
Abstract
This literature review is a comprehensive summary of premarital (prenuptial) screening programmes for the most prevalent hereditary haemoglobinopathies, namely thalassaemia and sickle cell disease, and the important infections HIV (human immunodeficiency virus) and hepatitis viruses B and C (HBV and HCV). It describes the background to premarital screening programmes and their value in countries where these diseases are endemic. The use of premarital screening worldwide is critically evaluated, including recent experiences in Saudi Arabia, followed by discussion of the outcomes of such programmes. Despite its many benefits, premarital testing is not acceptable in some communities for various legal and religious reasons, and other educational and cultural factors may prevent some married couples following the advice given by counsellors. The success of these programmes therefore depends on adequate religious support, government policy, education and counselling. In contrast to premarital screening for haemoglobinopathies, premarital screening for HIV and the hepatitis viruses is still highly controversial, both in terms of ethics and cost-effectiveness. In wealthy countries, premarital hepatitis and HIV testing could become mandatory if at-risk, high-prevalence populations are clearly identified and all ethical issues are adequately addressed.
Premarital Testing for Thalassemia and Sickle Cell Disease
Introduction
The prevalence of inherited blood disorders in certain parts of the world is high, including the autosomally inherited haemoglobinopathies, thalassaemia and sickle cell disease. Premarital screening aims to identify carriers of the haemoglobin disorders, in order to assess the risk of having children with a severe form of disease. The couple can then choose whether or not to have an affected child.
Improved healthcare and management means that the numbers of thalassaemic patients and their life expectancy are increasing, and this places extra demands on healthcare systems, meaning that some countries are unable to deliver optimum treatment to all their affected patients. Effective prevention can maximize the available resources if it is instituted properly, preventing up to 95% of affected births. 2 Healthy carriers of beta-thalassemia can be identified inexpensively and accurately by a simple blood test. Couples who undergo testing can be informed about genetic risks and given options for reducing risk, including prenatal diagnosis. 2
History of premarital screening for thalassaemia and sickle cell disease
Premarital thalassaemia screening was first carried out in 1975 by Silvestroni and colleagues 3 in Latium, Italy, as part of a school prevention programme. Screening for sickle cell anaemia began before this, in Virginia in 1970. 4 Nationwide screening programmes also began in Canada, Cyprus, Greece, Italy and the UK during the 1970s, with proven success 5 (see Table 1). Until this point, the genetic causes of hemoglobinopathy were understood, but little had been done to prevent them in newborns. 18
Countries with known premarital screening programmes
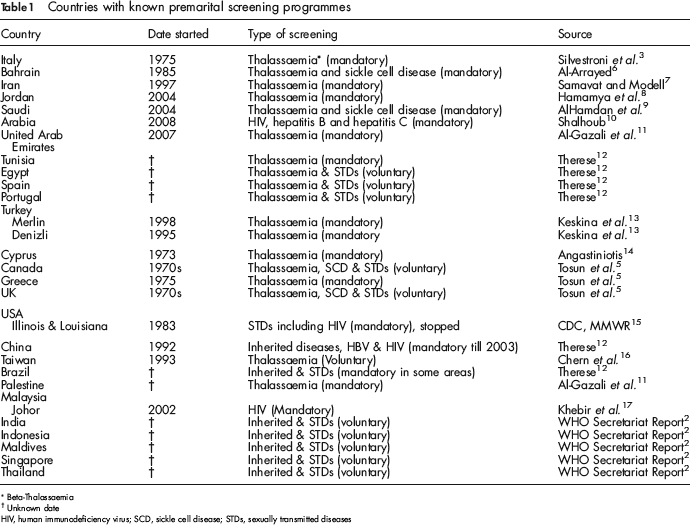
Beta-Thalassaemio
Unknown date
HIV, human immunodeficiency virus; SCD, sickle cell disease; STDs, sexually transmitted diseases
Angastiniotis and Modell
20
classified countries who deliver premarital screening programmes into three categories:
Endemic Mediterranean countries in which preventive programmes are long-established, with success rates (preventive) of 80–100% and optimum treatment via specialist clinics. Developed, industrialized countries in which prevalence is increasing because of migration; these countries can fund screening programmes, but find it difficult to reach immigrants with certain cultural backgrounds. Developing countries in which there are economic difficulties and other health priorities (e.g. infectious disease control), or other religious and cultural constraints
20
(see later).
In Cyprus, Greece and Italy, premarital screening for thalassemia has been normal practice for a long time because consanguinity is high. Similar preventive programmes have been introduced in Bahrain, China, India, the Islamic Republic of Iran, Indonesia, Malaysia, the Maldives, Singapore and Thailand, and recently in Saudi Arabia and United Arab Emirates. In the UK, Northern Ireland and other northwest European countries, prenatal diagnosis is available and abortion is a prevention strategy. 2
In China, couples who wish to marry are extensively tested, including physical examination. They are given premarital health instructions and ‘counselling’ – in the form of watching videotapes of the type of child they might conceive – after which appropriate measures are taken. This approach has been strongly criticized in terms of human rights, control, oppression and eugenics, even though the value of vigilant premarital screening is acknowledged. 21
In Lebanon, thalassaemia patients are managed in chronic-care centres in collaboration with the ministries of Social Affairs and Public Health. Their screening programme includes providing information, training health professionals and developing training materials, with priority given to disseminating knowledge and increasing public awareness. 22
Tosun et al. 5 studied the premarital haemoglobinopathy screening programmes in Mersin, Turkey, where consanguinity is 30%. If the man and the woman are both carriers, results are given confidentially and they are counselled about their options, including prenatal diagnosis.
In Saudi Arabia, premarital testing for haemoglobinopathies is mandatory. 9 The results of at-risk couples are treated in the same way as in Turkey. Prenatal diagnosis is not offered, however, as discussed later. 9
Role of culture and education in the success of screening programmes
‘Consanguinity’ refers to relationships by blood or common ancestry, in which the chances of offspring inheriting a recessive allele for a disease are increased; the closer the relationship, the greater the risk. Marriages between members of the same tribe or extended family group are favoured in some cultures, including those between first cousins. Consanguineous marriages are uncommon in Western countries. Marriage between first cousins is forbidden by the Orthodox Church and Roman Catholic Church, and may be seen as incestuous in the United States.
Personal characteristics including socioeconomic status have implications for the outcome of premarital screening programmes. Education of the couples who are to be screened is extremely important and it is essential to educate all members of the screening team (laboratory technologists, nurse practitioners, physicians, counsellors, outreach workers and social workers). According to Schmidt, 23 ‘sufficient planning in the educational area before the first blood sample is drawn can avoid failures of the programme.’ The meaning of the term ‘carrier status’ should be made known to members of the public long before they get married. For successful public education, governments and government organizations must cooperate, as well as community and religious leaders, school parent organizations and health personnel. 5
A study by Eshra and colleagues 24 based in Egypt revealed gaps in knowledge regarding premarital screening, even among educated people. These people acquired their knowledge from the mass media and medical personnel. People who responded to information about premarital screening had favourable attitudes towards premarital counselling and examination of consanguineous marriages, possibly relating to social changes, declining illiteracy, increasing economic pressures, increasing numbers of nuclear families and longer waiting times before starting a family. 24 People with a negative attitude towards these tests were mostly unmarried males. Eshra and colleagues 24 therefore suggested that education programmes about the benefits of premarital examination should target unmarried males, so they can make informed choices about unmarried females and consanguineous marriages.
Religious beliefs restrict the success of screening programmes in some communities. In Southern Iran, premarital screening has been mandatory for 10 years, yet high-risk couples still get married and give birth to children homozygous for beta-thalassaemia. Often this is because of religious and traditional cultural restraints 25 ; in the case of Islam, consanguineous marriages are permitted, so thalassemia persists in some parts of the community, making the programme redundant. 25
Some people believe that their fate is determined by God and therefore accept the risk of having a sick child. A recent report in The Jordan Times 26 showed that many Jordanians view the results of their ‘unions’ as fate. One interviewee stated: ‘All my ten children are disabled; they will get their reward in heaven’. On the contrary, there are many teachings in Islamic culture that promote healthy marriage and the role of counselling. 27
AlKhaldi et al. 28 evaluated the attitude of health-science students in Saudi Arabia towards premarital screening and counselling. Most students had a positive attitude, but around 25% refused testing and counselling according to their interpretation of Islamic principles. Awatif 29 studied attitudes among female students in King Saud University, discovering that 86% of them felt positively about premarital testing. El-Hazmi 30 assessed attitudes in a community-based study and found 94% of participants considered premarital testing and counselling to be important in preventing genetic blood diseases; 87% thought testing should be mandatory. The Saudi community clearly shows awareness of premarital testing and its value; however when AlHamdan et al. 9 studied the outcome of the first 2 years of the Saudi screening programme, they found that about 90% of high-risk couples still got married despite knowing their risk of having a sick child. This undermines the high level of awareness identified in other studies. One possible explanation is that both AlKhaldi et al. 28 and Awatif 29 focused on the opinions of university students and El-Hazmi's community study 30 was among university students and people attending scientific meetings and health centres. None of these studies was truly representative of the Saudi population as a whole and therefore the results cannot be generalized.
Reports by Karimi et al., 25 Monaghan 26 and AlKhaldi et al. 28 were from three different Islamic countries, and all three provided evidence that religious beliefs could be obstacles to the success of premarital screening programmes, regardless of other factors such as education level. The same conclusions were reported long ago in other (non-Muslim) communities. In 1981, Angastiniotis and Hadjiminas 14 stated that support from the Church was the main reason for the success of screening programmes in Cyprus and Greece.
Counselling
Genetic counselling is the process by which an individual or a family obtains information about a genetic condition that may affect them, so that they can make appropriate decisions about marriage, reproduction and health management. 27 Genetic counselling protects the autonomy of the couple, fulfilling their right to be fully informed about the disorder and all available options. 2 Although premarital tests for haemoglobinopathies are reliable and useful, not everyone with these genes responds to counselling. Neal-Cooper and Scott 4 reported that young couples’ concerns about producing a child with sickle cell disease are often offset by their strong desire to have children regardless of risk. The researchers suggested that at-risk couples should be contacted directly by counsellors and encouraged to undertake education and counselling.
Prevention and treatment of genetic diseases is virtually impossible. 1 Studies of patient perspectives about premarital examinations reveal a need for physicians to offer counselling for various health problems before the patient asks, so they can turn down unwanted help rather bring up sensitive issues. 31 Screening programmes that inform about the risks associated with child bearing should be performed well before child-bearing age. Unfortunately, premarital screening often comes too late for couples to change their opinions about marriage based on their haemoglobin phenotype, because by this point they are already committed to their relationship. Furthermore, it may be ‘taboo’ for a woman to reject marriage for these reasons, and it may affect her social life, preventing her from ever getting married.
One successful approach is ‘solution-focused’ premarital counselling. Murray and Murray 32 discuss how this focuses on a couple's resources, helping them to develop a shared vision for the marriage. Background information about premarital counselling and solution-focused therapy provide a framework in which intervention strategies in those confirmed with positive status for a disease can be developed. These solution-oriented interventions include solution-oriented questions and feedback, as well as a Couple's Resource Map (CRM) which depicts the support available to the couple from various personal, relationship and contextual resources. 33 The available choices include avoidance of marriage, reproductive options for those who proceed with the marriage following prenatal diagnosis, adoption of the affected child, donation of sperm, ova or a pre-embryo from an unaffected individual, and pre-implantation diagnosis. 26 Choosing the best option depends on availability, cost, and local regulations and religious rules. For example, in Saudi Arabia adoption of children is prohibited on religious grounds and prenatal diagnosis is useless because abortion is forbidden unless the fetus is malformed. However, pre-implantation diagnosis is permitted and affordable.
Thus the success of genetic counselling depends on the approach adopted by the counsellor as well as the education and attitude of the couple. Screening programmes must be equitable, accessible and understood by the target population, but most importantly they must comply with the prevailing cultural, ethnic, economic and societal values.
Premarital testing in Saudi Arabia and other Arabian countries
Genetic and congenital disorders are common in Arab countries, contributing greatly to infant mortality and morbidity. Common among these diseases are the haemoglobinopathies and glucose-6-phosphatase deficiency. 11 In the first half of the twentieth century, the governments of countries like Egypt, Syrian Arab Republic, Lebanon, Tunisia, and Morocco began promoting optional premarital examinations. To begin with, there were no methods for detecting disease carriers, so hereditary diseases and consanguinity were little affected. Medical certificates were often provided without complete medical check-ups. 34 As detection became possible, the burden of screening was taken up by the Governments of Egypt, Lebanon, Bahrain, Saudi Arabia and United Arab Emirates in order to establish appropriate screening techniques and policies.
Premarital screening is essential for changing attitudes towards consanguineous marriage 35 particularly in places where consanguineous and ‘tribal’ marriages are common, resulting in a high incidence of genetic disorders. 36 Such marriages are rare in Western societies, often restricted by civil legislation and religious beliefs 37 but it has been estimated that 25–60% of all marriages in Arab regions are consanguineous, 11 with a high incidence of first-cousin marriage. In fact, marriage within ‘the family’ is encouraged in many parts of Asia and Africa and the east-Mediterranean region, which is mainly occupied by Arabs and Muslims for whom religious considerations are of paramount importance. 38 This is why it is so important to examine the options for prevention and management of genetic disorders and their ethical and (country)-policy-related implications.
In 2004, the Saudi Arabian Government implemented compulsory premarital screening aimed at decreasing the incidence of haemoglobinopathies. It was implemented by the Ministry of Health, which is responsible for providing free health care to the entire population, and the decision to make testing mandatory was based on discussions with numerous technical, religious and social organizations. Currently, there are over one hundred health reception centres, 70 blood-testing laboratories and 20 genetic counselling and education clinics in the country. Both screening and counselling are free of charge. A specialist centre in Riyadh, in association with King Faisal Specialist Hospital, trains all the health personnel who work on the programme. The carefully formulated guidelines are regularly updated. 9
AlHamdan and colleagues 9 assessed the premarital screening programme two years after it became mandatory. Everyone in Saudi Arabia had good access to the programme. High prevalence of carrier status was reported predominantly in the eastern and south western regions of the country, but (as mentioned above) 90% of couples detected as carriers did not follow the advice they were given and went ahead with their marriages. This result requires evaluation and revision of the programme by the Saudi health authority in order to achieve its goals as AlHamdan said.
Premarital Screening of HIV, HBV and HCV
Epidemiology of HIV, HBV and HCV
Currently, there are about 4.1 million people with HIV infection worldwide; 95% of them are in developing countries, generally in sub-Saharan Africa and Southeast Asia. 39 Approximately 1.8 billion people have serologic evidence of HBV infection and 350 million have a chronic infection. At least 500,000 of them die of liver malignancy and cirrhosis. 40 The World Health Organization (WHO) estimates 170 million people around the world are infected with HCV. 41 Prevalence varies widely, with Egypt having the highest of 22%. Healthy blood donors reveal infection rates of 0.01–0.02% in the UK and northern Europe, 1–1.5% in southern Europe, and 6.5% in parts of equatorial Africa. 41 According to the Centres for Disease Control and Prevention, 1.8% of the US population is positive for anti-HCV, with 8000–10,000 deaths each year caused by HCV infection. 41 Unfortunately, information about the prevalence of these diseases among the specific target groups is not available.
In 2004, the Saudi Ministry of Health announced the total number of HIV carriers was about 11,000, of which 2005 were Saudis, giving a prevalence of about 0.011% for the Saudi population (18 million). Estimates for the prevalence of HBV and HCV in young Saudi adults are available, but not specifically for the group targeted by screening programmes. El-Hazmi 42 found prevalence rates of 1.4% for hepatitis B surface antigen (HBsAg) and 0.2% for anti-HCV among Saudi blood donors in Riyadh, and prevalences of 2.0% and 1.6%, respectively, among non-Saudi blood donors. Another study by Bashawri and colleagues 43 found a steady decrease in HBsAg (from 2.58 to 1.67%) and anti-HCV (from 1.04 to 0.59%) in the Eastern region among blood donors between 1998 and 2001. However, Saudi Arabia began mandatory premarital screening for hepatitis B and C viruses and HIV in the beginning of 2008. 10 Adding these new tests to the Saudi mandatory premarital screening programme means that about a quarter of million individuals must undergo HIV, HBV and HCV testing annually 10 , which is not cost-effective due to the low prevalence of these diseases – especially HIV. As a Saudi citizen, the author of this paper appreciates the rationale for adding these new tests, namely the massive public and media pressure on the government. At the time of writing, however, the current programme has been running for less than a year, and no formal reports have yet been released. This programme will definitely enable the Saudi health authority to clearly estimate the epidemiologic indicators for these infections or any other health problems among Saudis in the future.
The need for premarital screening of HIV, HBV and HCV
Heterosexual sex and perinatal transmission can affect the fetus, resulting in infections of the newborn. Newborns infected with HIV will eventually develop AIDS (acquired immunodeficiency syndrome). Although detection of HIV in the mother and providing anti-HIV therapy is common, success rates are unclear and there are financial and medical constraints. In Belarus, Kazakhstan, the Republic of Moldova, the Russian Federation and Ukraine, massive outbreaks have been reported among injecting drug users. Transmission of HIV to non-injecting sexual partners occurs, as well as recipients of blood and other tissues, thus increasing overall prevalence. Hepatitis viruses (HBV and HCV) are also transmitted among drug users; in fact, hepatitis epidemics among drug users do precede HIV infection. Prevalence of HCV in injection drug users is far greater than HIV, indicating that HCV has greater transmissibility via blood. 44
Perinatal hepatitis is not always symptomatic but there is a high risk of infection becoming chronic, and there are only a limited number of medications for treating HBV and HCV infections. An effective vaccine for HBV is now available, 45 forming an essential part of vaccination programmes around the world.
These important infections are a heavy financial burden for health services. In the US, annual costs associated with the treatment of HCV infection alone exceed $600 million. 41
Evaluation of screening programmes for HIV in various countries
Sexual and vertical (from mother to fetus) modes of transmission of HIV are well known; therefore the WHO recommends voluntary screening programmes together with counselling and education services in countries with high HIV prevalence rates. 44 Several studies have examined the acceptability and benefits of these screening programmes, revealing important issues, both negative46–48 and positive17,49,50 as described below.
Negative aspects of the screening programmes
Mandatory premarital screening for these infections would involve assessing many new couples each year, with huge financial implications. 46 Petersen and White 48 evaluated HIV seroprevalence premaritally in eight areas of the US; with rate estimates of 0.4% in women and 0.1% in men. These rates were much higher than those obtained by routine tests among blood donors. They also found that the number of marriage licenses issued was not greatly affected, and concluded that mandatory premarital screening would be more expensive than other HIV prevention programmes, and have a limited impact on the epidemic. These findings concur with those of an earlier study 46 in which public education, counselling and discretionary testing reduced the spread of HIV infection more effectively than premarital screening. Petersen and White 48 proposed some more economical and effective alternative strategies: testing HIV status in pregnant women and treating affected fetuses, and increasing the availability of drug treatments to high-risk groups like intravenous drug users.
Turnock and Kelly 47 evaluated mandatory premarital HIV testing in Illinois (there was only one other similar programme in the US, in Louisiana; both were discontinued within 2 years). 51 This enforcement generated many legal concerns, not least regarding the infringement of fundamental liberty, the right to marry and the implications of involuntary withdrawal of blood. 52 The study concluded that these mandatory tests were not a cost-effective way to control HIV infection; the cost of running the programme for 6 months was $2.5 million (or $312,000 per seropositive person). The number of marriage licenses issued in Illinois decreased by 22.5%, but the number of licenses issued to Illinois residents in surrounding states increased significantly, meaning some couples moved to other states to marry. 53
Positive aspects of the screening programmes
Altman et al. 50 conducted a study to determine the effectiveness of premarital testing in New Jersey, USA. They found that seroprevalence in unmarried couples was 0.55–0.62%, much more than other earlier estimates. Therefore they recommended voluntary HIV-1 testing and counselling for marriage applicants.
Some studies show mandatory premarital testing to be cost-effective; in the US, McKay and Phillips 49 predicted savings of $70,000 to $127,000 for every case of HIV infection prevented. They found a statistically significant cost-benefit ratio of between 3.1 and 28.2 in many scenarios.
Khebir et al. 17 evaluated a premarital screening programme in Johor State (Malaysia) over 3 years. They reported a positivity rate of 0.17% for premarital screening compared with a positivity rate of 0.05% for antenatal screening. The number of marriage applications actually increased and public awareness of HIV was raised, thus improving the chances of early detection. This programme uses a newer, rapid and cheap but highly sensitive and specific screening test (SD Bioline HIV-1/2 3.0; Standard Diagnostics Inc. Kyonggi-do, South Korea) and the screening and confirmatory tests are free to the public.
Adibi et al. 40 assessed the economics of preventing HBV transmission in unmarried people in Iran, where cultural influences are strong and HBV infection is endemic. They reported that premarital HBV testing is cost effective.
Factors influencing the success of screening programmes for HIV, HBV and HCV
Although the prevalence of these infections seems to be the most important factor when implementing screening programmes, the country's resources, availability of medical care, education, and public awareness are also important. Some international associations (e.g. Bill Clinton HIV Initiative and the United Nations AIDS programme) have suggested that HIV screening should be mandatory in countries with prevalence of 5% or more. 54
In regions where the prevalence of HIV, HBV and HCV is high, knowledge about the diseases and uptake of voluntary counselling and testing is low. 55 This is probably because these infection rates are greater in developing and underdeveloped countries where literacy and levels of understanding are low. Culture and individual attitudes also have a role in the success of testing.55–57 Iliyasu et al. 55 reported that knowledge of HIV in Nigeria is low, especially in rural areas, even though it has the third highest population of people living with HIV. Many Nigerians did not know the cause of AIDS or the modes of transmission, and those who knew about the disease rejected voluntary counselling and testing because of misconceptions and fear, gaps in knowledge and limited access to the services. Formal education, female gender and HIV knowledge predicted a positive attitude.
The impact of culture cannot be underestimated. Luginaah et al. 56 reported that HIV testing has a far-reaching social impact, especially for people planning to marry, which extends beyond individuals and couples in certain communities where values may clash with the concept of premarital HIV testing and there are issues of confidentiality.
Other than Saudi Arabia, only China implements mandatory premarital testing for HBV and this is because the prevalence of HBsAg carriers is high (10%). 12 Mandatory premarital screening for HCV is only reported in Saudi Arabia as well. 10
Routine testing for the hepatitis viruses and HIV is undertaken by many countries, but usually before blood donation, before surgical procedures, in people who are admitted to hospital and in prisoners. Mandatory pre-military recruitment and pre-employment screening are now common. When Adibi et al. 57 evaluated the attitudes of young adults in Iran towards premarital HBV screening, male sex and higher education level were associated with more positive attitudes. They inferred that a universal premarital HBV screening programme would be highly acceptable in Iran.
Conclusion
Thalassemia and sickle cell disease are common, incurable, autosomal recessive inheritable haemoglobinopathies that cause significant morbidity and mortality and impose a heavy financial burden on society. A simple blood test before marriage can easily detect carriers of these diseases, to inform couples about their chances of producing affected children and ensure they receive appropriate advice. Since their introduction in the early 1970s, some premarital screening programmes have become widely accepted and highly valued in preventive healthcare, so much so that many countries have made them mandatory. Their value to public health is widely acknowledged.
Yet, not all screening programmes have shared this degree of success. Some very strong social factors influence the acceptability of preventive programmes, not least among them religious beliefs, cultural norms, traditions, literacy and education level, government policies and the attitudes of individual couples. For mandatory infection screening programmes to be successful, every one of these factors needs to be addressed. Experiences from some Islamic countries indicate that the way in which some individuals misinterpret their religion creates a significant obstacle to the success of screening programmes in Muslim communities.
HIV and hepatitis infections are now prevalent in epidemic proportions and are easily transmitted to sexual partners and to newborns. They are not curable, and mortality and morbidity rates are high. For these reasons alone, they are strong candidates for inclusion in premarital screening programmes. Currently, routine screening for these important viral diseases is mainly conducted among blood and tissue donors. The situation is only changing slowly. China and Saudi Arabia have started premarital screening for HBV and Iran is considering including it as part of its own premarital screening programme. Mandatory premarital screening for HIV is a different issue altogether. It has been tried in some countries, such as the USA, Malaysia and Saudi Arabia, but with very limited success in USA. Enforcement is still highly controversial, and raises serious ethical and cost-effectiveness issues. More outcome data from Malaysia and Saudi Arabia, among other countries, will do much to increase the body of evidence on these matters.
In developed and committed countries, mandatory premarital screening does have the potential to succeed as long as the target population is clearly identified and all ethical issues (including confidentiality of the results), religious, cultural and human rights and concerns about proper post-diagnostic management are fully addressed.
Footnotes
Acknowledgements
We are grateful to the journal's reviewers for their valuable comments which guided the revision of the manuscript.