
Abstract
Objectives
To examine the effect of smoking on three first trimester screening markers for Down's syndrome that constitute the Combined test, namely nuchal translucency (NT), pregnancy-associated plasma protein-A (PAPP-A) and free β human chorionic gonadotophin (free β-hCG) and to use the results to determine which of these markers need to be adjusted for smoking and by how much.
Methods
The difference in the median multiple of the median (MoM) values in smokers compared to non-smokers was determined for NT, PAPP-A and free β-hCG in 12,517 unaffected pregnancies that had routine first trimester Combined test screening. These results were then included in a meta-analysis of published studies and the effect of adjusting for smoking on screening performance of the Combined test was estimated.
Results
The results using the routine screening data were similar to the summary estimates from the meta-analysis of all studies. The results from the meta-analysis were; median MoM in smokers compared to non-smokers: 1.06 NT (95% confidence interval 1.03 to 1.10), 0.81 PAPP-A (0.80 to 0.83) and 0.94 free β-hCG (0.89 to 0.99). The effect of adjusting for smoking on the Combined test is small, with an estimated less than half percentage point increase in the detection rate (the proportion of affected pregnancies with a positive result) for a 3% false-positive rate (the proportion of unaffected pregnancies with a positive result) and less than 0.2 percentage point decrease in the false-positive rate for an 85% detection rate.
Conclusion
Adjusting first trimester screening markers for smoking has a minimal favourable effect on screening performance, but it is simple to implement and this paper provides the adjustment factors needed if a decision is made to make such an adjustment.
Cigarette smoking in pregnancy influences levels of serum markers used in screening for Down's syndrome, although there is no evidence of an association between the birth prevalence of Down's syndrome and smoking. 1
In the early second trimester of pregnancy, human chorionic gonadotrophin (hCG; total hCG and the free ß subunit) and inhibin-A are materially influenced by smoking. The median total hCG multiple of the median (MoM) in smokers has been estimated to be 0.822 (18% lower than non-smokers), the median free β-hCG MoM to be 0.80 (20% lower than non-smokers), and the median inhibin-A MoM to be 1.62 (62% higher than non-smokers). 1 Alphafetoprotein and unconjugated oestriol are less influenced by smoking, with median MoM values in smokers of 1.05 and 0.96, respectively. Adjusting for smoking can be simply achieved by dividing a smoker's observed MoM value for a particular marker by the median value of that marker in smokers. 1
In the late first trimester, two serum markers, free ß-hCG and pregnancy-associated plasma protein-A (PAPP-A) and an ultrasound marker, nuchal translucency (NT), measured between about 11 and 13 weeks of gestation constitute the Combined test. Published studies have shown a lower free ß-hCG median MoM in smokers than non-smokers with estimates ranging from no difference to 13% lower, 3–7 lower PAPP-A levels with median MoM values ranging from about 15% to 25% lower in smokers 3–7 and higher NT values ranging from no difference to 16% higher in smokers. 3,5,7,8 The range of estimates prompted us to examine the levels of these first trimester markers in our own data and include these in a meta-analysis of published results to provide more precise estimates of the effect of smoking than is possible from the results of individual studies.
Measurements of free ß-hCG, PAPP-A and NT, together with a record of smoking status were collected on 12,517 unaffected pregnancies as part of routine first trimester Combined test screening at the Wolfson Institute of Preventive Medicine between 1 January 2003 and 30 September 2007. There were too few in women who smoked and also had an affected pregnancy with Down's syndrome to investigate the effect of smoking on screening markers in affected pregnancies. In our data, approximately 8% of women smoked, with Caucasian women most likely to smoke (8.8%) followed by Afro-Caribbean women (7.7%), Oriental women (2.3%) and women of South Asian origin (1.1%). Smokers were, on average, younger (32 versus 35 years of age at expected date of delivery), had first trimester screening at the same gestational age (88 days) and, contrary to previous observations, 5 smokers were on average the same weight as non-smokers (68 kg). This may have been due to the general decline in smoking over time being less evident in certain groups such as the relatively poor and overweight.
Table 1 shows the median MoM value for the three markers according to smoking status, with the median MoM in non-smokers set to 1.00 for each marker. The median PAPP-A MoM in smokers was 20% lower than that in non-smokers (P < 0.001). The median free β-hCG MoM was 4% lower than non-smokers and the median MoM for NT was 3% higher in smokers, both small differences, but nonetheless statistically significant (P = 0.011 and P < 0.001, respectively). The standard deviations for each marker were similar in smokers and non-smokers. As previously found, there was a minor statistically significant dose-response relationship in our data for PAPP-A 7–9 , but most of the effect was between smokers and non-smokers and the dose response relationship was not clinically useful (the median MoM in women who smoked a few cigarettes per day was only marginally higher than in heavy smokers).
Median free β-human chorionic gonadotrophin (β-hCG), pregnancy-associated plasma protein-A (PAPP-A) and nuchal translucency (NT) multiple of the median (MoM) values measured at 10 to 13 weeks gestation in smokers compared to non-smokers (median set to 1.00 MoM)
*P = 0.01
† P < 0.01
Figure 1 shows the results of a meta-analysis for each marker (including our current results with those previously published) using a random effects model, 10 again setting the median MoM in non-smokers to 1.00. For each marker, studies that did not provide an estimate of the standard deviation in smokers were assigned the pooled estimate for that marker. 4,8 The summary estimate for PAPP-A was a median MoM of 0.81 in smokers (19% lower than non-smokers), close to our estimate of 0.80 MoM. The summary estimate for free ß-hCG was 0.94 MoM (6% lower) and for NT was 1.06 (6% higher), also both close to our estimates of 0.96 and 1.03, respectively. For each marker, the median MoM in smokers was statistically significantly different from the median value in non-smokers (1.00 MoM).
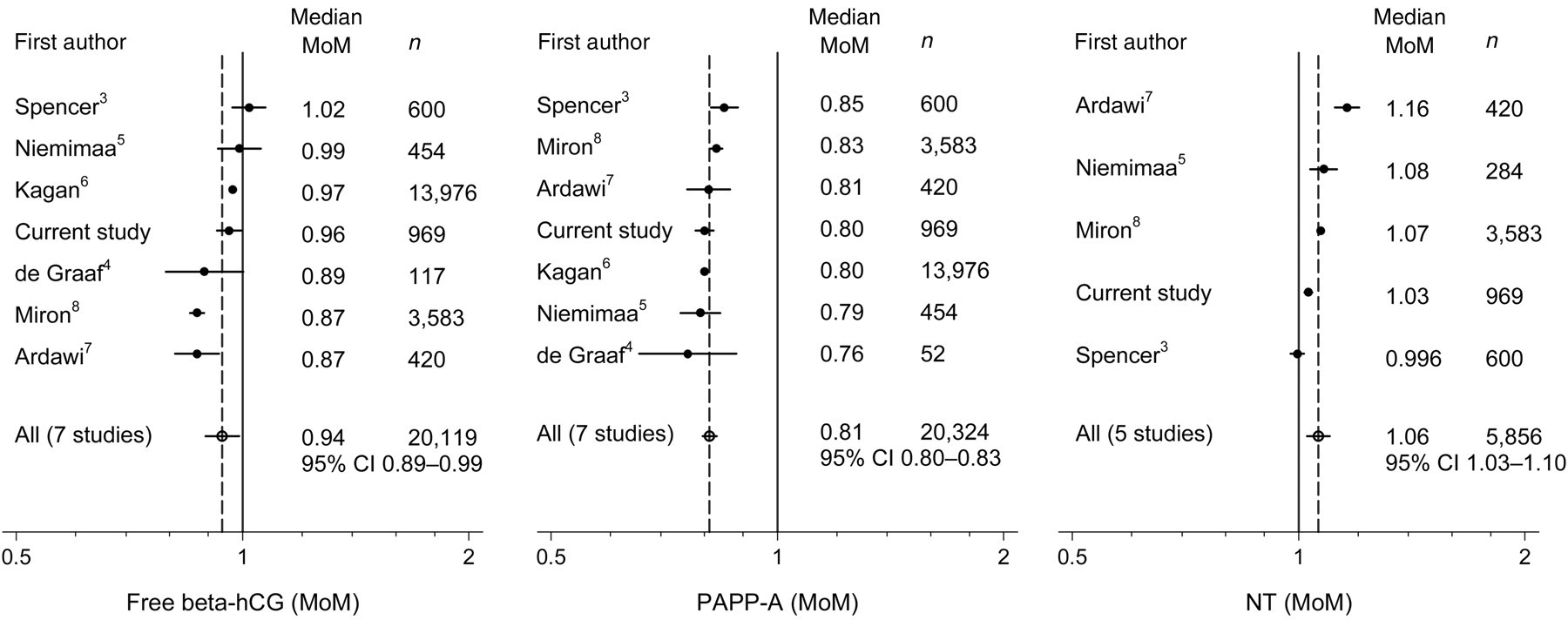
Published studies of free β-human chorionic gonadotrophin (free β-hCG), pregnancy-associated plasma protein-A (PAPP-A) and nuchal translucency (NT) measured at 10–13 weeks gestation in pregnancies of women who smoke compared to women who do not smoke, showing the median multiple of the median (MoM) value and number of pregnancies in each study, together with a pooled estimate of the median with 95% CI and the median in non-smokers (solid line, median set to 1.0 MoM)
Among women screened at the Wolfson Institute the Combined test false-positive rate was 8.6% (1,058/12,517), close to the 8.9% expected on the basis of the age distribution of the women screened and ignoring their smoking habits (using a 1 in 250 term risk cut-off). The false-positive rate in smokers was 11.1% (108/969), statistically significantly higher than the false-positive rate in non-smokers (8.4%, 969/11,558 P = 0.003).
Table 2 shows the predicted effect on the detection and false-positive rates of the Combined test with and without adjustment for smoking (using the results from the meta-analysis) according to the prevalence of smoking (10%, 20% and 30%) and without. Modelling was performed by simulation and with adjustments to marker MoM values for smoking as previously described. 1,11 The effect of adjusting for smoking is small with no more than a half percentage point increase in the detection rate for a 3% false-positive rate and no more than a 0.2 percentage point decrease in the false-positive rate for an 85% detection rate. At a fixed risk cut-off of 1 in 250, adjusting for smoking results in a small decrease in both the detection and false-positive rates. Similar modelling applied to the Integrated test (first trimester NT, PAPP-A and second trimester AFP, uE3, hCG and inhibin-A) showed a similar marginal improvement in screening performance, using the adjustment factors taken from these results and those previously published. 1
Screening performance of the Combined test (markers measured at 11 completed weeks gestation) adjusting marker MoM values for smoking and without adjusting for smoking according to prevalence of smoking. Detection rate (DR) for a 3% false-positive rate (FPR), FPR for an 85% DR and DR and FPR for specified risk cut-off
Whilst adjusting MoM values in smokers has a negligible effect on the overall screening performance, this paper provides the adjustment factors needed if a decision is made to adjust first trimester screening markers for smoking.