
Abstract
Objective
Examination of neonatal hearing screening practices around the world suggests that more attention is placed on infants who fail bilaterally on their hearing screen than infants who refer (fail) in one ear. Some programmes only report bilateral failures as positive hearing screens. This study investigates how limitations of the screening techniques demand continued audiologic evaluations in unilateral referrals.
Setting
The study sample consisted of all infants born at a single academic paediatric hospital between February 1998 and February 2002.
Methods
There were 16,007 infants screened using ALGO automated auditory brainstem response. Eighteen of the infants who failed the screen in one ear but passed in the other ear were found to have permanent hearing loss, and had their subsequent clinical course and audiologic management analysed. The final audiologic outcome after four years in both the pass and fail ear were examined.
Results
One group of unilateral referrals (n = 6) had obvious anatomic reasons for the ear failing the screen (canal atresia/stenosis). There were five patients in which the ear that passed the screen was later found on more extensive audiologic evaluation to have significant hearing loss. Review of recent literature was also completed to examine the methods by which unilateral screening referrals are commonly reported and whether or not this affected follow-up diagnostic evaluation.
Conclusion
Infants who pass one ear and refer one ear on neonatal hearing screening still need to have thorough and prompt evaluations. In many cases, the ear that passed can be found to have significant hearing loss.
Introduction
Despite all of the successes in neonatal hearing screening, patients with unilateral referrals have not received the same attention as those who referred bilaterally. It is traditionally thought that patients with one hearing ear can develop speech and language skills at paces similar to children without hearing loss. Such misconceptions need to be adjusted in light of studies showing that binaural hearing has definite advantages for hearing in noisy environments and localization, 4 and that unilateral hearing loss in children results in increased need for additional educational assistance with a 22% to 35% rate of repeating at least one grade in school. 5
Modern hearing screening equipment targets ears that have > 40 dB hearing loss (poorer than a mild hearing loss). While such setting helps to reduce the number of false positives generated, it takes a toll in the sensitivity of the test. With such limits in sensitivity, it is even more important to execute careful follow-up for all patients who refer on the hearing screen, whether it be unilateral or bilateral. Patients who fail neonatal hearing screening unilaterally may be at risk for hearing loss in the ear that initially passed the screen.
Methods
This is a retrospective review of patients born in Lucile Packard Children's Hospital in Palo Alto, California. Between February 1998 to February 2002, 16,007 infants were screened using the ALGO Newborn Hearing Screener automated auditory brainstem response (A-ABR) system from Natus Medical Inc. The screening was performed by volunteers trained in the use of the device by the director of the screening programme (MP), who has previously described reliable results with extremely low false positive rates. 6 The infant population was drawn from both the well-baby nursery (n = 15,562) and the neonatal intensive care unit (NICU, n = 445). The stimulus delivered had an intensity of 35 dB. Infants who referred in one ear but passed in the other ear were confirmed on an outpatient screen, and their subsequent clinical course and audiologic management were analysed. The final audiologic outcome after four years in both the passed and referred ears was examined and aetiologies determined.
In order to determine current practices on reporting of neonatal hearing screening results, a literature search using Medline and the key words ‘neonatal hearing’ was carried out. The date range was chosen from 2000 to 2007 in order to focus attention on what is being reported in the current literature. The resulting abstracts were reviewed and pertinent articles were analysed. Articles were deemed pertinent to our search when the subject involved neonatal hearing screening and numbers or incidence rates were reported for individuals failing the screen (i.e. referrals). The articles were carefully examined to determine if patients who referred unilaterally were considered failed or passed. When this could not be determined from reading the article, e-mails were sent to the corresponding author for clarification.
Results
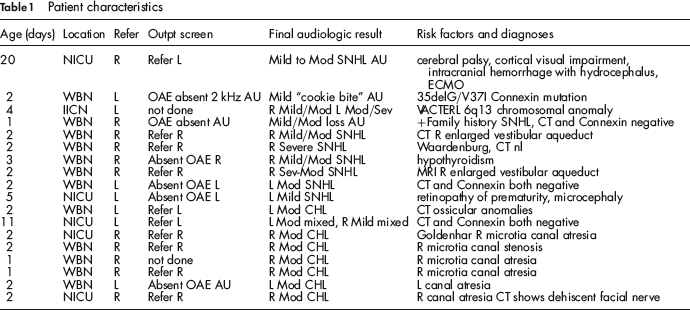
Of the 16,007 infants who were screened in the four-year study period, 18 patients with permanent hearing loss referred unilaterally. The unilateral referral rate was 1.1/1,000 screened. Table 1 summarizes the characteristics of this patient population. During the four years of follow-up, all 18 were found to have at least mild hearing loss in the referring ear. Six of the 18 had obvious unilateral anatomical cause for hearing loss such as aural atresia or severe canal stenosis. Of the remaining 12 patients, 10 had sensorineural hearing loss (SNHL), 1 had conductive hearing loss, and 1 had mixed bilateral hearing loss. Of the 10 who had purely SNHL, four patients were later found to have bilateral loss (Figure 1). Further analysis of the four patients revealed that the ear that passed the screening initially had hearing loss that ranged from mild to moderately severe during later testing. In 3 out of these 4 patients, the pass ear demonstrated audiograms that had a threshold less than 35 dB in at least one frequency (but worse than 35 dB at the other frequencies), which would explain how an ear with moderate to moderately severe loss could still pass the broadband click stimulus used by A-ABR devices. Three out of the four patients referred in the worse hearing ear; however one patient referred in the ear that was later found to be the better hearing ear (i.e. the patient passed in the worse hearing ear).
Flow chart indicating pattern and cases of unilateral referrals on screening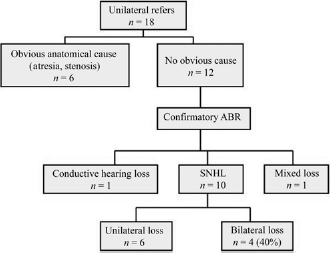
Patient characteristics
Medline search dating from January 1, 2000, using the key-words ‘neonatal hearing’ and limits of English language and Human subjects was performed. There were 69 articles dealing specifically with neonatal hearing screening and reported rates of referrals or failures. Twenty-five articles did not indicate whether unilateral referrals were considered failed or passed, and answers were sought from the corresponding author by email. The final number of articles available for analysis was 66.
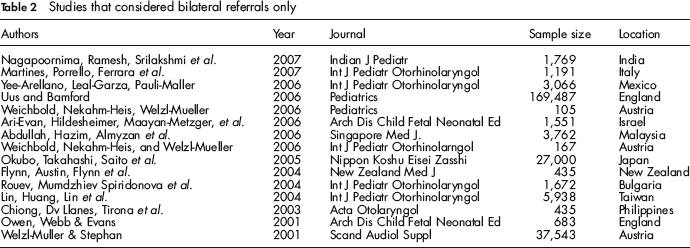
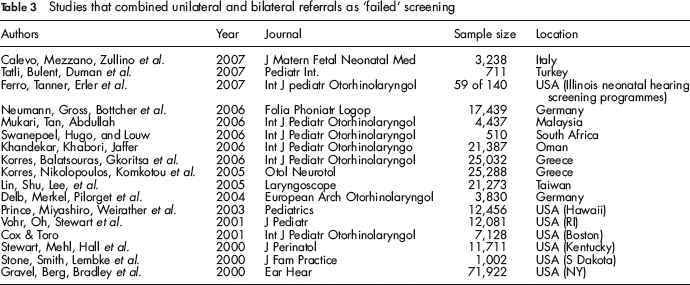
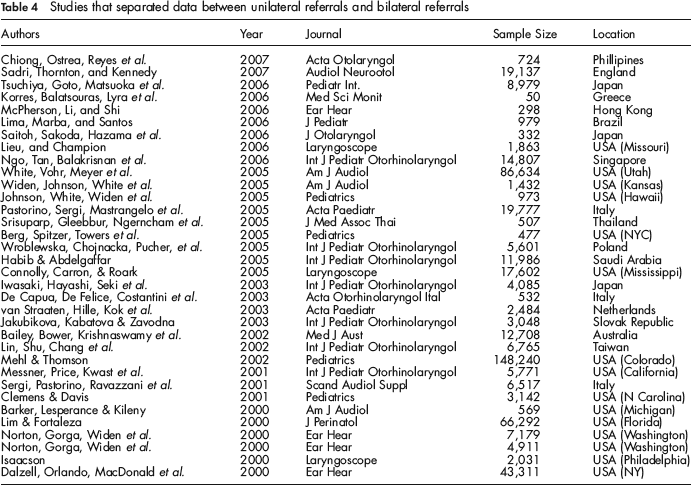
The final analysis revealed three separate categories of articles. Group 1 consisted of 15 articles that only considered bilateral referrals as failures in hearing screens, unilateral referrals were considered to be passes (Table 2); all of these originated from locations outside the USA. Group 2 consisted of 17 articles, and combined unilateral and bilateral referrals into one reported refer rate (Table 3). Group 3 consisted of 34 articles that separated unilateral versus bilateral referrals and demonstrated follow-up for each of the referred ears, rather than the individual infant (Table 4).
Studies that considered bilateral referrals only
Studies that combined unilateral and bilateral referrals as ‘failed’ screening
Studies that separated data between unilateral referrals and bilateral referrals
Discussion
Hearing loss is one of the most common congenital deformities. Approximately 5000 infants with moderate-to-profound hearing loss are born in the United States every year. 7 Depending on the region, overall prevalence of congenital hearing loss ranges from 0.7 to 4.2/1,000 live births. Since Surgeon General C. Everett Koop issued the ambitious challenge in 1988 to have 90% of all infants born with significant hearing loss identified by 12 months of age, the rate of neonatal hearing screening has steadily increased over the years and reached > 90% in the United States by the beginning of 2004. 2
Several technologies are utilized today for neonatal hearing screening. A-ABR and transient-evoked otoacoustic emission (TEOAE) are two of the most popular and are utilized either independently or in combination in 1 or 2 stage fashion. Regardless of the screening method, virtually all programmes are aiming to identify infants who suffer moderate through profound hearing loss only. Consequently, it is likely that all ears with mild hearing loss (up to 40 dB) can be missed by neonatal hearing screening. Such limitation is necessary to reduce the number of false-positives; however, the price to be paid is in test sensitivity. If all ears existed independently of each other, then very little recourse is available to compensate for the loss in sensitivity by lowering neonatal hearing screening threshold. Fortunately, ears are paired structures, and the results of this study suggest that significant hearing loss in one ear may be a risk factor for hearing loss in the opposite ear.
Because many congenital hearing losses are due to systemic causes such as congenital syndromes, maternal drug/disease exposure, or hereditary factors not yet elucidated, it is easy to appreciate the likelihood of simultaneous bilateral effects. But in the era of limited resources, it has sometimes been the practice to assume that children who only referred in one ear have a well functioning opposite ear and therefore require less follow-up. The unilateral referral rate found in this study of 1.1/1,000 screened is similar to those reported in literature (0.4–4/1,000.)8–12 Even though most studies report the rate of unilateral referrals, some of them also report differential treatment of unilateral versus bilateral referrals. For example, in Lieu et al's 2006 study on follow-up of referrals, they clearly stated that prior to 2002, unilateral referrals were not followed up for 12 months whereas bilateral referrals were re-screened in 1–2 months. The article mentioned that such practice in their hospital was stopped by Missouri state government regulation in 2002. 10 For other areas of the world that have yet to have similar government regulation, differential treatment of unilateral versus bilateral referrals persists today.
Our literature search clearly shows that unilateral referrals are not treated in any uniform fashion when studies around the world are examined together. A significant number of studies that originate from areas outside of the USA continue to consider unilateral referrals as ‘passing’ the hearing screen. In fact the largest series available from the United Kingdom by Uus and Bamford went on to explain that ‘the yield figure is significantly lower than demonstrated by most Northern American programmes because the target case for the newborn hearing screening in England does not include unilateral or mild hearing loss.’ 12 These same authors in an earlier publication do quote a bilateral referral rate of 0.85% and a unilateral referral rate of 1.75%, and acknowledge that while unilateral hearing loss has a smaller impact on developmental outcomes than bilateral hearing loss, there is evidence that unilateral losses can result in significant and measurable developmental deficits. 13
Our current study indicates that up to 40% of infants with SNHL who pass neonatal hearing screening in one ear and fail in an ear without external congenital malformations, may actually have bilateral hearing loss. With 9 out of 32 recent articles ignoring unilateral referral in their screening analysis, it is likely a large number of infants who would benefit from early hearing intervention are not receiving the assistance needed.
Conclusion
Unilateral referrals on neonatal hearing screening should be considered a risk factor for significant hearing loss in the opposite ear that initially passes the screen. Therefore patients with unilateral referrals should follow similar diagnostic work-up protocols as those who refer bilaterally.