine the distribution of DV measurements in the first trimester: (i) women attending for routine antenatal care in the Hospital Clinic, Barcelona between October 1999 and December 2006 who had the Combined test (n = 6940) and (ii) women who had an ultrasound examination immediately before chorionic villus sampling (CVS) in the period October 1999–December 2007 (n = 310). DV blood flow was measured at the time of NT measurement at 10–13 weeks. Some of these data (51%; pregnancies seen between 1999 and 2002) were included in a previous publication. 6 None of the women had an Integrated test and although Combined tests were performed the marker values were not used in this study other than to estimate correlation coefficients between DVPI and PAPP-A, free β-hCG and NT.
DV was assessed by a transabdominal ultrasound examination (Eccocee SSA and Power-Vision 400, Toshiba Medical Systems; Voluson PRO, General Electrics Healthcare). Eighteen ultrasonographers performed the measurements. The image of the fetus was captured in an almost sagittal view, the fetus lying in an oblique position so that the DV is seen as vertical as possible on the screen (low insonation angle). Preferably, the same magnification was used as for NT measurement, so only the fetal trunk was included in the image. Colour Doppler was applied once the fetus was resting quietly in the desired position. Pulsed Doppler sample volume of 1 mm was positioned on the ithsmic portion of the DV to obtain homogenous wave forms.
If reverse blood flow was observed in the DV, a second examination was performed at least one minute later, and the result only accepted if the two were consistent. Care was taken to avoid confusion from waveforms of neighbouring veins. For example, if signals from the inferior vena cava or suprahepatic veins, physiologically displaying reverse flow, were superimposed on that from the DV, it could mistakenly be interpreted as reverse DV blood flow and lead to a false-positive result (see below). Conversely if the umbilical vein signal was superimposed, the normal flow in the vein superimposing the DV could mask an absent or reversed DV flow and so generate a false-negative result. DV blood flow was assessed as a quantitative marker, the DVPI calculated using a programme within the equipment. DV measurements were not obtained in 3.3% of pregnancies. Details of the outcome of pregnancy were obtained by telephone if the pregnancy was not delivered at the Hospital Clinic, Barcelona. If a mother could not be reached, the outcome was obtained from the attending obstetrician. Follow-up was obtained in 97.4% of pregnancies. Unaffected pregnancies were defined as pregnancies without Down's syndrome or other chromosomal abnormalities.
Screening performance was estimated using Monte Carlo simulation. 8 Briefly, 500,000 Down's syndrome and 500,000 unaffected hypothetical pregnancies, each with a set of marker values expressed as multiples of the normal median (MoM) were simulated from the multivariate Gaussian distributions of MoM values in Down's syndrome and in unaffected pregnancies. The distributions were defined by the parameters (means, standard deviations, correlation coefficients and truncation limits) for NT and the serum markers estimated in a larger prospective study (SURUSS)7,9–11 and the parameters for DVPI estimated in the current study.
As with the other screening markers, DVPI were converted into MoM values. Probability plots were used to assess the fit of DVPI MoM values in Down's syndrome and unaffected pregnancies to Gaussian distributions (a reasonably straight line indicating a good fit). The distributions of DVPI in Down's syndrome and unaffected pregnancies were described using the median MoM values (rather than the means to prevent the influence of outlying values) and standard deviations (calculated using a regression between the log DVPI MoM values and corresponding centile within the 10th–90th centile range). Correlations between DVPI and NT and between DVPI and the first trimester serum markers were estimated using the measurements obtained in Barcelona, excluding observations that were greater than 3.5 standard deviations from the median. Truncation limits for DVPI MoM values were assessed from inspection of the probability plots in Down's syndrome pregnancies and in unaffected pregnancies.
Each simulated pregnancy was assigned a maternal age based on the maternal age distribution of maternities in England and Wales 1996–1998 12 and the maternal age-specific odds of an affected live birth.11–13,14 For each simulated pregnancy, the predicted risk of having a pregnancy with Down's syndrome was calculated by multiplying the maternal age-specific odds of having an affected live birth,11,13,14 adjusted to early mid-trimester (by multiplying by 1/0.77 to allow for the general fetal loss in Down's syndrome pregnancies from this time in pregnancy until term 15 ), by the likelihood ratio (for a given set of marker values) obtained from the overlapping multivariate Gaussian distributions of marker levels in affected and unaffected pregnancies. Each simulated pregnancy was classified as screen positive if the risk estimate was greater than or equal to a specified cut-off level.
Estimates of screening performance were specified as the detection rate (the proportion of affected pregnancies with a positive result) for a specified false-positive rate (the proportion of unaffected pregnancies with a positive result) and as the false-positive rate for a specified detection rate. Estimates of screening performance were calculated, with and without the addition of DVPI to (i) the Combined test and (ii) the Integrated test.
The safety of each screening approach with and without the addition of DVPI was determined as (i) the number of procedure-related unaffected fetal losses (due to amniocentesis or CVS) per 100,000 women screened and (ii) the number of Down's syndrome pregnancies detected for each procedure related unaffected fetal loss. The fetal loss rate from amniocentesis or CVS was taken as 0.9%, 16 with uptake taken as 80% for unaffected pregnancies and 90% for Down's syndrome pregnancies, higher due to women with Down's syndrome pregnancies having higher risk estimates. 7
The cost of each screening method was expressed as (i) the cost of screening 100,000 women and (ii) the cost per Down's syndrome pregnancy detected. Costs were those in the UK public sector and included cost of ultrasound scan, reagent and non-reagent laboratory costs, service costs (computer-assisted test interpretation and administration), the cost of a diagnostic test, termination of pregnancy, medical evacuation of products of conception and delivery. 7 The cost of an ultrasound scan of both NT and DVPI was taken to be 50% greater than the cost of an ultrasound scan of NT alone.
Results
DVPI results were available in 66 Down's syndrome pregnancies and 7184 consecutive unaffected pregnancies screened between 10 + 0 and 13 + 6 weeks of gestation. Mean maternal age was 32 years and mean gestational age when the ultrasound was performed was 12 weeks three days.
Figure 1 shows the DVPI values in Down's syndrome pregnancies compared with the median 5th and 95th centiles in unaffected pregnancies according to gestational age. In unaffected pregnancies the median DVPI was 1.1. The 95th centile in unaffected pregnancies was 1.5. Over half (58%) of Down's syndrome pregnancies had a DVPI value above this. Only three Down's syndrome pregnancies had a DVPI value below the unaffected median. The median DVPI in Down's syndrome pregnancies was 1.71. As previously found, there was no statistically significant association between DVPI in unaffected pregnancies and gestational age,
6
so gestation-specific normal medians were not needed to calculate MoM values; DVPI values were converted into MoM values by dividing by the median of 1.1 in unaffected pregnancies. The resulting median MoM in Down's syndrome pregnanies was 1.55 (95% CI 1.36–1.73). The median DVPI was the same (to one decimal place) for women attending for routine antenatal care as for women who had an ultrasound examination immediately before CVS.
DVPI in 66 Down's syndrome pregnancies from 10–13 completed weeks gestation with the median, 5th and 95th centiles in unaffected pregnancies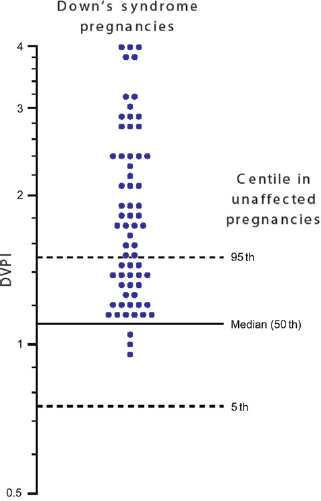
Figure 2 shows the probability plots of DVPI MoM values in Down's syndrome and unaffected pregnancies between 10 + 0 and 13 + 6 weeks’ gestation. The range of values over which the DVPI MoM values are log-Gaussian (shown by the linear portions of the two plots in Figure 2) is relatively narrow, hence the truncation limits of 0.9 and 1.5 used in the subsequent analyses used to estimate screening performance. The standard deviations of the log10 MoM values in Down's syndrome and in unaffected pregnancies (calculated by a regression of the points on the probability plots between the 10th and 90th centiles) were 0.1955 and 0.0791, respectively, relatively small standard deviations compared with other Down's syndrome screening markers. In unaffected pregnancies there was a small statistically significant increase in the standard deviation with gestational age; however, it had negligible effect on screening performance or risk estimate so the overall standard deviation (0.0791) was used in further analyses.
Probability plot of DVPI (MoM) in Down's syndrome and in unaffected pregnancies (with dashed lines at the truncation limits, 0.9–1.5). DVPI, ductus venosus pulsality index; MoM, multiples of the normal median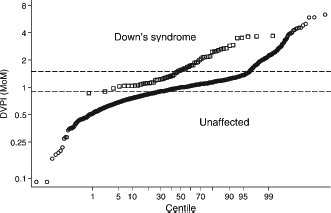
Figure 3 shows the overlapping Gaussian distributions of DVPI in Down's syndrome and unaffected pregnancies together with the truncation limits. As a single screening marker without using maternal age, DVPI has a detection rate of 62% for a 5% false-positive rate, a similar performance to NT alone.
Relative frequency distributions of DVPI in Down's syndrome and in unaffected pregnancies (with dashed vertical lines at the truncation limits, 0.9–1.5). DVPI, ductus venosus pulsality index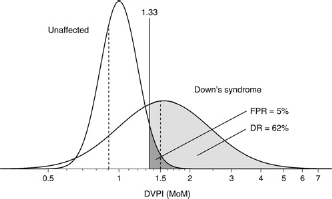
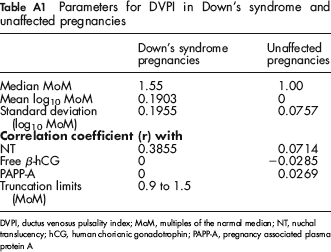
Figure 4 shows the NT MoM values plotted against the DVPI MoM value for each pregnancy in Down's syndrome (left part of the figure) and in unaffected pregnancies (right part). There was a moderate association between the two markers in Down's syndrome pregnancies with a correlation coefficient, r, of 0.3855 (P < 0.01), which was used in subsequent screening performance, cost, and safety analyses, but there was no statistically significiant correlation between DVPI and free β-hCG or PAPP-A, so for both r = 0 was used in subsequent analyses. In unaffected pregnancies there was a statistically significant association between DVPI and NT, free β-hCG and PAPP-A. The correlation coefficients were small (r = 0.0714, −0.0285 and 0.0269, respectively) but were nevertheless included in further analyses. While this study provides no information on any correlation between DVPI and second trimester serum markers the little or no correlation between DVPI and the first trimester serum markers indicated that it was reasonable to assume no correlation with the second trimester serum markers. The relevant distribution parameters needed to model screening performance and estimate the risk of a Down's syndrome pregnancy are given in Appendix Table A1.
DVPI (MoM) plotted against NT (MoM) in (a) Down's syndrome pregnancies and in (b) unaffected pregnancies. DVPI, ductus venosus pulsality index; MoM, multiples of the normal median; NT, nuchal translucency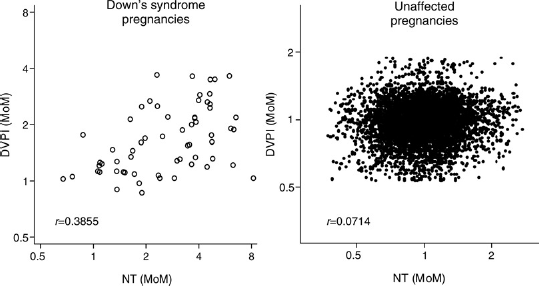
Table 1 shows the estimated screening performance of the two tests (Combined and Integrated) considered with and without the addition of a DVPI measurement. Adding DVPI reduced the false-positive rate of both tests. At an 85% detection rate the false-positive rate is more than halved (for example, from 4.4% to 2.1% for the Combined test at 11 completed weeks), approximately halved at a 90% detection rate (for example, from 2.0% to 1.1% for the Integrated test with first trimester markers measured at 11 completed weeks) and reduced by about 40% at a 95% detection rate (for example, from 6.1% to 3.5% for the Integrated test). Screening performance results were not estimated for 10 completed weeks’ gestation because of a lack of NT measurements in Down's syndrome pregnancies before 11 weeks in the literature.
Screening performance of the Combined test and Integrated test with and without DVPI
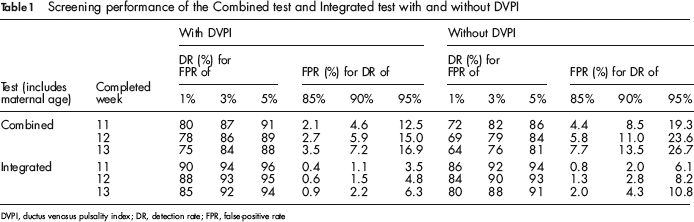
DVPI, ductus venosus pulsality index; DR, detection rate; FPR, false-positive rate
Table 2 shows the estimated screening performance of the two tests considered with and without a DVPI measurement according to risk cut-off. The odds of being affected given a positive screening result (OAPR) is also shown. At each specified risk cut-off the inclusion of DVPI in each of the two tests increases the detection rate, reduces the false-positive rate and nearly doubles the OAPR. For example, at a 1 in 200 mid-trimester risk cut-off (approximately 1 in 250 at term) the Integrated test with the addition of DVPI and with first trimester markers measured at 11 completed weeks has a detection rate of 91%, a false-positive rate of 1.2% and the OAPR is 1:6. The corresponding figures for the Integrated test without the addition of DVPI are 90%, 2.1% and 1:10.
Screening performance of the Combined test and Integrated test with and without DVPI, according to risk cut-off (at mid-trimester)
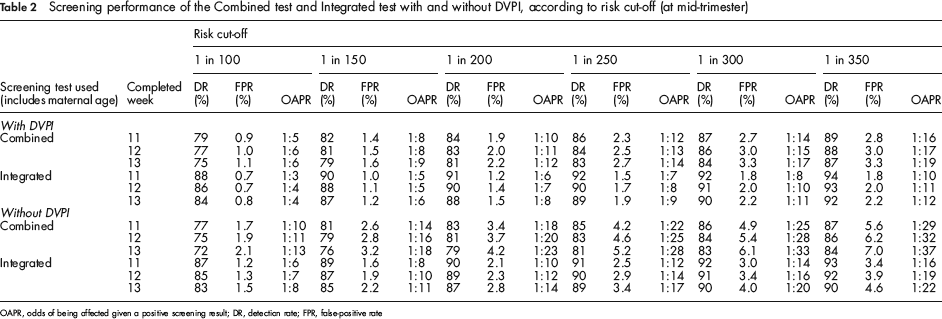
OAPR, odds of being affected given a positive screening result; DR, detection rate; FPR, false-positive rate
Table 3 shows the safety of screening based on the two tests with and without the addition of DVPI. With the addition of a DVPI measurement the number of procedure related unaffected fetal losses is between about two-thirds and one-half the number when DVPI is not included. For example, at a 95% detection rate, with markers measured at 11 completed weeks, there are 14 procedure related unaffected fetal losses per 100,000 women screened with the Integrated test. With the addition of DVPI this falls to eight fetal losses. The number of Down's syndrome pregnancies detected for each procedure related fetal loss increases from 13 to 23.
Safety of screening and diagnosis based on the Combined test and Integrated test, with and without the addition of DVPI, for specified detection rates
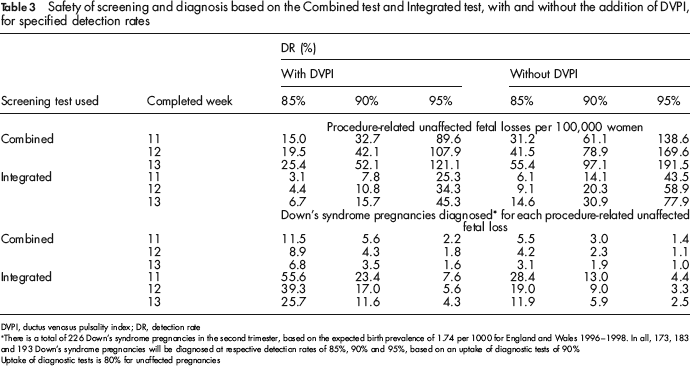
DVPI, ductus venosus pulsality index; DR, detection rate
There is a total of 226 Down's syndrome pregnancies in the second trimester, based on the expected birth prevalence of 1.74 per 1000 for England and Wales 1996–1998. In all, 173, 183 and 193 Down's syndrome pregnancies will be diagnosed at respective detection rates of 85%, 90% and 95%, based on an uptake of diagnostic tests of 90%
Uptake of diagnostic tests is 80% for unaffected pregnancies
Table 4 shows the cost of screening programmes at specified detection rates according to the three tests with and without the addition of a DVPI measurement. The cost of programmes based on the Combined test are reduced with the addition of DVPI. For example, at a 90% detection rate the programme costs decrease from £3.6 million to £2.9 million per 100,000 women screened, and from £17,800 to £14,200 per Down's syndrome pregnancy diagnosed because fewer invasive diagnostic tests are needed to achieve the same detection rate. There is little effect on the programme cost with screening based on the Integrated test with or without the additon of DVPI.
Cost of screening (including diagnosis and termination of pregnancy) using the Combined test and Integrated test, with and without the addition of DVPI, for specified detection rates
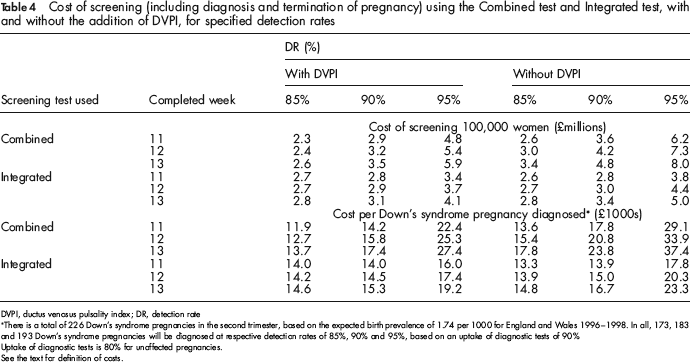
DVPI, ductus venosus pulsality index; DR, detection rate
There is a total of 226 Down's syndrome pregnancies in the second trimester, based on the expected birth prevalence of 1.74 per 1000 for England and Wales 1996–1998. In all, 173, 183 and 193 Down's syndrome pregnancies will be diagnosed at respective detection rates of 85%, 90% and 95%, based on an uptake of diagnostic tests of 90%
Uptake of diagnostic tests is 80% for unaffected pregnancies.
See the text for definition of costs.
Discussion
The use of DVPI as an additional marker as part of first trimester or Integrated screening improves screening performance, reducing the false-positive rate for a given detection rate by about one-half. For example, the Integrated test with a DVPI measurement can achieve a 90% detection rate for a 1.1% false-positive rate instead of 2.0% without a DVPI measurement. The extra cost of performing the DVPI measurement is offset by the reduced number of invasive diagnostic tests needed to achieve a given detection rate, so improving safety without an increase in overall costs per Down's syndrome pregnancy diagnosed.
This study combined data from the screening programme in Barcelona with those from SURUSS. 7 This was necessary because the data did not include second trimester markers and hence were incomplete with respect to the markers and marker parameters needed for the assessment of DVPI with Integrated screening. It was also desirable to use the SURUSS data because they are observational until the completion of second trimester screening, so allowing the valid comparison of first and second trimester tests, without bias arising from the fetal loss of Down's syndrome pregnancies between the late first trimester and early second trimester.
The measurement of DVPI requires Doppler ultrasound equipment and appropriate skill and training. Most modern machines used for NT measurement include colour and pulsed Doppler facilities. The safety of Doppler ultrasound is always an issue that warrants attention. No harm has been linked to Doppler ultrasound but on grounds of prudence the procedure was avoided before 10 weeks’ gestation. Also, pulsed Doppler was applied for no more than a few seconds only in each pregnancy, once the fetus was in an appropriate position. Our results are based on DVPI measurement performed at the same examination as the NT measurement and in experienced hands would take an extra few minutes, so it is reasonable to allocate, as we did in our cost analysis, a marginal cost of performing the DVPI at 50% greater than the cost of the NT measurement. As with NT measurement, the main time issue is waiting for the fetus to adopt the appropriate position and to remain still. A recent study showed that sonographers experienced in NT measurement require an average of 80 examinations before they could successfully assess a DV, 17 a similar number of scans needed to acquire completed NT measurement. 18 In centres where this evaluation can be performed there is a strong case for introducing it into routine screening practice.
DV blood flow has been used as a categorical variable (normal/abnormal) by several groups.2,17,19 We also considered the use of DV blood flow recorded as a categorical variable in which reversed or absent end diastolic blood flow in the DV was a positive result, but otherwise the test was negative. This was a useful discriminatory test on its own, with a 49% detection rate and a 2.8% false-positive rate, but not as useful as DVPI, which had a detection rate of 58% for the same 2.8% false-positive rate. It also offered less improvement than DVPI when added to the two tests considered here. For example, as a categorical variable it reduced the Integrated test false-positive rate from 2.0% to 1.5% at a 90% detection rate, but as a continuous variable (DVPI MoM value) it reduced the false-positive rate to 1.1%. The use of DV blood flow has been suggested as a test in pregnancies with intermediate risk 3 but if it can be measured routinely it will yield a higher screening performance, particularly when part of an Integrated test.
We have given the distribution parameters that will allow the incorporation of DVPI measurement in screening based on first trimester Combined tests and Integrated testing using first and second trimester markers. This will enable screening centres to carry out pilot projects adding DVPI to the markers currently used in their screening tests.
Footnotes
APPENDIX
Parameters for DVPI in Down's syndrome and unaffected pregnancies
| Down's syndrome pregnancies | Unaffected pregnancies | |
|---|---|---|
| Median MoM | 1.55 | 1.00 |
| Mean log10 MoM | 0.1903 | 0 |
| Standara deviation (log10 MoM) | 0.1955 | 0.0757 |
|
|
||
| NT | 0.3855 | 0.0714 |
| Free β-hCG | 0 | –0.0285 |
| PAPP-A | 0 | 0.0269 |
| Truncation limits (MoM) | 0.9 to 1.5 | |
DVPI, ductus venosus pulsality index; MoM, multiples of the normal median; NT, nuchal translucency; hCG, human chorionic gonadotropin; PAPP-A, pregnancy associated plasma protein A