
Abstract
Objectives
To examine variations in screening status category with time for 20,862 invasive breast cancers diagnosed in the West Midlands between 1989 and 2006, and to provide 10-year relative survival rates for each category.
Method
Population-based breast screening was introduced in the West Midlands from 1988. Primary invasive breast cancers diagnosed from 1 April 1989 to 31 March 2006 in women eligible for breast screening were identified from the West Midlands Cancer Intelligence Unit's cancer registration database. A screening status was determined for each case using previously published methodology.
Results
Screening status rates are affected initially by the gradual rollout of the screening programme and more recently by the need to wait for three years before interval cancers and cancers in lapsed and non-attenders can be identified. In the steady-state period 1994–2003, 40.6% of invasive breast cancers were screen-detected, 36.3% were interval cancers and 11.2% were cancers in non-attenders (NA). Ten-year relative survival was 89.6% for screen-detected breast cancers, 73.3% for interval cancers and 51.9% for cancers in NA.
Conclusion
The detection of invasive breast cancers by screening has improved over time, with an equivalent reduction in the numbers of interval cancers. This, together with a stable rate of cancers in NA and an improvement in the survival of women with interval cancers, suggests that further improvements in breast cancer mortality can be predicted. International comparisons of interval cancer rates are difficult due to interprogramme differences in the time between screens.
Introduction
The number of invasive screen-detected (SD) breast cancers and their tumour characteristics (size, grade and nodal status) are reported annually5, 6 and compared with the number of cancers that one would expect to find on the basis of the Swedish Two Counties Study. 7 Interval cancers (cancers appearing after a women has been screened but before her next screen) are the next most frequently reported group 8 and can be used to provide additional monitoring. However, the collection of interval cancer numbers and characteristics requires time and accurate data collection by cancer registries for full ascertainment. Historically the UK cancer registries have had long lag times for ascertainment and incomplete data-sets, making comparison of interval cancer characteristics from the early years of screening difficult.
In 1993 the NHSBSP introduced guidance 9 on the collection and use of breast cancer data which identified five categories to which a breast cancer diagnosed in women eligible for screening could be assigned. These were: SD cancer, interval cancer, cancer in a non-attender (NA), cancer in a lapsed attender (LA) and cancer in a woman not invited for screening. There is little published literature on the allocation of a screening status category based on attendance for screening, and the implications of these data for the NHSBSP. In the West Midlands a breast screening status category has been derived for all breast cancers diagnosed in women eligible for screening from the introduction of the programme in 1988 to 2006. Details of the methodology have been published previously. 10 This paper examines variations in the screening status over time of invasive breast cancers, and provides 10-year relative survival rates for each screening status category. Particular attention is given to the variation in interval cancer rates with year of diagnosis and/or screening and the time between screening and diagnosis. The implications of these data for the efficacy of the NHSBSP are discussed.
Method
Breast screening in the West Midlands
The West Midlands region includes 11 % of the UK breast screening programme. The total population is 5,267,308 11 and, with a wide variation in social and ethnic backgrounds, it is representative of the UK as a whole. Screening started in 1988 and was rolled out over the subsequent three years. Screening initially consisted of a single mediolateral oblique view for women 50–64 years of age on a three-year cycle. Two views for prevalent screens were introduced in 1994 and two views for all screens from 2002. Expansion of the upper age range to 70 commenced in 2002. Compliance rates (uptake) are within the national minimum standard of 70%, with the region reporting an overall rate of 74.8% in 2007/2008. 6
Screening history status
A screening history status was allocated to all cases of primary invasive breast cancer diagnosed in women who were eligible for screening (aged 50–64) in the West Midlands since the introduction of the NHSBSP. For interval cancers the upper age range was extended by three years. Recurrences were excluded. As only one screening service in the region had started screening in 1988, screening histories for women diagnosed before 1 April 1989 were also excluded.
Each invasive breast cancer was assigned a screening status category using previously published methodology. 10 The main categories are: SD; interval (I); NA; LP; and not screened – diagnosed before first invitation. Invasive breast cancers assigned to the following categories which accounted for only 2.6% (n = 542) of the total were combined as ‘Other’: not screened – not known to the NHSBSP; not screened – ceased and defaulter.
The 389 invasive breast cancers for which a screening history status could not be determined were excluded from the final analysis. These included cases where insufficient screening information was available, cancers diagnosed in women who were not resident in the West Midlands or who were last screened outside the region, and cancers diagnosed in women who could not be traced on any NHS systems. After all exclusions had been made, 20,862 primary invasive breast cancers were included in the analysis.
Cancer incidence rates
Where cancer incidence rates were analysed by year of diagnosis, rates were calculated as the number of invasive breast cancers diagnosed per 1000 women eligible for screening in each year. Rates analysed by screening year were calculated as the number of invasive breast cancers detected per 1000 women screened each year (1 April-31 March the following year). Interval cancer rates were calculated using time from screen to diagnosis as specified by the NHSBSP 12 and do not include non-invasive or microinvasive cases, Pagets only or Pagets with ductal carcinoma in situ, and interval cancers diagnosed more than 40 months following the previous screen.
Relative survival
Relative survival is the observed survival in the patient group divided by the expected survival of the general population, matched by age and sex. The calculation of relative survival eliminates the effect of poor cause of death coding on death certificates; thereby avoiding one of the major drawbacks of cause specific survival analysis. The cumulative relative survival is interpreted as the proportion surviving a given interval after diagnosis in the hypothetical situation that breast cancer is the only possible cause of death. Expected survival probabilities for women in the general UK population were calculated using SURV2, a computer program originally developed by Hakulinen et al. 13 with probability of life tables supplied by the Government's Actuary Department. For each relative survival rate, 95% CI were approximated as twice the standard error. Relative survival curves were tested for statistically significant differences using likelihood ratio tests for inequality. 14
Results
Variation in screening status categories with time
Changes in screening status categories with time can be examined either according to calendar year of diagnosis (cancer registration perspective) or by allocating the cases to the screening year in which they could have been detected (screening perspective). Figure la shows for invasive breast cancers diagnosed in each calendar year from 1989 to 2005, the incidence rates for the five most common screening status categories. As each screening unit comes on line, the SD cancer rate rises rapidly as prevalent invasive breast cancers are detected. After reaching a peak in 1992 of 3.7 per 1000 eligible women when every programme has completed its first screening round, the SD cancer rate falls to around 3.0 per 1000 in 1995, before increasing steadily to 4.8 per 1000 in 2005. The rapid rise after 2002 probably reflects the introduction of two-view mammography for all women which, by the end of 2004, had been implemented by 100% of the region's screening units.
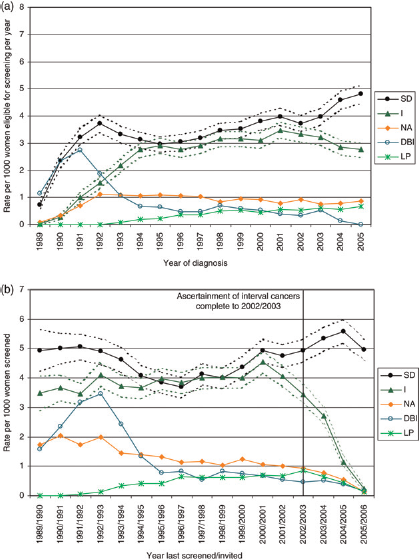
(a) Variation in invasive breast cancer screening status categories with year of diagnosis: cancer registration perspective (b) Variation in invasive breast cancer screening status categories with year last screened/invited: breast screening perspective
The invasive interval breast cancer rate rises until 1995 when it plateaus at around 3.0 per 1000 eligible women. The rate in NA levels off at around 1.0 per 1000 eligible women and the rate in LA increases slowly until 1999 after which it levels off at around 0.6 per 1000. The diagnosed-before-invited rate falls rapidly as each screening unit has completed its first three-year screening round before levelling off at around 0.6 per 1000 eligible women from 1994 onwards.
Figure 1b shows how the rates for the five most common screening status categories vary with the year women were invited for screening. Based on year last screened/invited, the SD invasive breast cancer rate is high at around 5.0 per 1000 women screened during the earlier years of the programme due to the detection of prevalent invasive breast cancers in the screened population as each unit comes online. The rate then decreases gradually to reach its lowest level of 3.7 per 1000 women screened in 1996/ 1997. From 2002/2003 onwards, the SD cancer rate rises steadily to reach 5.6 per 1000 women screened in 2004/ 2005, probably as a result of the introduction of two-view mammography for all women.
The invasive interval breast cancer rate varies between 3.5 and 4.1 per 1000 women screened from 1989/1990–1999/ 2000, with a sharp rise to 4.6 per 1000 women screened in 2000/2001. Between 2000/2001 and 2002/2003 the interval cancer rate begins to fall as the invasive breast cancer detection rate rises. From 2003/2004 onwards, the interval cancer rate falls because of delays in the ascertainment of cancers arising two and three years after screening. As expected, the rate in women diagnosed before their first invitation is high between 1989/1990 and 1993/1994 and then decreases rapidly as each programme completes its first three-year screening round; levelling off at less than 0.8 per 1000 women screened from 1995/1996 onwards. The rate in NA declines as the programme matures, and stabilizes at around 1.0 per 1000 from 1995/1996 onwards. As is the case with interval cancers, ascertainment of NA and LA cancers is incomplete from 2003/2004 onwards.
Overall distribution of screening status categories
Table 1 shows the distribution of the eight screening status categories for the 20,862 women aged 50–64 diagnosed with invasive breast cancer that were eligible for screening between 1 April 1989 and 31 March 2006. Because the ascertainment of interval cancer cases is only complete to 2002/2003 and because of the relatively high proportion of cancers diagnosed before invitation at the start of the NHSBSP, the proportion of interval cancers in Table 1 for the period 1 April 1989–31 March 2006 appears artificially low. If the proportions in each screening status category are re-calculated including only the 11,516 cases diagnosed between 1 April 1994 and 31 March 2003, the proportion of invasive interval breast cancers increases from 30.5% to 36.3%. This time period is referred to as the ‘steady-state’ period.
Distribution of screening status categories for invasive breast cancers diagnosed in women aged 50–64 who were eligible to be invited for screening between 1 April 1989 and 31 March 2006
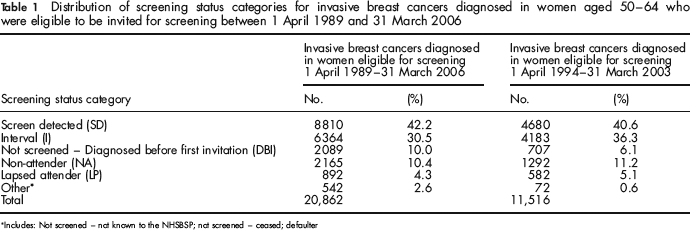
Includes: Not screened – not known to the NHSBSP; not screened – ceased; defaulter
Variation in interval cancer rates with time from screening to diagnosis
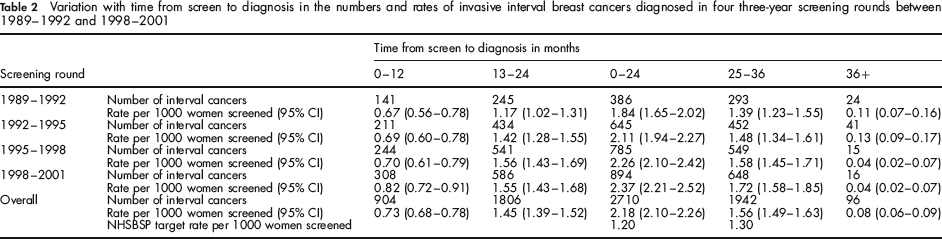
Table 2 shows how invasive interval breast cancer rates vary with the time from screening to diagnosis and compares interval cancer rates at 0–24 and 25–36 months with the NHSBSP target rates. At 0–24 months, the overall interval cancer rate (2.2 [95% CI 2.1–2.3] per 1000 women screened) is 1.8 times the NHSBSP target rate of 1.2 per 1000 women screened and at 25–36 months the figure of 1.6 (95% CI 1.5–1.6) is 20% higher than the NHSBSP target rate of 1.3 per 1000 women screened. There is an overall increase in the 0–24 month and 25–36 month interval cancer rates between 1989/1990–1991/1992 and 1998/ 1999–2000/2001, with the former rising from 1.8 (95% CI 1.7–2.0) to 2.4 (95% CI 2.2–2.5) per 1000 women screened and the latter from 1.4 (95% CI 1.2–1.6) to 1.7 (95% CI 1.6–1.9). The decrease with time in the number of interval cancers diagnosed after 36 months (from 0.1 per 1000 women screened in 1989–1992 to 0.04 per 1000 women screened in 1998–2001) represents improvements in round length as the NHSBSP matured.
Variation with time from screen to diagnosis in the numbers and rates of invasive interval breast cancers diagnosed in four three-year screening rounds between 1989—1992 and 1998—2001
Survival analyses
Figure 2 shows relative survival rates for invasive breast cancers in the five main screening status categories diagnosed between 1 April 1989 and 31 March 2006. Deaths were followed up to 9 May 2008. Women with invasive SD breast cancers have the best survival, with a 10-year relative survival rate of 89.6% (95% CI 88.5–90.8). The 10-year relative survival rate for interval cancers (73.3%, 95% CI 71.7–75.0) is slightly higher than that for cancers diagnosed in LA (66.9%, 95% CI 61.6–72.1). The 10-year relative survival rate for cancers diagnosed in NA is particularly poor at only 51.9% (95% CI 49.1–54.7).
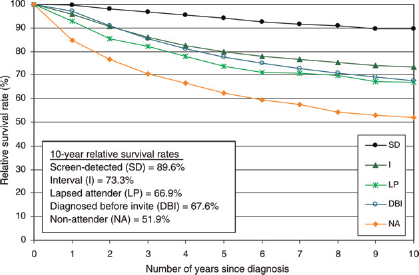
Variation in 10-year relative survival rate with screening status category for invasive breast cancers diagnosed 1 April 1989–31 March 2006 followed up to 9 May 2008 SD, screen-detected; I, interval; LP, lapsed attender; DBI, diagnosed before invitation; NA, non-attender
Figure 3 shows how five-year relative survival rates change with time for invasive SD and interval breast cancers diagnosed in four three-year periods. While there is a small (2.5%) increase in five-year relative survival in each three-year screening period for SD cancers from 92.4% (95% CI 90.3–94.6) in 1989/1990–1991/1992 to 94.7% (95% CI 93.3–96.1) in 1998/1999–2000/2001, interval cancers show a much more marked 19.5% change, with five-year relative survival increasing significantly (P < 0.001) from 70.7% (95% CI 67.1–74.3) in 1989/1990–1991/1992 to 84.5% (95% CI 82.0–87.1) in 1998/1999–2000/2001.
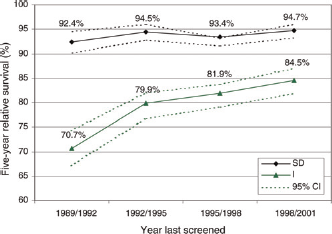
Variation in five-year relative survival with year of screening for women with invasive screen-detected breast cancers and invasive interval breast cancers
Discussion
This study shows that, in periods where the steady state is achieved (i.e. where the proportion of cancers diagnosed in women before their first invitation includes mainly those aged 50–52 and where sufficient time has elapsed for the interval cancers occurring up to three years after the last negative screen to be recorded), the majority (40.6%) of invasive breast cancers recorded in women eligible for screening are SD. This is encouraging, as is the gradual decrease in the cancers detected in NA from around 2.0 per 1000 women screened at the start of the NHSBSP to less than 0.9 per 1000 women screened in 2002/2003.
However, in terms of programme success, interval cancers are considered to be the most important category. A number of studies have looked at the incidence of interval cancers in randomized controlled trials and screening programmes15, 16 but there is little consistency, mainly because of differing screening interval and background incidence. Nevertheless, in most studies the interval cancer rates exceed the targets set by the NHSBSP. 17–19 This study confirms these findings, with interval cancers rates in the first two years 1.8 times higher than the target of 1.2 per 1000 women screened and those in months 25–36 some 20% higher than the target of 1.3 per 1000 women screened.
One of the strengths of the present study is the time period it covers. With the exception of Bucchi et al 20 much of the previous research on this subject was based on data from the first few years of screening, with full ascertainment of cases for a maximum of two years while the programme was in its infancy. The present study has nine years of complete interval cancer data, for 1 April 1994 to 31 March 2003 when the NHSBSP was well established and continually improving. During this period, the invasive interval breast cancer rate (Figure la) rises steadily in parallel with the invasive SD breast cancer rate until 1998 when the two lines start to diverge. From 1999 onwards, the SD rate begins to rise and interval cancer rates begin to decrease, such that interval cancers form only 29% of the invasive breast cancers diagnosed in 2005 compared with 35% in 1994, and SD cancers form 51% of the invasive breast cancers diagnosed in 2005 compared with 40% in 1994. The higher initial interval cancer rates and lower SD cancer rates are likely to be due to suboptimal screening performance, single view and low background film density, 21 all of which have improved in more recent years.
The interval cancer targets set by NHSBSP 22 were based on a number of assumptions that in retrospect are not necessarily true. The time interval between screens in the Swedish Two Counties study was targeted to be 24 months, but in reality was closer to 33 months 23 and this was extrapolated to 36 months for the NHSBSP. One might therefore expect the 25–36 month interval cancer rate to be higher than the target. These interprogramme differences in the time interval between screening rounds makes international comparisons of interval cancers virtually impossible, particularly as, on an operational level, individual screening units are operating at an unquantified percentage variance with this stated interval.
We have presented invasive interval breast cancer rates in terms of the number of women screened or the number of women eligible for screening rather than as proportionate incidence,24–26 because both SD and interval cancer rates are affected by background incidence which is no longer known, as the UK has no control group since the introduction of population screening. The incidence of invasive breast cancer in the West Midlands was increasing by 2% per annum before screening started, and in the late 1990s the use of hormone replacement therapy has further inflated the background incidence.27, 28 These changes in background incidence presumably account for the essentially parallel rise in SD and interval cancer rates until the introduction of two views for incident screening between 2002 and 2004, which led to an improved sensitivity causing the two lines to diverge.
Case ascertainment is a key issue when using cancer registration data to monitor performance of a breast screening programme. The West Midlands Cancer Intelligence Unit (WMCIU) is perceived to maintain one of the better cancer registration databases, with 99% estimated completeness 29 for breast cancer in their resident population. Population leakage from around the borders is inevitable as women living and being screened within the West Midlands can opt to be diagnosed and treated in an adjacent region and their cancers would be registered elsewhere. Such problems are, however, reduced by regular case exchange between cancer registries and by de-duplication and cross-regional matching exercises undertaken centrally by the Office for National Statistics. Women also retire to other places in the UK or abroad. However, some remain registered with their family doctor, returning home for both screening and treatment.
The 10-year relative survival rankings of women with differing presentation matches those reported by the Swedish Two Counties Study, 3 with women with SD cancer surviving relatively better than those with either interval cancers or cancers diagnosed before invitation whose survival is in turn much better than that of NA who have actively declined screening invitation(s).
The true effect of improved treatment is shown in the 19.5% increase in 10-year survival of interval cancers between 1989–1992 and 1998–2001 compared with the 2.5% increase seen for SD cancers.
In conclusion, the West Midlands breast screening histories project is proving to be a useful resource with which to evaluate the effectiveness of the NHSBSP in the West Midlands. The detection of invasive breast cancers has improved over time, with an equivalent fall in the numbers of interval cancers. This, together with a stable rate of cancers in NA and an improvement in the survival of women with interval cancers, suggests that further improvements in breast cancer mortality can be predicted. From a quality assurance perspective, categorizing invasive breast cancers in this way allows the identification of individual screening services which may stand out either in terms of good or bad practice. While the bad practice can be addressed and modified, good practice can be incorporated into future guidelines, allowing the continual improvement of the programme.