
Abstract
Objective
To investigate the relationship between the level of disability and regular Pap smear testing among women in Taiwan and explore how this relationship may vary with the various levels of physician availability.
Methods
This population-based cohort study followed a total of 5,469,581 women from Taiwan, who were 30 years old or older in 2001 and covered the period January 2001 to December 2003. Of the total study population, 184,701 individuals were women with disability. Gynecologist-obstetrician/general practitioner to female population ratio was used as an indicator of physician availability. Multiple logistical regression models were used.
Results
After adjusting for age, socioeconomic status, racial group, residence area and physician availability, women with severe disability (OR = 0.38; 95% CI: 0.38, 0.39) were the least likely to undergo Pap smear testing. Women with moderate disability (OR = 0.59; 95% CI: 0.58, 0.60) and mild disability (OR = 0.88; 95% CI: 0.86, 0.89) were also significantly less likely to undergo a routine test than women without disability. Women residing in the areas with the greatest physician availability (OR = 0.93; 95% CI: 0.93, 0.94) were significantly less likely to undergo a Pap test than those in the areas with the lowest level of resource availability. The disparity in routine screening between women with and without disability remained across the different levels of physician availability.
Conclusions
In Taiwan, women with disability were found to be at higher risk of lower compliance than women without disability. The gap between women with and without disability persisted across different levels of physician availability.
Introduction
Previous studies have compared the use of preventive health services in women with and without disabilities. Several studies in the United States have shown that women with disabilities are less likely to receive a regular Pap smear.8–16 In contrast, one study revealed that wheelchair dependent spinal cord injured women had higher attendance rates for cervical cancer screening than the general female population in England. 17 Thus the findings on disability and cervical screening have varied, depending on the population studied.
Although previous research has revealed that there is an association between disability and cervical cancer screening, these studies may suffer from a number of limitations. Most of the studies used self-reported Pap test data as their data source and, therefore, were subject to recall bias.8–15 In addition, most previous studies focused on the disabled population in the United States and revealed a negative effect between disability and cervical cancer screening. This discrepancy between the results of these studies and the English study is possibly due to heterogeneity in the health care systems and the culture; therefore it may not be possible to generalize the findings in Western countries to Asian populations. No published study has examined the relationship between disability and cervical cancer screening using population claims data in an Asian country with a universal health care insurance system.
Furthermore, several studies have shown that an adequate physician availability correlates with earlier cancer detection.18–20 These studies have examined the effects of physician availability on the early detection of colorectal cancer, malignant melanoma and breast cancer. Other studies have revealed that residing in an area with a greater number of physicians is correlated with increased mammography and Pap smear testing. 21 It is therefore possible that an increase in physician availability may increase routine Pap smear testing among disabled women.
To better understand the relationship between cervical cancer screening and disability in an Asian society and the physician availability effect on cancer screening in disabled women, we conducted a population-based cohort study. We aimed to explore the relationship between level of disability and receipt of preventive services and whether the relationship is modified by physician availability.
Methods
Setting and Cohort
Taiwan implemented a universal and comprehensive National Health Insurance (NHI) programme in March 1995. In addition to curative services, the programme also provides several preventive services, including cervical cancer screening. A free annual Pap smear test is offered to women aged 30 and over.
This study was a population-based cohort study. Women at or above the age of 30 years in the year 2001 and enrolled in the NHI programme in Taiwan in the year 2001 were identified. Women who died before the end of 2003, had delivered between January 2001 to October 2004 or had previously undergone hysterectomy were excluded. The final study subjects consisted of 5,469,581 women, including 184,701 women with disability. The study cohort was analysed for their utilization of Pap smear testing from January 2001 to December 2003.
Data collection and study outcome
Four national registries in Taiwan were used to obtain information about individuals within the population: the NHI ambulatory claims data for 2001 to 2003, the NHI enrolment files in the year 2000, the Death Certificate Registry, and the NHI major disease file. People with physical and mental disabilities receive a government subsidy as part of the welfare programme in Taiwan. We identified each subject's disability status from the NHI enrolment files for the year 2000. Four disability categories were used: none, mild, moderate and severe. In Taiwan, those with disability are defined as people who are limited in their ability to engage in ordinary living activities and to participate in society, who, after evaluation by the committee composed of professionals from medicine, social work, special education and employment counselling, have one of the following physical or mental impairments: 22
Mental function and nervous system structure;
Sensory functions and pain involving the eye, ear and related structures;
Functions and structures involving the voice and speech;
Functions and structures related to cardiovascular, haematological, immunological and respiratory systems;
Functions and structures related to the digestive, metabolic and endocrine systems;
Functions and structures related to the genitourinary and reproductive systems;
Neuromusculoskeletal and movement-related functions and structures;
Functions and related structures of the skin.
According to level of severity and grades of disability, people with disability can then be categorized into three levels: mild, moderate and severe. Because the subsidy provided by the government is based on the level of disability and not types of disability, information on the type of disability is not available in the enrolment files.
This study includes control variables such as age, socioeconomic status (SES), ethnic status, geographic location of residence and medical resources. Because the NHI programme is financed by wage-based premiums for people with a clearly defined monthly wage and by fixed premiums for people who do not have a clearly defined monthly wage, we used the insurable income and categories as a proxy for the SES and this variable was divided into five levels. Women with a clearly defined monthly wage were classified into three categories: ≥NT$40,000, NT$20,000 to NT$39,999 and <NT$20,000. Women without a clearly defined monthly wage were categorized into three groups: farmers/fishermen, members of occupational unions and low-income persons. If the woman was not the primary policyholder, then the insurable wage/category of the insured primary policyholder was used.
The physician availability variable was obtained from The Medical Personnel Registry and 2000 census in Taiwan. The town level number of gynaecologists-obstetricians/general practitioners per 10,000 female population was used. We divided this variable into four levels, the lowest to the 25th percentile (0 ~ 5.41 per 10,000 female population), the 25–50th percentile (5.41 ~ 7.96 per 10,000 female population), the 50–75th percentile (7.96 ~ 11.24 per 10,000 female population) and the 75th percentile to the highest (11.24 ~ 190.48 per 10,000 female population).
Although the NHI programme offers free annual Pap smear tests to all women aged 30 or over, we followed the recommendation of the US Preventive Services Task Force to construct our dependent variable. Routine cervical cancer screening was defined as any use of a Pap smear test within a three-year period. From the details of the ambulatory care claims file, we dichotomized the outcome variable into ‘having at least one Pap smear test during the three-year study period’ and ‘not having at least one Pap smear test during the three-year study period’.
Unique and anonymous identifiers were used to link the different data sources. In order to protect privacy and assure confidentiality, all unique personal identifiers were encrypted and confidentiality assurance was addressed by abiding by the data regulations of the Bureau of National Health Insurance.
Statistical analysis
Simple and multiple logistic regressions were used to fit univariate and multivariate models so that risks for the study outcomes in women with/without disabilities could be compared. For each model, the odds ratios (OR) and 95% confidence intervals (CI) were calculated. All tests were two-sided. Power calculations were conducted to assure that the study had a sufficient power. Significance was set at P < 0.05. All analyses were conducted using the SAS 9.1 software package.
Results
The details of the study sample are presented in Table 1. The sample consisted of 184,701 women (3.4%) with physical or mental disability and 5,284,880 women (96.6%) without disability. The frequency of women without disability who had undergone at least one Pap test during the three-year study period was 51.7% and this was compared with women with disability at a mild, moderate or severe level where the rates were only 44.7%, 34.7% and 25.5%, respectively. Whereas 6.8% of women with severe disabilities were aged between 30–34 years, a higher percentage (13.3%) of non-disabled women fell into this age group. Overall, the women with disability were relatively older than the control population, but the women with different levels of disability shared a similar age distribution. The Sociodemographic characteristics, the racial groups and the register area were similar across all four groups of women (see Table 1).
The distribution of Sociodemographic characteristics and percentage of women undergoing smear testing by disability categories in Taiwan, 2001–2003. Values are numbers (percentage)
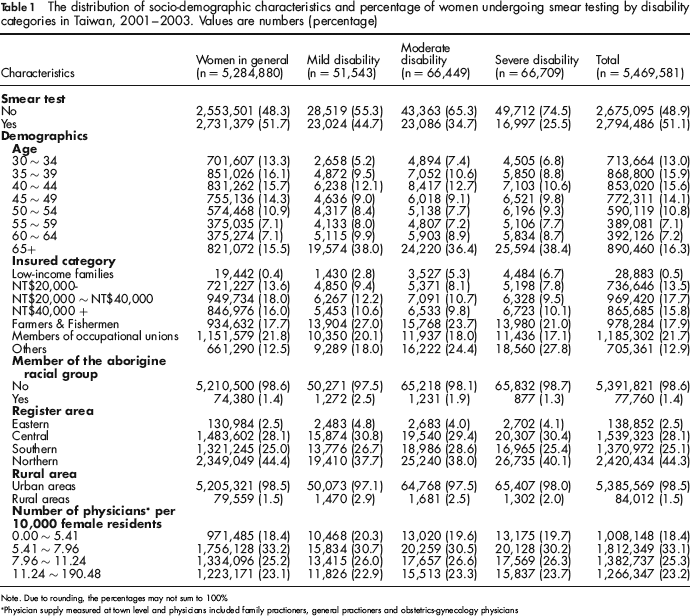
Note. Due to rounding, the percentages may not sum to 100%
Physician supply measured at town level and physicians included family practioners, general practioners and obstetrics-gynecology physicians
Table 2 shows the results of the simple and multiple logistic regression analyses. The simple logistic regression results indicate that women with mild, moderate and severe disabilities were 24%, 50% and 68%, respectively, less likely to have at least one Pap test during the three-year study period than women without disabilities over a similar period. The results revealed a decreasing trend in undergoing a Pap smear test in the three-year period from mild to severe disability. After adjusting for possible confounders such as age, SES, racial group, area of residence and medical resource availability, this dose-response pattern between level of disability and Pap smear testing remained statistically significant. Thus, women with severe disabilities (OR = 0.39; 95% CI: 0.38, 0.39) were still the least likely to undergo a Pap smear test in the three-year period. Compared with all women residing in the lowest physician supply area, all women who resided in the richest physician supply area were 7% less likely to undergo at least one Pap smear test over the three-year period.
Logistic regression analysis relating to receiving Pap smear tests among the wome with different disablility levels and women in general across Taiwan, 2001–2003
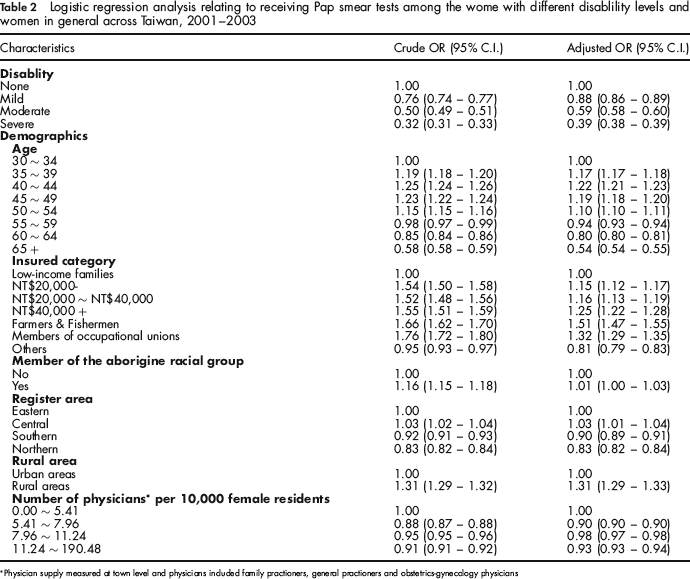
Physician supply measured at town level and physicians included family practioners, general practioners and obstetrics-gynecology physicians
Discussion
This is the first population-based study using claims data to compare the actual Pap smear test screening behaviour of women at various levels of disability with women without disability for an Asian population. The primary finding was that there was a significant inverse relationship between disability and the likelihood of undergoing a Pap test under the NHI programme in Taiwan over the three-year study period. A clear dose-response effect was observed between disability level and likelihood of undergoing cervical cancer screening. Women with disability were less likely to undergo at least one Pap test in the three-year period as recommended by international guidelines. Women with severe disability had the lowest compliance rate. The results are consistent with previous studies conducted in the United States.8–16
There are a number of possible plausible explanations for the lower Pap smear rate among disabled women. Structural and attitudinal barriers may have contributed to the disparities. One reason could be that the health care providers may have the misconception that women with disabilities are asexual and therefore are at little risk of cervical cancer.3,4,8,9 Secondly, a Pap smear test requires the patient to lie on an examination table and this could be difficult for some of these disabled women. 4
Furthermore, as many speculate that increasing physician availability may increase the early detection of cancers,18,20 we examined the relationship between physician availability and routine Pap smear screening. We found that the higher physician availability did not lead to a higher routine Pap smear screening rate. The result differs from the findings of a study conducted by Benjamins et al., which showed that the number of physicians per capita was an important predictor of Pap smear testing utilization. 21 One plausible explanation of the difference may be due to the Integrative Delivery System (IDS) programme in Taiwan. The IDS programme was implemented in Taiwan in 1999 to improve access to health care among rural residents, particularly on preventive care.23,24 The resources or services offered by the IDS programme may not be captured by the proxy measure of per capita physician number. In addition, according to the multivariate analysis result, we found that the disparities observed between women with different disability levels persisted across regions with different physician availability. It suggests that increasing physician availability or the IDS programme alone may not improve routine Pap smear screening among women with disabilities. The disabled women are a unique subpopulation with special needs. For these women, physician availability may not help to modify or reduce structural or attitudinal barriers to a routine cervical cancer screening such as the need for easily accessible transportation and the availability of examination tables. Also, increasing physicians or resources alone may not change women's or providers’ misconceptions. Educational interventions may be more effective in this regard.
There are some potential limitations in this study. First, due to data limitation, no information about disability type was available. Therefore, we were not able to investigate how the various types of disability may have affected the women's decision on receiving routine Pap smear screening.11,12 Future research will be needed to investigate this. Secondly, although we excluded women from our study who had undergone uterectomy since the implementation of the NHI programme in Taiwan in March 1995, we were unable to identify those women who had experienced uterectomy before the NHI programme was implemented due to data limitation. This classification bias may have led to an underestimation of the Pap smear rates in this study. Thirdly, we were not able to identify those who participated in other Pap smear screening programmes. For example, there may be women who used various new screening methods and the effect of this would be to underestimate the Pap smear screening rates in this study.
Despite these limitations, this study makes a unique contribution to the existing literature. First, it confirms that there is a relationship between level of disability and the receipt of preventive services in an Asian population under a universal health insurance coverage system. Second, the large population, which includes an adequate large number of samples, allows this study to achieve sufficient statistical power to detect differences between disability status and physician availability. The findings suggest that increasing physician availability alone may not help to improve women's use of Pap smear tests. Third, the use of computerized administrated data prevented recall bias by the subject affecting the result and it also eliminated the selection effect resulting from the method of data collection. 9 These factors have produced more reliable overall results.
Conclusion
Despite the universal insurance coverage and other social welfare programmes in Taiwan, the proportions of women in Taiwan either with (34.2%) or without disabilities (51.7%) undergoing routine cervical cancer screening were substantially lower than those in the United States (74% and 78% respectively). The national target goal of 2009 set by the Taiwanese government is 58%, whereas the goal of the American Healthy People 2010 is 80%. These comparisons highlight a large gap in routine cervical cancer screening between Taiwan and the United States. As there are more than 0.2 million women with disability in Taiwan and they are at especially high risk of not receiving routine cervical cancer screening compared with women without disability, more efforts are required to close the gap. Increasing the supply of physicians alone may not increase the use of Pap smear testing. Policies and interventions should focus on access to transportation, modified examination equipment and the education of service providers about the special health care needs of women with disabilities. These approaches will help to address the barriers to increasing the use of screening and reducing cervical cancer mortality among women with disability.