
Abstract
Aims
To evaluate whether willingness to undergo colonoscopy screening is influenced by being a first-degree relative of hospitalized patients with or without colorectal cancer after briefing and surgeon recommendation.
Methods
We performed a cross-sectional study of 327 first-degree relatives of hospitalized patients aged higher than 40 years, divided into Group A (151 relatives of colorectal cancer patients) and Group B (176 relatives of non-cancer patients) at the University Hospital of the Canary Islands, Spain. All were personally briefed by a surgeon, aided by a colorectal cancer pamphlet, and encouraged to accept screening colonoscopy with sedation.
Results
Willingness to undergo colonoscopy screening was greater in Group A (66.9%) than in Group B (29.0%); (odds ratio: 11.1; 95% confidence interval = 4.27 to 29.14; P < 0.001). Pre-briefing awareness of screening colonoscopy was also significantly higher in Group A (76.8% vs. 33.5%; P < 0.001), the main source of information being a close relative with colorectal cancer.
Conclusions
Being a close relative of a colorectal cancer patient is positively related with willingness to undergo colonoscopy screening in this study. This cross-sectional study outlines a strategy for increasing the level of willingness to undergo colorectal cancer screening in a group of people at risk.
Background
Colorectal cancer is characteristically silent in the early stages. 1 By the time symptoms appear, prognosis is usually poor. More than two thirds of colorectal cancer patients present with symptoms and nearly half already have distant or local metastasis. 5 For this reason, preventive screening has been proposed as the most effective method of reducing colorectal cancer-related mortality. Among the main screening techniques currently available, colonoscopy is widely used as it allows immediate detection and treatment of pre-cancerous adenomatous polyps. Evidence from a non-randomized intervention study shows that colonoscopic polypectomy may reduce the incidence of colorectal cancer by 76%6,7 with a 5-year survival rate of 90% or more for patients diagnosed with local colorectal cancer. 8 The other main screening techniques include fecal occult blood test, barium enema and sigmoidoscopy.
Many studies indicate that physician recommendation has a powerful motivating effect on screening participation. 1 Ignorance of the fact that early stages of colorectal cancer are mostly curable, together with underestimation of colorectal cancer risk factors, preparation for colonoscopy, discomfort of previous endoscopic procedures and overestimation of the complications of colonoscopy contribute to the poor level of understanding about this pathology and reluctance to undergo screening among the general population. 5
We wished to evaluate whether willingness to undergo colonoscopy screening is influenced by being a first-degree relative of hospitalized patients with or without colorectal cancer after briefing and surgeon recommendation.
Methods
Design
We performed a cross-sectional study of 327 people between October 2001 and June 2006 at our Hospital. Criteria for inclusion were: first-degree relatives and aged 40 years or more, with no previous colorectal cancer screening attendance, who visited hospitalized patients (parents, siblings or offspring).
They were divided into two groups: Group A consisted of 151 relatives of colorectal cancer patients and Group B consisted of 176 relatives of patients with non-cancer diseases. All were personally asked to attend a briefing in the Hospital Department of Surgery, by a member of the colorectal cancer surgical team before surgical intervention of their relatives. However, some patients of the relatives in Group B were not undergoing surgery.
Participants were briefed with the aid of a leaflet.
For the briefing sessions, a specially designed pamphlet (see appendix 1) containing graphic illustrations and explanatory text was administered and explained to all relatives in both groups. The participants were then encouraged to accept a screening colonoscopy with sedation.
Data collected included the following variables:
Main independent variable: Being a first-degree relative, that is, the parents, sibling or offspring of a hospitalized patient with or without colorectal cancer (Group A and Group B, respectively). Dependent variables:
Principal outcome: Willingness to undergo a colonoscopic screening. We categorized willingness Yes or No with respect to expressed intention to undergo colonoscopy screening, recorded immediately after the briefing. Other outcomes:
Fear of positive diagnosis (yes/no), Interest in information that measures the attitude to colonoscopy screening. It was recorded as favourable or not favourable. ‘Favourable attitude’ means that after the briefing the respondents considered colonoscopy screening ‘an interesting and good idea to detect and treat polyps’, Reasons for refusal (lack of time, fear of being diagnosed with colorectal cancer, discomfort or other causes), Awareness of screening colonoscopy, that measures pre-existing awareness of colonoscopy screening was also collected after the briefing, using the direct question ‘Did you know about colonoscopy before this briefing?’ (yes/no), The source of the knowledge about screening colonoscopy (a close relative with colorectal cancer, the media – primarily television, physician or a friend). Covariates included in the multivariate models Age, sex, place of residence (urban/rural) and whether the participants had a history of cancer disease (yes/no), type of relative (parent/sibling/offspring), educational variable was dichotomous, defined as ‘no educational level’ and ‘some educational level’ (elementary/secondary education/college/university). The independent variables age, sex, residence and type of relationship, a previous history of cancer disease and educational level were introduced in this study because of their possible impact on willingness to undergo colorectal cancer screening, considering their potential bias effect in the relationship between being a colorectal cancer relative and willingness.
Statistical analysis
Continuous variables are expressed with means and standard deviations. Ordinal and nominal variables are expressed with frequencies and percentages. Chi-square, Fisher exact tests and Kruskal-Wallis test were used for comparison of proportions, as appropriate. T-test was used to compare age means between Group A and Group B. Those significant variables in the bivariate analysis and those non-significant but considered as possible confounders were entered in the multivariate analysis. Logistic regression was used for modelling the relationship between the variables being a colorectal cancer relative and willingness, controlling for the following variables: being a relative of patients with or without colorectal cancer, subtypes of relatives (categorized as: sibling vs. offspring, sibling vs. parent and offspring vs. parent), age (categorized as equal or lower than 50 and higher than 50), sex, place of residence (rural vs. urban), some educational level (yes vs. no) and whether participants had a history of cancer disease (yes vs. no). The dependent variable was willingness. The method used for selecting the variables was entered, in the multivariate and bivariate analyses method. Odds ratios (OR) and 95% confidence intervals (CI) were calculated. A P value of less than 0.05 was considered statistically significant.
In another analysis, participants were grouped according to age, categorized as ≤50 years vs. >50 years. Two regression analyses were carried out with these two groups separately, using the variable ‘being a colorectal cancer relative’ as the main independent variable, with ‘willingness to undergo colonoscopy screening’ as the dependent variable and including in each analysis the covariates sex, educational level, history of cancer disease, urban residence and type of relative.
Finally, to test the interaction effect between being a colorectal cancer relative and age (≤50 vs. >50 years), we carried out a logistic regression analysis using as independent variables: being a colorectal cancer relative, categorized age, the interaction being a colorectal cancer relative by categorized age, sex, educational level, history of cancer disease, urban residence and type of relative, and willingness to undergo colonoscopy screening as the dependent variable.
Statistical analysis was performed with SPSS 17.0 (Chicago Ill), MedCalc 9.6.0.0 (Frank Schoonjans, Belgium) and StatXact 5.0.3 (Cytel Co., MA).
Results
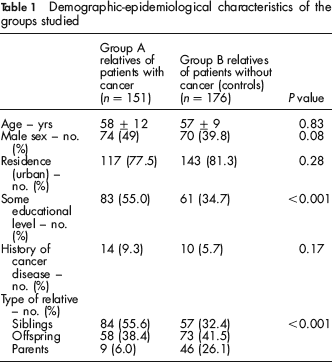
Table 1 shows the comparisons between baseline characteristics for the two groups of the study.
Demographic-epidemiological characteristics of the groups studied
Willingness was significantly greater in Group A (66.9%) than in Group B (29.0%); P < 0.001, as shown in Table 2.
Rates of willingness to undergo colonoscopy classified according to types of relatives and jointly
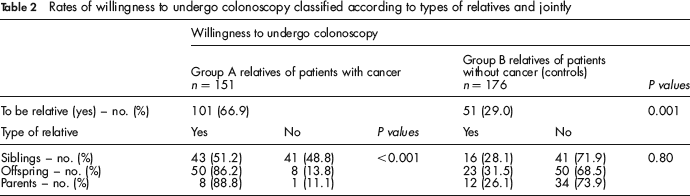
Table 2 shows the relationship between type of relatives and willingness to undergo colonoscopy. No differences were found in Group B, but within Group A the great majority of parents (88.8%) and offspring (86.2%) showed greater willingness to undergo colonoscopy as compared with siblings (51.2%).
Pre-briefing awareness of colonoscopy screening was higher in Group A than Group B (Table 3). The source of this knowledge was a close relative with colorectal cancer, higher in group A, the media – primarily television – and a friend, higher in group B and a physician, higher in group A.
Comparison between first-degree relatives of hospitalized cancer (Group A), and non-cancer patients (Group B) on awareness of colorectal cancer screening
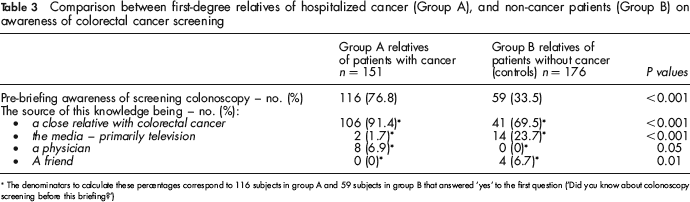
The denominators to calculate these percentages correspond to 116 subjects in group A and 59 subjects in group B that answered ‘yes’ to the first question (‘Did you know about colonoscopy screening before this briefing?’)
The majority of Group A, 79.4%, and Group B, 93.8%, showed a favourable attitude and difference was found between both proportions (P < 0.001). Reasons for unwillingness to undergo colonoscopy screening were as follows: fear of being diagnosed with colorectal cancer, 59.6% vs. 52.6%; endoscopy-related discomfort, 10.6% vs. 19.8%; lack of time, 23.4% vs. 17.2% and other reasons 6.4% vs. 10.3%. (Table 4).
Reasons for unwillingness to undergo colonoscopy screening between the groups
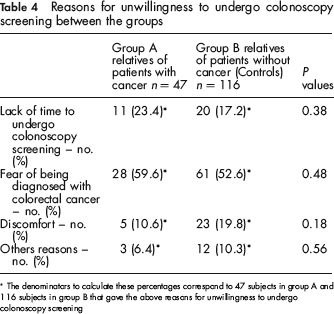
The denominators to calculate these percentages correspond to 47 subjects in group A and 116 subjects in group B that gave the above reasons for unwillingness to undergo colonoscopy screening
When age was categorized as ≤50 years and >50 years, stratified logistic regression analysis showed that the variable being a colorectal cancer relative was a significant predictor of willingness (OR = 24.6; 95% CI = 5.51–109.78, P < 0.001, for participants aged ≤50 years, and OR = 4.5; 95% CI = 2.47–8.05; P < 0.001, for participants aged >50 years).
To test the interaction being a colorectal cancer relative by categorized age (≤50 and >50 years), we performed another logistic regression analysis. The independent variables were: being a colorectal cancer relative, categorized age, the interaction factor being a colorectal cancer relative by categorized age, sex, educational level, history of cancer disease, urban residence and type of relative as independent variables, and willingness to undergo colonoscopy screening as the dependent variable. The results showed a principal effect of the variable being a colorectal cancer relative (OR = 6.7; 95% CI = 3.51–12.91, P= < 0.001) but we did not find a significant effect of the interaction term being a colorectal cancer relative by categorized age (OR = 0.5; 95% CI = 0.14–1.58, P = 0.23).
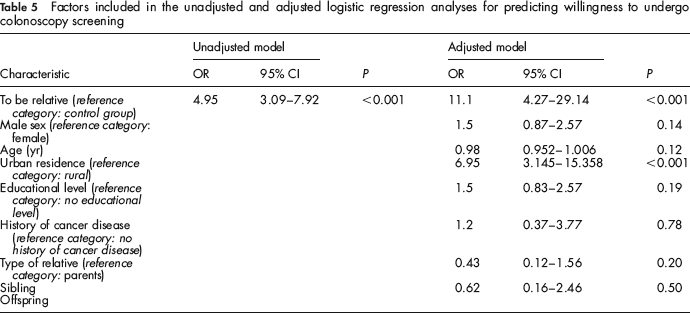
Table 5 shows the final multivariable models for willingness to undergo colonoscopy screening. We found an association between being a colorectal cancer relative and willingness to undergo colonoscopy screening, adjusted for residence (urban), type of relative of the patient, age, sex, some educational level and history of cancer disease (unadjusted analysis: OR = 4.95; 95% CI = 3.09–7.92; P < 0.001. Adjusted analysis: OR = 11.1; 95% CI = 4.27–29.14; P < 0.001).
Factors included in the unadjusted and adjusted logistic regression analyses for predicting willingness to undergo colonoscopy screening
Discussion
The main finding of this study was that first-degree relatives of colorectal cancer patients showed significantly greater willingness to undergo colonoscopy screening compared with those of other hospitalized patients. The fact that 66.9% of colorectal cancer relatives accepted colonoscopy screening is important; there are very few reports of higher intent rates.6,9 A surprising finding was that favourable attitude to colonoscopy screening (after the briefing) was higher in Group B participants, who were not related to colorectal cancer patients, than in Group A. The reasons for this are not clear, but speculatively may be related to levels of knowledge about screening and participant identification with genetic polyp risk groups. Group B participants, in general less familiar with colorectal cancer screening, expressed greater interest than group A, but, knowing they did not have the genetic risk factor, this interest did not manifest in willingness to undergo the procedure themselves.
The single most important risk factor associated with colorectal cancer is age > 50 years and incidence increases with age. 2 We used a cut-off age of >40 years, which is lower than that normally applied, as our main target Group (A) were first-degree relatives of hospitalized colorectal cancer patients and there is evidence linking genetic factors and increased colorectal cancer. 3 In this sense, we found few studies specifically aimed at patients with increased risk due to their colorectal cancer family history.
In our study, when age was included in the logistic regression analyses, in direct scores or categorized as less or equal and more than 50 years, unexpectedly we did not find an independent effect or an age-group by group interaction to predict willingness to undergo a colonoscopic screening.
In our view, the difference in willingness to undergo colonoscopy screening between the two groups was due to family experience of colorectal cancer in Group A, particularly among parents and offspring of hospitalized colorectal cancer patients as compared with siblings. This seems to have made them more receptive to the direct personal contact with a physician; together, they were more likely to arrive at the decision to undergo colonoscopy screening. Surgeons have been found to be powerful sources of screening information in family history colorectal cancer patients. 10
The use of general media educational campaigns is necessary to increase public awareness of the disease and the different screening techniques available, but may not be sufficiently motivating to increase participation in screening programmes. 2 Apart from public campaigns and physician recommendation, another supplementary strategy that may help increase participation is the use of personal reminders by mail or telephone. 3
With respect to screening programme design, a basic question arises as to what constitutes the most effective use of human and technical resources. Based on the literature, the answer seems to lie in combining physician recommendation with the most likely and available population at risk.
The recruitment approach used in this study takes advantage of the fact that all those included in the study voluntarily visited the hospital at regular intervals, which facilitated contact, and that they were all close relatives visiting seriously ill family members, so their heightened awareness of illness and its consequences may be assumed. Our working hypothesis was that such awareness and probable emotional involvement would modify their motivation to accept screening colonoscopy, especially when encouraged to do so by an experienced colorectal cancer surgeon.
Usually, lack of physician recommendation is considered as one of the top three reasons individuals do not undergo colorectal cancer screening, 11 including counselling the individuals about the timing of the follow-up colonoscopy, and lack of time to communicate with and to educate them. Physicians should expressly inform relatives about colorectal cancer screening, especially those with previous polyps who are at higher risk of developing colorectal cancer, and the fact that surveillance colonoscopy potentially decreases or eliminates their risk of developing colorectal cancer. 12
Colorectal cancer screening rates may be improved by increasing discussions about colorectal cancer screening between physicians and first-degree relatives of hospitalized patients. 13 Barriers to screening include public unawareness of the existence and usefulness of screening, the preparation and the inconvenience of colonoscopy, discomfort experienced in previous colonoscopy procedures and reluctance to undergo invasive endoscopic techniques.
With respect to reasons given for unwillingness to undergo the procedure, fear of colonoscopy was the most common reason given by both groups. The other reasons included lack of time and colonoscopy-related discomfort.
Others researchers have found that the most frequently cited reason for not screening was the absence of symptoms at the time of screening. These findings and ours reflect the generally low level of awareness about the silence, curability and seriousness of the disease and the increased risk of colorectal cancer because of their colorectal cancer family history.9–14–17
Referring to this point, Jacobs found that 96% of first-degree relatives of CRC patients would be screened if they were at risk for colorectal cancer; however, participants did not perceive themselves to be at risk of colorectal cancer. 18
A notable finding was that less than 7% of all first-degree relatives said that they had previously been informed by a physician about the existence of colonoscopy screening. This is striking as physicians are mostly responsible for promoting preventive medicine measures. It is clear that general practitioners or family doctors must have the awareness, means and time to identify individuals at risk and counsel them about the need to undergo screening. 3 This highlights a major concern in primary care worldwide: the problem of overburdened general practitioners. The study design shifted the burden of briefing onto a colorectal cancer surgeon to maximize the motivating effect, but in our opinion this role could be carried out by any authoritative physician or health professional.
Limitations
This pilot study has certain limitations. First, the study goes only part of the way to achieving the ultimate objective of all screening efforts – preventive intervention. However, our aim was to evaluate express willingness to undergo screening colonoscopy, a necessary link in the chain leading to such intervention.
Second, the design of this study placed considerable pressure on all those individuals with hospitalized relatives to accept colonoscopy, but this pressure was probably even greater for those with colorectal cancer relatives, which may have introduced a bias in the results. The pamphlet used in our briefing of participants focused mainly on Group A (relatives of colorectal cancer patients), but this is consistent with the aim of the study. Group B participants were enrolled to act as controls. However, the pamphlet also explains that polyps allowed to grow may turn into cancer and, in the general population, the risk of having polyps starts around the age of 50, so we feel it also applied to Group B participants who were approaching this age or had already reached it.
Third, the high rates of willingness to undergo colonoscopy screening may not manifest in actual performance, but we believe that the first step in the process leading up to performance is for people at risk to commit themselves by expressing willingness.
Finally, as with Group B, Group A people were informed by a colorectal cancer surgeon, but it must be said that in this study the colorectal cancer surgeon performing the briefing was only one of a team (of approximately 15 surgeons) that could be assigned to operate and the participants were so informed. Even so, we admit the possibility of extra pressure on Group A people, but this is consistent with the aim of the study.
Conclusions
Surgeon recommendation aimed at a targeted population at risk of colorectal cancer positively influenced the decision to participate in colonoscopy screening in this study. Once a patient with colorectal cancer is hospitalized, their relatives become more aware of the impact of the disease and show increased willingness to accept screening colonoscopy. The special relationship that develops between the surgeon and visiting relatives of hospitalized colorectal cancer patients may favour willingness to undergo colonoscopy screening.
The present study outlines a strategy for increasing the level of willingness to undergo colonoscopy screening in a group of people at risk. Physician recommendation and the recruitment approach used in the hospital proved effective and may constitute a model for increasing screening participation of people at risk.
Footnotes
Acknowledgements
The authors would like to thank Dr Alejandro Jiménez Sosa, Senior Methodological Consultant, for valuable advice regarding the preparation of the manuscript.
INFORMATION LEAFLET