
Abstract
Objectives
To determine the prevalence of permanent and transient congenital hypothyroidism (CH) in Isfahan, Iran.
Methods
In 256 primarily diagnosed CH patients identified through the neonatal screening programme from May 2002 to February 2005, treatment was discontinued for 4 weeks and T4 and thyroid stimulating hormone (TSH) were measured. Permanent or transient CH was determined from the results of the thyroid function tests and the radiologic findings. Patients with TSH levels >6 (mIU/I) were diagnosed with permanent CH.
Results
Results were available from 204 patients, of whom 122 patients were diagnosed with permanent CH (59.8%) (prevalence 1:748 births), and 82 with transient hypothyroidism (prevalence 1:1114). Permanent CH was associated with higher initial TSH levels than transient hypothyroidism (P < 0.05). The most common aetiology of CH was dyshormonogenesis.
Conclusion
The rates of both permanent and transient CH in our study were higher than the comparable worldwide rates. The transient group had low T4 levels, suggesting that iodine contamination should be investigated. The aetiology of CH was also different from that recorded in many other studies.
Introduction
Permanent CH may result from defects in the proteins involved in the synthesis of thyroid hormone as well as from defects of transcription factors involved in the development of the thyroid gland.6–9 Most cases of permanent CH result from thyroid gland dysgenesia, which includes athyreosis, thyroid ectopia, or hypoplastic gland in situ. The pathogenesis of most thyroid dysgenesis cases remains unknown.10,11
Transient CH can be caused by iodine deficiency, exposure to excess iodine in the perinatal period (e.g. use of iodinated disinfectants or contrast agents) or fetal exposure to either maternally derived thyroid-blocking antibodies or anti-thyroid drugs taken by pregnant women with autoimmune thyroid disease. 12–15
After the elimination of iodine deficiency, screening programmes for congenital hypothyroidism were established in Iran in Tehran and Isfahan, although using different screening methods. The overall incidence of CH was high in both areas (1/914 in Tehran and 1/370 in Isfahan).16–17 Recently, Ordookhani et al. have reported a high prevalence of a permanent and severe form of CH among their studied population in Tehran. 18
We aimed to determine the incidence of permanent and transient CH among neonates diagnosed during the first three years of the CH screening programme in Isfahan.
Material and Methods
The Isfahan CH screening programme began in May 2002 and is continuing. The figure shows the structure of the programme (Figure 1). All three-seven day old neonates were referred to the Endocrine and Metabolism Research Center (EMRC) of Isfahan University of Medical Sciences. Using a questionnaire, a neonate's sex, weight, height, head circumference, and maternal age and any parental consanguinity were recorded. Venous blood samples were obtained from the cubital vein on the day of referral, and serum T4 and thyroid stimulating hormone (TSH) levels determined.
CH Neonatal screening programme, Isfahan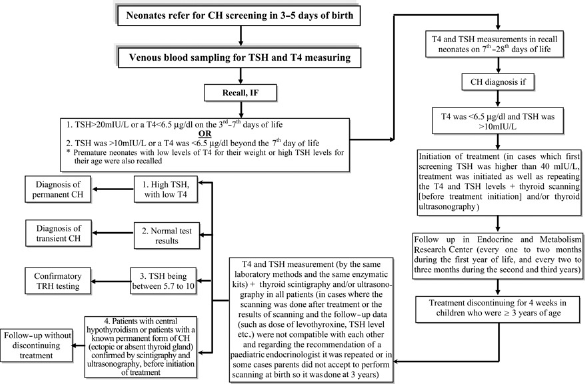
A paediatric endocrinologist and collaborating general practitioners evaluated the laboratory results and the questionnaire, and after physical examination, the neonates who needed to be recalled were determined. The need for recall was based on the measured T4 and TSH levels. Neonates with a TSH > 20 mIU/L or a T4 <6.5 μg/dl on the third-seventh days of life were recalled. Beyond day 7, neonates were recalled if their measured TSH was >10mIU/L or their T4 was <6.5 μg/dl. Premature neonates with low levels of T4 for their weight or high TSH levels for their age were also recalled. 17
If the first TSH level was between 20 and 39 mIU/L, T4 and TSH measurements were repeated. If the TSH level was >40 mIU/L, treatment was initiated in addition to repeating the T4 and TSH levels. If the results of the second lab tests were within normal limits, the neonates were considered to have transient TSH elevation. In such cases, treatment was halted and the subjects were excluded from the study. Otherwise, the treatment was continued.
A paediatric endocrinologist clinically examined recalled neonates. Based on the results of the secondary measurements (between days 7 and 28), neonates were considered hypothyroid if their T4 was <6.5 μg/dl and their TSH was >10mIU/L.19–23 In both preterm and full-term neonates whose T4 measurements were low according to their weight, 24 further tests including T3 resin uptake (T3RU) and free T4 index (FTI) were performed, and treatment was started after confirmation of secondary hypothyroidism or TSH > 10mIU/L. In a few neonates whose TSH levels were slightly above the upper limit of normal (5 < TSH < 10), thyrotropin-releasing hormone (TRH) tests were also performed.25–26
Neonates with confirmed hypothyroidism underwent treatment with a single dose of levothyroxine (10–15 μg/Kg/day). Before treatment, neonates with CH underwent thyroid scintigraphy with technetium pertechnetate to determine the aetiology of the hypothyroidism. Thyroid ultrasonography was performed when scintigraphy showed no uptake in the thyroid gland area to confirm thyroid agenesis.
Infants diagnosed with CH were followed closely in the first three years of life. They were followed up every one to two months during the first year of life, and every two to three months during the second and third years.
In order to distinguish between permanent and transient cases of CH, levothyroxine therapy was discontinued for 4 weeks in children who were ≥3 years old, after which time thyroid function tests (T4 and TSH) were evaluated by the same laboratory methods and the same enzymatic kits. 20 Thyroid scintigraphy and/or ultrasonography were performed in all patients after discontinuing treatment. Thyroid scanning at birth was performed before starting treatment, but in cases where the scan was performed after treatment, or the results of scan and the follow-up data (such as dose of levothyroxine, TSH level, etc) were not compatible it was repeated. In some cases parents did not give permission for scanning to be performed at birth, so it was performed at three years.
If the thyroid function tests showed a high TSH with low T4, the patient was diagnosed with permanent CH.23,24 Those patients with normal test results were considered to be transient cases. In those cases with TSH between 5.7 and 10, confirmatory TRH testing was performed.22,27 In patients with central hypothyroidism, or those with a known permanent form of CH (ectopic or absent thyroid gland) confirmed by scintigraphy and ultrasonography, therapy was not discontinued.
The aetiology of CH among patients with permanent CH was determined as follows: thyroid dysgenesis cases (agenesis, ectopia and hypoplasia) were confirmed by both scintigraphic and ultrasonographic imaging, and patients with abnormal thyroid function test results but normal scintigraphy and ultrasonography scans were considered to be cases of dyshormonogenesis.
Laboratory methods
TSH was measured with Iran Kavoshyar Co. kits using immunoradiometric assay (IRMA) methods. T4 level testing was performed using a radioimmunoassay (RIA) method, using Iran Kavoshyar Co. kits. The sensitivity of the T4 and TSH tests were 0.38 μg/dl and 0.05 mIU/L, respectively; these were controlled with a berthold LB 2111–12 gamma counter.
Statistical analysis
Mean and standard deviations for the demographic data, T4, and TSH levels in neonates were calculated. The mean serum T4 and TSH values of patients with permanent and transient CH were compared using one-way ANOVA during the study period (the first measurement versus after discontinuing therapy). The statistical analyses were performed with SPSS software (version 10).
Results
During the 33 months from May 2002 to February 2005, 91317 neonates were screened. Of the screened newborns, 51.3% were girls and 48.7% were boys (P < 0.05). Overall 992 neonates (1.1%) were recalled, from whom 256 patients were diagnosed as hypothyroid and underwent treatment. The overall incidence of CH was 2.8/1000 (1:357 live births). The female to male ratio was 0.7 (110:146). Parental consanguinity was present among 29.7% of all screened cases but was higher (37.6%, 96:255) in neonates with confirmed hypothyroidism (P = 0.005). First degree consanguinity was present among 72.9% (70:96) of CH patients (P = 0.0000).
Of 256 patients diagnosed with hypothyroidism, a diagnostic discontinuation of therapy at around three years was undertaken in 204. Among the others, two patients died, 12 were not referred for follow-up, two were diagnosed with central hypothyroidism, and 36 were followed up in the EMRC CH center but not referred to determining the permanency of CH at the time the study was performed.
In 204 patients, treatment was discontinued for 4 weeks and their T4 and TSH measured again. Of these, 122 (59.8%) were determined to have permanent CH. The remaining 82 (40.2%) were diagnosed with transient CH. The prevalence of permanent and transient CH was 1/748 and 1/1114, respectively. The characteristics of the patients with permanent and transient CH are presented in Table 1. The TRH test was performed in 19 patients, of whom six were diagnosed with transient CH and the reminder with permanent CH. In transient and permanent patients, 4 and 11 (6 dyshormonogenetic and 5 dysgenetic) were preterm, respectively.
Characteristics of neonates with permanent and transient CH
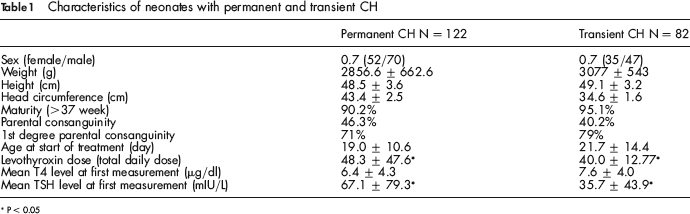
P < 0.05
According to the scintigraphic and/or ultrasonographic findings performed in 114 permanently CH patients and 54 transiently hypothyroid neonates, all transient CH patients had normal thyroid glands and in permanent CH patients, 67 (58.8%) had dyshormonogenesis and 47 (42.2%) had thyroid dysgenesis (36 agenesis or hypoplasia and 6 ectopia) (P < 0.05 for dyshormonogenesis vs. dysgenesis). The characteristics of the permanent CH patients with dyshormonogenesis and dysgenesis are presented in Table 2.
Characteristics of permanently hypothyroid neonates with thyroid dysgenesis and dyshormonogenesis
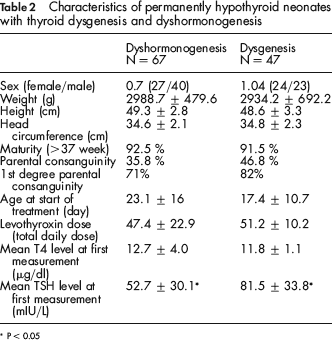
P < 0.05
Discussion
In this study of 204 patients with primary CH, 59.8% were confirmed to have the permanent form of the disorder. In the study by Gaudino et al. in France, 38% and 62% of 79 patients with CH were demonstrated to have transient and permanent CH, respectively. 28 In the study by Ordookhani et al. of 35 neonates with primary congenital hypothyroidism, 25 (71.4%) had permanent CH, six (7%) had transient CH, and four cases were unclassified. 18 In a study from Saudi Arabia, only two of 24 neonates with CH had transient CH. 29 It is generally accepted that 10–15% of primary CH patients are diagnosed with the transient type. 30 Higher rates of transient CH may be due to iodine deficiency, iodine overload, transplacental passage of thyrotropin (TSH) receptor-blocking autoantibodies, elevated thyroid autoantibodies, anti-thyroid drug ingestion or the use of iodine-containing topical antiseptics, maternal consumption of goitrogens and/or thyroid affecting medications, neonatal very low birth weight (<1500g) and prematurity (<37 weeks’ gestation), immaturity of thyroidal iodine organification, and gene mutations.12–15,19
Studies suggest that iodine deficiency is no longer a problem in the Isfahan region,31,32 and although neonatal departments have been asked not to use iodine-containing topical antiseptics, whether this recommendation has been followed is uncertain. The limitation of our study was that we did not measure urine iodine concentration of studied neonates.
Further investigations are needed to understand the causes behind higher rates of transient CH, and in particular the higher prevalence of elevated thyroid auto-antibodies in areas that were previously iodine deficient but where iodine supplementation has been implemented. The role of excess iodine should also be investigated. 33
A recent study by Ordookhani et al. has reported that elevated urine iodine concentration was the most frequent finding in newborns with transient CH. 34
The prevalence of permanent CH in our study was 1 in 748 live births. This is approximately five to six times higher than the worldwide incidence of CH. 1 The prevalence of transient CH was also higher (1 in 1114 live births). Comparing the findings of our study with other international research suggests that permanent CH in Isfahan was nearly two to three times more frequent than the prevalence of permanent CH in Greece (1 in 1800), Saudi Arabia (1 in 1400) and Turkey (1 in 2354).35,36,29 This difference may be due to dissimilarities between the screening methods, environmental, genetic or immunological factors as well as ethnicity.37–39
The female to male ratio of the permanently hypothyroid patients in our study was 0.7. This value differs from many other studies in this field, which have generally reported higher incidence of CH among females compared with males.18,30 This result could be a consequence of the high rate of parental consanguinity in our region, or of neonates with an undiagnosed family history of CH, as reported also by Castanet et al. 38 In Table 2, the female to male ratio in dysgenetic patients was high, and because 51.3% of screened newborns were girls and 48.7% boys, more girls were screened.
The rates of parental consanguinity among patients diagnosed with permanent CH and its different aetiologies or transient CH were similar. These findings are not in agreement with the results from the Ordookhani et al. study. 18 Further investigations are needed in this field in order to deduce the role of parental consanguinity and its effect on the incidence of CH, and whether it has a greater effect on the incidence of permanent versus transient congenital hypothyroidism, the proportion of CH in male and female, and on the incidence of dyshormonogenesis and dysgenesis.
The mean dose of levothyroxin was much higher among patients with permanent CH than those with transient CH, which was in accordance with other studies. Skodes et al. in Cyprus 35 have reported that children with transient CH require a lower dose of thyroxin in order to maintain normal thyroid hormone levels than those with permanent CH.
The mean T4 level before starting treatment was not significantly different among patients with permanent or transient CH, whereas in the study from Greece, 36 initial T4 levels correlate with the aetiology of CH. The mean TSH levels before treatment were significantly higher in the patients with permanent CH than in those with transient CH.
It was concluded from these findings that the first TSH and T4 levels may have a predictive role for identifying permanent forms of CH from the transient forms. In the study by Silva et al. in Brazil, carried out to assess the characteristics and aetiologies of congenital transient hypothyroidism, the TSH initial levels were not relevant to determine whether the thyroid dysfunction was transient or permanent. 40 The transient group had low T4 levels, which indicates that iodine contamination should be considered.
Although treatment was started earlier among patients with permanent CH compared with patients with transient CH, the difference in start times was not statistically significant.
In our study, the rate of prematurity was not significantly different between transient and permanent CH, whereas according to some reports prematurity is a risk factor for transient CH.28,41
The most common cause of CH, accounting for 85% of cases of permanent CH, is thyroid dysgenesis. Dyshormonogenesis accounts for the remaining 15%. 42 The results of our study were different from other studies in that 58.8% of neonates with permanent CH had dyshormonogenesis and 42.2% had dysgenesis. Although the most common aetiology of CH was dyshormonogenesis, there was no significant relationship between parental consanguinity and the two mentioned aetiologies. This may be due to small sample size or other unknown factors, which should be investigated using a larger sample size. In contrast to many studies, thyroid agenesis was more prevalent than thyroid ectopia among patients with thyroid dysgenesis.
Ordookhani et al. found that 51.4% and 48.6% of patients had dysgenesis and dyshormonagenesis, respectively, 18 and a study from Saudi Arabia also found that dyshormonogenesis was more prevalent. 28 These differences may be due to the higher rates of parental consanguinity in these regions. 3
Our data is not extensive enough to determine the rates and role of parental consanguinity, and its possible role in the aetiology of permanently hypothyroid children. In similar studies, (e.g. Ordookhani et al.) 42.9% and 55.6% of dyshormonogenetics and dysgenetics patients had parental consanguinity, respectively. 18
Conclusion
The preliminary data from our study suggest that the rate of incidence of permanent congenital hypothyroidism is high. The aetiologies behind the cases of CH in our study were different from those of other studies, even some conducted in the same country. The reasons for these differences are unclear, but variables including the environment, complex gene interactions, and immunologic factors probably play a role. Further studies with larger sample sizes will be critical in ascertaining the role of such variables in the incidence of the different forms of CH. The background information gained through studies such as this will be critical for the planning of appropriate genetic and immunologic studies in our region.