
Abstract
Objectives
To examine the psychological impact of being assigned to colonoscopic surveillance following detection of adenomatous polyps at flexible sigmoidoscopy (FS) screening.
Setting
Participants invited for screening in 12 of the 14 study centres in the UK FS Trial.
Methods
A postal survey following FS screening assessed bowel cancer worry, psychological distress, generalized anxiety, bowel symptoms, general practitioner (GP) visits, positive emotional consequences of screening, and reassurance among people with no polyps (n = 26,573), lower-risk polyps removed at FS (n = 7401) and higher-risk polyps who underwent colonoscopy and were either assigned to colonoscopic surveillance (n = 1543) or discharged (n = 183). A sub-sample (n = 6389) also completed a questionnaire prior to screening attendance that measured bowel cancer worry, generalized anxiety, bowel symptoms and GP visits, making it possible to examine longitudinal changes in this group.
Results
People offered surveillance reported lower psychological distress and anxiety than those with either no polyps or lower-risk polyps. The surveillance group also reported more positive emotional benefits of screening than the other outcome groups. Post-screening bowel cancer worry and bowel symptoms were higher in people assigned to surveillance, but both declined over time, reaching levels observed in either one or both of the other two groups found to have polyps, suggesting these results were a consequence of polyp detection rather than surveillance per se. Few differences were observed between the group assigned surveillance and the group discharged following colonoscopy.
Conclusion
The results of the current study are broadly reassuring and indicate that referral for colonoscopic surveillance is not associated with adverse psychological consequences.
Introduction
There has been little evidence of adverse psychological effects among the screened population as a whole for either FOBT, 12 FS, 13 or colonoscopy. 14 Among people with a positive FOBT result, there are also broadly reassuring results: a large UK population-based study found no differences in anxiety between people with normal or abnormal FOBT results eight months after their invitation to complete the test, 15 and no short-term impact on quality of life was observed as a result of detection of adenomatous polyps in a small study of colonoscopy screening. 14 Similarly, a Norweigan study found no differences on measures of anxiety, depression or general wellbeing, either immediately after screening or 17 months later, 13 with the exception of slightly poorer wellbeing at three months among those with polyps, but this difference had disappeared by 17 months. The authors attributed their reassuring results to clinicians’ efforts to explain the significance of polyps, which they believed had attenuated any negative impact. In the UK FS Trial, 16 individuals found to have higher-risk (i.e. large or numerous) polyps were referred for colonoscopy, whereas those with lower-risk polyps had them removed during FS and were discharged. No adverse effects were found in those who had polyps detected using measures of general anxiety or specific worry about bowel cancer, regardless of whether they had been sent for a colonoscopy, 17 but this study did not distinguish between people who were discharged following colonoscopy or recommended to have colonoscopic surveillance.
Surveillance can create a sense of being cared for, along with the opportunity to be reassured by an endoscopist about any bowel cancer worries, but on the negative side colonoscopy is widely seen as uncomfortable and embarrassing, 18 and while the anxiolytic effects of a single colonoscopy return to normal soon after the procedure, regular screening might be a reminder of cancer risks. The limited research conducted to date suggests that colonoscopic surveillance is well-tolerated. Liljegren et al. 19 surveyed people identified as having a higher than average risk of colorectal cancer (based on genetic mutation status or family history) up to 10 years after clinic referral, when they had received up to 12 colonoscopies. Perceived benefit of colonoscopy was higher among those who recalled having had a polyp removed but was unrelated to the number of colonoscopies received. Depression scores were lower than population norms, and anxiety levels were no different from population norms in the sample as a whole, although men had significantly raised anxiety. Cancer-specific worries, though, were not assessed.
The present study evaluated the psychological impact of being told that colonoscopy surveillance was required following the detection of adenomas by comparing patients undergoing FS screening who had one of four different outcomes: (i) no polyps detected, (ii) lower-risk polyps removed at FS, (iii) higher-risk polyps with referral to colonoscopy followed by discharge from follow-up or (iv) higher-risk polyps with referral to colonoscopy who were then recommended for colonoscopic surveillance. Previous research has suggested that the adverse consequences of screening are more likely to be detected using specific rather than general measures of psychological impact. 20 Consequently it was hypothesized that any adverse effects of surveillance colonoscopy would be stronger for bowel cancer worry compared with a general measure of psychological distress. It was also hypothesized, in line with the findings of Liljegren et al., 19 that the perceived positive consequences of screening would be greater among people who had had a polyp removed, and hence would be higher in those assigned to colonoscopic surveillance compared with the no polyps group, with equivalent levels observed across all groups found to have polyps.
Patients and Methods
Sample
Participants were men and women aged 55–64, at average risk of getting colorectal cancer, invited for screening in 12 of the 14 study centres in the UK FS Trial. 16 Exclusion criteria for the trial were: inability to provide consent; personal history of colorectal cancer, adenomas or inflammatory bowel disease; a strong family history of colorectal cancer (i.e. 2 or more close relatives affected); severe or terminal disease with a life-expectancy of less than five years; presence of a temporary health problem that would have prevented them from having the test; and sigmoidoscopy or colonoscopy within the previous three years. Those eligible for inclusion in the trial were written to by their general practitioner (GP) with an information leaflet on colorectal cancer and FS screening and were asked whether, if invited, they would accept the offer of screening. The information leaflet described the aims of FS screening as the detection and removal of premalignant polyps. Respondents who replied saying they were interested in screening were randomly allocated to screening or usual care. 16 Data from the pilot and first study centre were excluded from the analyses because different postscreening questionnaires were used.
In the FS Trial, individuals with 1–2 small tubular adenomas were considered Tower risk’ and were not offered colonoscopy following polypectomy at FS, while those with more numerous or advanced adenomas were offered colonoscopy. The majority of these individuals were offered surveillance colonoscopy according to a prescribed protocol, similar to the British Society of Gastroenterology guidelines for the management of ‘higher-risk’ cases. 10 Outcome data were available for 35,891 individuals. Of these, 26,573 were found to have no polyps, 7401 had lower-risk polyps, 1543 had higher-risk polyps and were assigned to colonoscopic surveillance, and 183 had higher-risk polyps but were discharged following colonoscopy. In addition, 62 were considered higher-risk but their colonoscopy was not carried out for a variety of reasons (e.g. they were too ill or did not want to undergo the procedure). A further six were referred straight to surgery, and 123 were diagnosed with cancer. These 191 were excluded from the present analysis leaving a total n of 35,700.
Participants were sent a detailed questionnaire 3–6 months after screening, by which time they had been told whether or not they needed colonoscopic surveillance. The response rate to this questionnaire was 90% (see Figure 1). Completion of the postscreening questionnaire was higher among women, older people and people with lower levels of socioeconomic deprivation.
Flowchart showing randomization and study attrition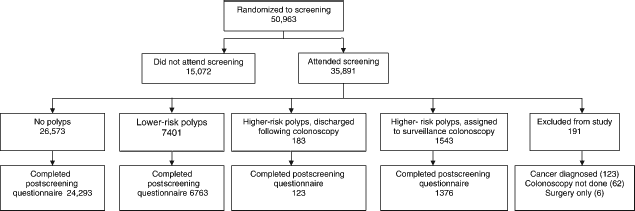
A sub-sample (n = 6389) had also completed a detailed questionnaire prior to screening attendance making it possible to compare pre- and postscreening results in this group. Because of the smaller group sizes for these analyses, there were only 20 individuals who were discharged following their colonoscopy so they were excluded from the longitudinal analyses.
Measures
Demographic variables: Date of birth, gender and postcode data were supplied by GP Practice databases. Age at the time of screening was calculated using date of birth and date of FS screen (recorded by the screening centre). Socioeconomic deprivation was indexed by converting postcode data into Townsend Index scores (an established indicator of area-based socioeconomic deprivation) for all centres except Glasgow.
Primary outcome variables
Bowel cancer worry was assessed before and after screening with the question: ‘How worried are you about getting bowel cancer’ (response options on a 4-point Likert scale: ‘not worried at all, a bit worried, quite worried, very worried’). This has been used in previous studies of breast cancer screening and in the pilot centres of the FS trial. 21 Higher scores indicate higher worry.
Psychological distress was measured postscreening using the 12-item version of the General Health Questionnaire (GHQ-12). 22 This assesses how people have felt in the preceding three months, with a 4-item response scale ‘Better/more than usual, same as usual, less than usual, much less than usual’. Responses were scored 0–3 and were summed to produce a scale from 0 to 36, with higher scores indicating greater distress.
Positive psychological consequences of screening were assessed postscreening using three items from the positive emotional subscale of the Psychological Consequences of screening Questionnaire (PCQ). 23 These were: ‘Do you think that your experience of having the Flexi-S cope test has …’ ‘Made you feel more hopeful about the future’, ‘Made you feel less anxious about bowel cancer’, ‘Given you a greater sense of wellbeing’. Response options were on a 4-point Likert scale: ‘not at all, a little bit, quite a bit, a great deal’ and were summed to produce a score from 3 to 12, with higher scores indicating more positive consequences. Cronbach's alpha in the present study for the emotional items was 0.81, which is similar to the value of 0.89 reported for the full 10-item scale which contains both positive and negative emotional items.
Secondary outcome variables
Reassurance was assessed postscreening using a single item on reassurance from the PCQ: ‘Do you think that your experience of having the Flexi-S cope test has given you a sense of reassurance that you do not have bowel cancer’. Response options were on a 4-point Likert scale: ‘not at all, a little bit, quite a bit, a great deal’ with higher scores indicating greater reassurance.
Generalized anxiety was measured before and after screening using the six-item version of the Spielberger State Anxiety Inventory. 24 This asks people to consider how they are feeling ‘right now’ and includes items such as ‘I feel calm’, ‘I am tense’. Responses were added giving a score of between 6 and 24 with higher scores indicating higher levels of anxiety.
Bowel symptoms were assessed before and after screening with the stem question: ‘Because we are studying bowel screening, we would like to know how often people get these bowel symptoms. ‘In the LAST THREE MONTHS have you’: ‘been constipated’, ‘had haemorrhoids (piles)’, ‘had diarrhoea’, ‘been troubled with wind’, ‘had pains in the abdomen (gut)’, ‘had bowel incontinence’, ‘noticed blood in your stools’. Response options for each symptom were: ‘no’, ‘occasionally’, and ‘frequently’. Scores were calculated by counting a response of occasionally or frequently as indicating the presence of a particular symptom and the total number of symptoms was calculated on this basis, with a range of 0–7.
GP attendance was measured before and after screening using one question: ‘About how many times have you been to see your GP in the last 3 months?’ Response options were: ‘Haven't been, once, twice, three or more times’. It was scored so that higher scores indicated more frequent visits.
Statistical analysis
Between-group analyses of variance (ANOVAs) were used to test for differences between screening outcome groups. Contrasts were used to examine whether the surveillance group differed from the three other outcome groups. Changes over time (pre-postscreening) were assessed using repeated measures ANOVA with time as a within-subjects variable and screening outcome group as a between-subjects variable.
Results
Demographic variables
Outcomes groups differed significantly by age and gender. The groups with lower-risk polyps and higher-risk polyps assigned to surveillance were slightly older than the group with no polyps (average age – no polyps: 60.3; lower-risk polyps: 60.5; higher-risk, discharged: 60.5; higher-risk and surveillance: 60.7). All three groups with polyps had a higher proportion of men (no polyps: 46% men; lower-risk polyps: 62%; higher-risk, discharged: 62%; higher-risk, surveillance: 68%). Deprivation was not associated with polyp status. Age and gender were therefore entered into all analyses as independent variables, but results are only reported where age or gender moderated the psychological impact associated with different screening outcomes.
Postscreening scores
Primary outcome variables
It was hypothesized that any adverse psychological effects would be observed on the measure of bowel cancer worry rather than general psychological distress (using the GHQ). As predicted, bowel cancer worry differed across the four groups (F3,31904 = 16.3; P < 0.001) but planned contrasts showed higher worry in the surveillance group compared with the no polyps group, and no significant differences between the surveillance group and the other two groups with polyps. And while general psychological distress (GHQ) differed by outcome group (F3,32055 = 2.66; P < 0.05), the surveillance group reported lower distress than the no polyps or lower-risk polyps groups (see Table 1).
Postscreening measures of psychological impact by screening outcome (means and SEs)
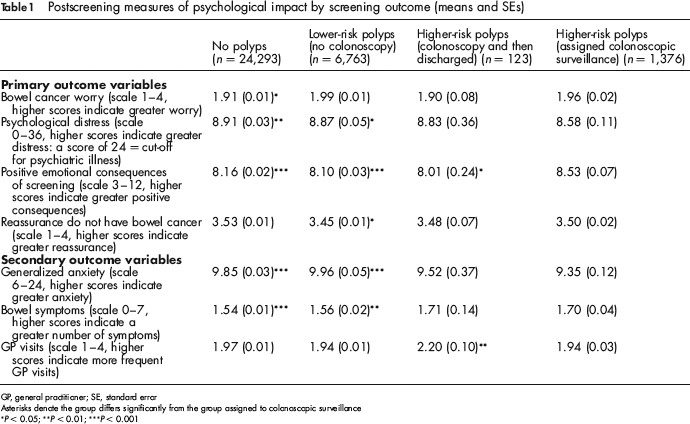
GP, general practitioner; SE, standard error
Asterisks denote the group differs significantly from the group assigned to colonoscopic surveillance
P < 0.05;
P < 0.01;
P < 0.001
It was also hypothesized that people referred for surveillance colonoscopy would have more positive views of screening than those found to have no polyps but equivalent levels to the other two groups with polyps detected at screening. There were significant differences across the groups (F3,31971 = 9.37; P < 0.001) but contrary to predictions the surveillance group reported higher positive consequences of screening than all three of the other groups. They also reported higher reassurance than the lower-risk group, although reassurance scores did not differ from the two remaining outcome groups. There was a significant age-by-group interaction (F3,32054 = 3.38; P < 0.05), with no age differences in reassurance among people with no polyps or lower-risk polyps, but greater reassurance among those over 60 who were assigned to surveillance (F1,1349 = 6.78; P < 0.01) (see Table 1).
Secondary outcome variables
Anxiety differed across outcome groups (F3,31667 = 7.22; P < 0.001), with people assigned to surveillance reporting significantly lower postscreening anxiety than either the lower-risk or the no polyps groups (see Table 1). There were also group differences in bowel symptoms (F3,288869 = 5.73; P < 0.001) and GP visits (F3,30601 = 3.60; P < 0.05) with the surveillance group reporting more bowel symptoms postscreening than the no polyps or lower-risk groups, but this was not reflected in help-seeking as they reported fewer GP visits than the group discharged following colonoscopy and did not differ from the lower-risk or no polyps groups on this measure.
Pre- and postscreening measures
In order to check whether postscreening group differences simply reflected prescreening group differences, and also to see whether factors such as worry increased or decreased following attendance at screening, we examined longitudinal changes in a subsample. As noted earlier, these analyses excluded the group discharged following colonoscopy because the sample size was too small.
There were no differences between outcome groups on pre-screening bowel cancer worry, generalized anxiety, number of bowel symptoms reported, or frequency of GP visits. Bowel cancer worry declined over time (F1,6440 = 45.9; P < 0.001) with a significant interaction between change in worry over time and outcome group (F2,6440 = 4.11; P < 0.05). However, reductions in worry in the surveillance group were greater than the lower-risk group, although did not reach conventional levels of significance (F1,1743 = 3.34; P < 0.10) and no difference was observed between the surveillance and no-risk group (see Table 2).
Pre- and postscreening measures of psychological impact by screening outcome on subsample (means and SEs)
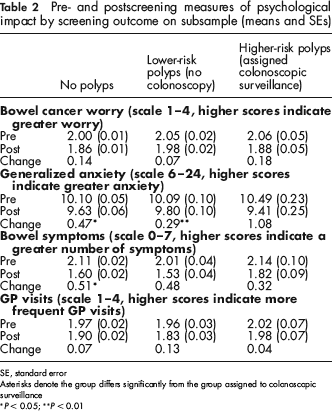
SE, standard error
Asterisks denote the group differs significantly from the group assigned to colonoscopic surveillance
P < 0.05;
P< 0.01
There was a significant reduction in anxiety over time (F1,6377 = 41.6; P < 0.001) and also a significant interaction with group (F2,6377 = 4.29; P < 0.05), with the surveillance group showing a greater reduction in anxiety compared with both the lower-risk polyp group (F1,1724 = 8.03; P < 0.01) and the no-polyps group (F1,4926 = 5.53; P < 0.05).
Although the number of reported bowel symptoms (i.e. diarrhoea, wind, pain, incontinence, blood, piles, constipation) decreased following screening (F1,5662 = 181.2; P < 0.001), the interaction between change over time and screening outcome group only approached significance. Pair-wise comparisons indicated smaller reductions in symptoms in the surveillance group compared with the no-polyps group (F1,4367 = 4.38; P < 0.05), but the former was similar to that observed in the lower-risk group. Self-reported frequency of GP visits decreased significantly over time (F1,5998 = 8.80; P < 0.01) but the interaction between change over time and outcome group was not significant.
Discussion
Following screening, bowel cancer worry was higher in the surveillance group than in those who had no polyps detected at screening but did not differ from the levels observed in the group found to have lower-risk polyps, suggesting that bowel cancer worry was related to the detection of growths in the bowel rather than being assigned to colonoscopic surveillance per se. In addition, declines in bowel cancer worry in the surveillance group were equivalent to those observed in the group found to have no polyps, supporting the idea that surveillance did not, in itself, make people worry about bowel cancer. On other measures there was evidence of beneficial psychological outcomes in the surveillance group, who reported lower general distress, more positive consequences of screening, and had greater reductions in anxiety compared with both the no-polyps group and the lower-risk polyps group. This suggests that the positive consequences of screening may extend beyond polypectomy and are perceived as greater among people assigned to colonoscopic surveillance. People assigned to surveillance were also more reassured that they did not have bowel cancer than the lower-risk group (who had polyps detected but no colonoscopy) and were equivalent to the levels observed among people with no polyps found, indicating that a comprehensive bowel examination following the detection of polyps offers as much reassurance as having no polyps detected in the first place.
Although there was evidence of residual concern about colorectal health among people assigned colonoscopic surveillance (with a smaller decrease in the report of bowel symptoms), the decline in symptoms was equivalent to those found to have lower-risk polyps, suggesting it was a consequence of having polyps detected rather than surveillance itself. In addition, there was no evidence of an associated increase in the use of primary healthcare resources.
Overall these findings are consistent with Liljegren et al.'s 19 results who found no increases in anxiety or depression among people receiving surveillance colonoscopy compared with the general population. There were hints in the latter study that anxiety was higher among men, but our study found no evidence that gender influences the impact of different screening outcomes.
No differences were observed between the group assigned colonoscopic surveillance and people discharged following colonoscopy on postscreening bowel cancer worry, psychological distress, reassurance they did not have bowel cancer, anxiety or number of bowel symptoms. If anything, the group discharged following colonoscopy showed evidence of relatively poorer outcomes reporting fewer positive consequences of screening and a greater frequency of GP visits compared with the surveillance group. However, relatively few people were discharged following colonoscopy and hence comparisons may have been underpowered to detect small differences.
While the overall sample size that would be required to obtain a larger sample of people discharged following one colonoscopy is prohibitive, future research could focus on the psychological consequences of being discharged from surveillance following a second or third colonoscopy as the available sample will be larger. Although it might be assumed that people would welcome being told they are no longer at higher-risk of colorectal cancer, previous research has shown that people are not always reassured by being told they are merely at ‘average’ risk of bowel disease following genetic test information 25 and similar levels of scepticism might arise in the context of being discharged from colonoscopic surveillance.
Limitations of the study include the lower response rates among men, younger people and people from areas with higher socioeconomic deprivation, and we cannot rule out the possibility that non-completers represent a vulnerable subgroup who experience adverse consequences following screening. However, with the exception of the group discharged following colonoscopy, completion rates were equivalent across the three outcome groups so it seems unlikely that this would have affected the pattern of results observed in the present study. Lower response rates in the group who were discharged following colonoscopy is more problematic and might have contributed to the failure to find differences between them and the group assigned to surveillance.
Information on the demographic characteristics of the sample was limited to age, gender and deprivation, leaving open the possibility that the screening outcome groups may have differed in other ways that could have influenced their responses. For example, differences between the screening outcome groups in dispositional optimism or depression may have led to greater endorsement of positive or negative items respectively. But if this were the case, differences between the screening outcome groups on pre-screening bowel cancer worry and anxiety should have been apparent, but no such differences were observed. In addition, the pattern of findings varied across measures, suggesting that global responses biases are an unlikely explanation for the effects observed.
No measures of general quality of life were taken so it is unclear whether surveillance colonoscopy might have a more general impact. However, both screening-specific and cancer-specific concerns were assessed (both positive and negative), and as noted in the introduction, previous research has tended to show stronger effects when specific rather than general measures of psychological impact have been used. 20 It therefore seems unlikely that adverse psychological effects associated with surveillance colonoscopy were undetected, although effects on social or physical aspects of life may have gone unobserved.
Additional limitations of this study include its focus on people who had taken up the offer of an invitation to be screened and who may therefore have more positive views on medical tests than other members of the general population. Consequently, the results may not generalize to a higher-risk group who are explicitly recommended to have screening, and among whom attitudes towards medical surveillance and testing may be less positive. In addition, we only assessed the relatively short-term psychological impact of screening and as a result do not know whether the observed positive consequences persist over time.
A further limitation was the use of single-item measures for a number of the outcome variables which are less reliable than multiple-item scales and may have reduced the likelihood of detecting significant differences. Although the large sample size compensates for this limitation to some extent, future research could use better measures of reassurance and use of health care to verify the findings observed here.
Conclusion
The results of the current study are broadly reassuring and show that referral for colonoscopic surveillance is not associated with adverse psychological consequences. Although postscreening bowel cancer worry and bowel symptoms were higher in people assigned to surveillance, they declined over time and were equivalent to levels observed in either one or both of the other two groups found to have polyps. This suggests they were a result of polyp detection rather than surveillance per se. Overall, surveillance itself appeared to be associated with better psychological wellbeing.
Footnotes
ACKNOWLEDGEMENT
This research was funded by a Health Technology Assessment grant and Cancer Research UK.