
Abstract
Objectives
In an attempt to improve breast cancer screening uptake and coverage, persistent non-offenders in the Heart of Birmingham Teaching Primary Care Trust were included in an invitation management initiative.
Methods
Persistent non-attenders were identified in routine screening lists. Phone contact was attempted or a home visit was made. If the case was not resolved, a second appointment was made and further phone calls and home visits were attempted.
Results
Of 548 persistent non-attenders identified, 228 (42%) declined screening, 171 (31%) attended, 72 (13%) had moved away or died, 11 (2%) were recently screened or under care for other conditions. Sixty-six cases (12%) remained unresolved. Fourteen women opted to be permanently withdrawn from the National Health Service Breast Screening Programme (NHSBSP). Twenty-four women had a negative experience of breast cancer screening (defaulted, recalled for assessment, recalled for technical reasons). No malignancies were found. A total of 1375 phone calls and 230 home visits were attempted. Uptake would have been 62.2% if none of the persistent non-attenders included in the initiative had attended for screening. With the initiative, uptake of breast cancer screening was increased to 65.3%.
Conclusions
Phone calls and home visits resulted in only a moderate increase in breast cancer screening uptake. The initiative encouraged nervous attenders who were reassured about the screening process. However, more women declined screening than were screened and the initiative made it easier for women to request to be permanently withdrawn from the NHSBSP.
Introduction
NHS breast screening coverage for women aged 53–64 years in the Heart of Birmingham Teaching PCT (tPCT) was 67.0% at 31 March 2007. That is, of the 11,500 women in the tPCT eligible to receive an invitation to the NHS Breast Screening Programme (NHSBSP) 7704 (67.0%) were screened in the previous three years. The tPCT is responsible for ensuring that general practices within their area maintain accurate GP lists, from which the eligible women are selected. Breast cancer screening for the tPCT is provided by two services which are responsible for screening 70% and 30% of the eligible population. GPs are provided with relevant information to enable them to encourage women to attend their appointment.
Coverage can be improved by ensuring women are invited every three years and that the eligible population does not include inactive patients who have moved away or died. Coverage can also be improved by increasing breast cancer screening uptake; the proportion of women sent an invitation for screening who attend. Initiatives that attempt to adjust one of these three factors may also affect the other two. Making extra efforts to encourage women to attend for screening may identify inactive patients on the screening lists. However, if uptake initiatives are not coordinated within screening round plans they may also delay the screening of the next batch of women, whose time between screens may slip beyond three years. This reduces the efficacy of breast cancer screening.
Heart of Birmingham tPCT is an urban area with a mobile population which makes it difficult to maintain accurate lists of women eligible for breast cancer screening. The area served has high levels of deprivation and the majority of the population is from minority ethnic communities; two factors associated with reduced uptake of breast cancer screening. 2 Nationally, uptake of breast cancer screening by women who received a routine invitation after failing to respond to all previous invitations was 19%. 3
To attempt to improve breast cancer screening uptake and coverage, persistent non-attenders identified within scheduled batches were included in an invitation management initiative involving telephone calls and home visits. The initiative was implemented by the Heart of Birmingham tPCT following the success of similar interventions to improve uptake of childhood immunization appointments.
Methods
The invitation management initiative targeted persistent non-attenders, defined as women who had missed more than one breast cancer screening appointment. Lists of women to be offered routine screening during the project period (22 January-31 May 2007 at the South Birmingham Breast Screening Service and 10 April-2 August 2007 at the City Hospital Breast Screening Service) were checked to identify persistent non-attenders. These women were sent a standard invitation letter with a timed appointment. Phone numbers were identified from the GP register. If a phone number was available, the woman received a phone call from staff working within the service following the routine invitation letter. Foreign language support was available as required. The purpose of the call was to ascertain if the woman intended to attend for screening, had any questions before deciding to attend and to offer her the opportunity to change her appointment if it was not convenient. A reminder call was made one working day before the woman's screening appointment. If the phone number was incorrect, attempts were made to obtain a new number using existing links between the screening service, the tPCT and general practices. Where no phone contact was possible, a home visit was made by a public health researcher provided by the tPCT. A case was said to be resolved if the patient had a determined outcome (attended, declined, inactive, recently screened or under care for other conditions). If a case was not resolved at the first stage, a second appointment was made by the screening office. Phone calls and home visits were again made at this second stage. A limit of five attempted phone calls was set for each stage.
Results
Outcomes
In total 548 persistent non-attenders were included in the initiative and received 1375 attempted phone calls and 230 attempted home visits. Overall, 482 cases (88%) were resolved. 228 women (42%) declined the screening appointment, 171 women (31%) attended the screening appointment, 72 women (13%) were found to be inactive patients and eight women (1%) had recently had breast mammography so could not be rescreened. Three women (1%) declined the screening invitation because they were under care for other conditions. Sixty-six cases (12%) remained unresolved.
Experiences of women
Seven of the 171 women (4%) who attended their screening appointment defaulted at some stage during the screening process. Three were not screened, one defaulted after one X-ray (i.e. did not complete the two-view screening process), two did not return after a technical recall and one did not return for assessment following the initial screen. Five women (3%) needed to return for technical reasons before being given a routine recall result and 12 women (7%) were recalled to assessment before being given a routine recall result. These women had a negative experience of breast cancer screening following inclusion in the initiative. No malignancies were found in women included in the initiative.
Women were not routinely asked to comment on their experience, but comments written on the data capture form were analysed. Negative comments were recorded from 10 women who were angry at receiving unsolicited phone calls or home visits about breast cancer screening. Conversely, positive comments were recorded from 10 women who were glad to be reminded to attend their appointment. The phone calls and home visits were welcomed by those women who wanted more information about the breast cancer screening process. Routinely, women invited to breast cancer screening are asked to call the screening office if they wish to change the assigned screening appointment. The direct phone calls and home visits undertaken as part of this initiative made it easier to change to a more convenient appointment time through emphasizing this existing facility.
Since every woman in the tPCT screening initiative was telephoned or visited, there was a greater opportunity for women to decline screening rather than to simply not attend their appointment. Fourteen of the 228 women (6%) who declined the screening invitation opted to be permanently withdrawn from the NHSBSP, which means that these women will no longer be invited for breast cancer screening. Overall, 23 of the 228 women (10%) who declined the screening invitation either reacted angrily at receiving an unsolicited phone call or home visit or opted to be permanently withdrawn from the NHSBSP.
Uptake of breast cancer screening
While the initiative was being carried out at each breast screening service, 5180 women from the Heart of Birmingham tPCT were invited for breast cancer screening, including previous attenders and women being invited for the first time. Uptake would have been 62.2% if none of the 548 persistent non-attenders included in the initiative had attended for screening. With the initiative, uptake of breast cancer screening was increased to 65.3% (Table 1). In these uptake figures the denominator has been adjusted to remove the 72 inactive patients identified by the initiative.
Uptake of breast cancer screening
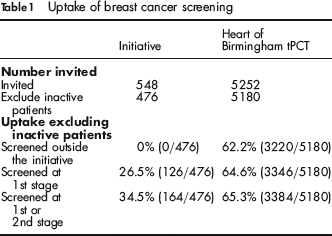
The improvement in uptake was mostly achieved at the first stage of the initiative; first appointment letter, phone call and in some cases a home visit undertaken before the first appointment. This stage resulted in 26.5% of women in the initiative being screened at their first appointment. 8.0% of women in the initiative did not attend their first appointment, but were screened at the second stage; second appointment letter, phone call and home visits where possible, after their first missed appointment. Phone calls and home visits to persistent non-attenders before the first offered screening appointment increased uptake from 62.2% to 64.6%. Continuing to target those persistent non-attenders who did not attend their first appointment increased uptake by a further 0.7 percentage points to 65.3%.
Of the 22 general practices taking part in the initiative, only two would have achieved the 70% uptake target without the initiative. A further three general practices met or exceeded the target as a result of this initiative. One general practice, which invited 147 women to breast cancer screening during the initiative, screened 81 women (55.1%) outside the initiative and 19 women as part of the initiative. The uptake for this general practice rose by 12.9 percentage points from 55.1% to 68.0%. Six other general practices with uptake under 60% for women screened outside the initiative raised their uptake by between 2.9 percentage points and 6.7 percentage points as a result of the initiative.
Number of phone calls and home visits
The invitation management initiative represented a large body of work for the tPCT and the screening offices. In total the 548 cases in the initiative received 1375 attempted phone calls and 230 attempted home visits. 274 (20%) of the attempted phone calls and 26 (11%) of the attempted home visits were to the 126 women who were screened at the first stage. 179 (13%) of the attempted phone calls and 20 (9%) of the attempted home visits were to the 38 women who were screened at the second stage.
Discussion
The enhanced activity of phone calls and home visits resulted in a moderate increase in breast cancer screening uptake from 62.2% to 65.3%. However, more women declined screening than were screened (228 [42%] declined, 171 [31%] attended for screening). Sufficiently detailed data were not recorded on the time spent by different staff groups in order to achieve these results and therefore an indication of the total cost of this intervention cannot be calculated. In order to justify such initiatives on economic grounds, time spent would have to be accurately recorded.
Because every woman in the tPCT screening initiative was telephoned or visited, this made it easier for women to decline screening or to be permanently withdrawn from the NHSBSP. All women who are eligible to receive a breast cancer screening invitation every three years should make an informed choice whether or not to attend on each occasion. When a woman is withdrawn from the screening programme, no further invitations will be offered. Withdrawing from the NHSBSP should be rare and a disclaimer letter (withdrawal form) must be completed to show informed choice. Steps should have been taken to reduce the number of cases opting out permanently from the programme and to decrease the possibility of women asking to be withdrawn from the programme solely on the basis of an unsolicited phone call or home visit.
Phone calls and home visits made it easier for women to arrange a more convenient screening appointment and provided a reminder to others to prompt them to attend. In addition, the initiative encouraged nervous attenders who benefited from receiving reassurance about the screening process including clarification that the screening was undertaken by females. These positive experiences should be carefully balanced with the negative comments received from women who were angry at receiving unsolicited phone calls about breast cancer screening. Furthermore, careful consideration should be given to the ethics of contacting women in this manner to enable and therefore encourage attendance at breast cancer screening.
Thirteen (8%) of the 171 women who attended for breast cancer screening were recalled to an assessment clinic for further investigation. No breast cancers were detected. A further seven women (4%) needed to have their films repeated for technical reasons. As women who have never attended for breast cancer screening are less sure of what to expect from the screening appointment a higher level of technical repeats generally occurs due to movement during the X-ray exposure. Also, as there are no previous films with which to compare the images, these women are more likely to be recalled to assessment. These factors should be considered and planned for when contemplating such an initiative and the special needs of these women in terms of returning to an assessment clinic should not be underestimated to avoid women having a negative experience of breast cancer screening.
The initiative enabled the tPCT to identify 72 inactive patients who were found to have moved away or died. PCTs must seek to minimize the number of inactive patients on GP lists. This is not only a breast cancer screening issue but affects all population-based public health programmes; e.g. cervical screening, bowel cancer screening and childhood immunizations.
Footnotes
Acknowledgements
The authors are grateful to the Heart of Birmingham tPCT which funded the analysis of these data, the City Hospital Breast Screening Service and the South Birmingham Breast Screening Service which carried out this initiative; Helen Morris, Rita Khan, Andrew Rouse, Sapna Sharma, Linda Gunn, Louise Flynn and Victoria Turner.