
Abstract
Objectives
To examine sociodemographic predictors of self-reported screening attendance, intention to accept human papillomavirus (HPV) testing and willingness to accept vaccination for a daughter under 16.
Setting
Home-based, computer-assisted interviews with a population representative sample of British women.
Methods
Participants were selected using random probability sampling of the Postcode Address File, 994 women aged 25–64 were included in these analyses. Women reported their attendance at cervical screening and intention to accept an HPV test. A subsample of those with a daughter under 16 years (n = 296) reported their willingness to accept HPV vaccination for their daughter.
Results
Screening attendance was associated with education level (odds ratio [OR] = 1.66, confidence interval [95% CI]: 1.07–2.56) and being married (OR = 2.04, 95% CI: 1.37–3.03). Acceptance of HPV testing was predicted by regular attendance for cervical screening (OR = 1.58, 95% CI: 1.03–2.42) and being from a white background (OR = 2.20, 95% CI: 1.18–4.13). Daughter's age was the only predictor of HPV vaccine acceptance, with mothers whose youngest daughter was 13–16 years old being the most likely to accept vaccination (OR = 2.91, 95% CI: 1.27–6.65).
Conclusion
In contrast to screening attendance, ethnicity plays an important role in HPV testing. Specific cultural barriers should be identified and addressed to ensure ethnic disparities in testing are limited. While marital status is associated with screening attendance, HPV testing could overcome this bias. Sociodemographic variables seem to play a limited role in HPV vaccine acceptance among mothers making vaccine decisions for their daughters, but as with other studies, age of daughter is important. The scientific reasons for vaccinating at 12–13 years should be emphasized in HPV information.
INTRODUCTION
In the UK there are around 2800 new cases of cervical cancer each year, accounting for 1% of all cancers. 1 This low prevalence is largely due to the success of the cervical screening programme, which has been estimated to prevent around 80% of cervical cancer deaths. 2 However, cervical screening is not without costs; particularly in relation to worry and discomfort associated with an abnormal result. 3 There is also concern about socioeconomic disparities in regular screening participation, which could be contributing to differences in rates of cervical cancer. 1 Although some studies have failed to find a consistent socioeconomic bias in self-reported screening attendance, 4 area-level data show lower uptake in more socioeconomically deprived health authorities. 5
The discovery that nearly all cases of cervical cancer are caused by high-risk types of human papillomavirus (HPV), a highly prevalent, sexually transmitted infection, 6 has offered new opportunities for cervical cancer prevention. HPV-DNA testing is used alongside cytology in the USA to increase sensitivity, and ongoing research is assessing the benefit of HPV testing as part of primary screening in the UK and Europe. 7 The use of HPV testing as a triage for borderline changes and mild dyskaryosis is currently being rolled out across the UK. 8 Qualitative research suggests that many women will welcome the introduction of HPV testing, although they are likely to have some concerns. 9 No large-scale quantitative studies of HPV testing acceptability have been carried out in the UK.
The most dramatic development in prevention of cervical cancer is prophylactic vaccination against the common high-risk types of HPV (16 and 18) that are responsible for 70% of cervical cancers. Phase III trials have demonstrated high efficacy in young women (15–26 years) who were not infected with vaccine-related virus types at baseline. 10,11 In the USA, the Centers for Disease Control and Prevention have recommended vaccination for women up to 26 years, and in the UK, the Department of Health has announced that they will be offering vaccination to girls aged 12–13 years with a ‘catch-up’ programme for girls up to 18 years. 12
A number of studies have assessed intended acceptance of HPV vaccination in the USA 13 and the UK, 14,15 but most of these have been in specific population subgroups. In the two UK studies, anticipated acceptance levels were 75–80% among mothers considering the vaccine for their daughters. 14,15
Knowledge about HPV and cervical cancer will be critical to ensure informed participation in testing and vaccination and therefore developing public information about HPV will be an important target for health education. Understanding the demographic characteristics associated with acceptance of HPV testing and vaccination could help identify groups that need to be targeted.
This study used data collected in a population-based survey of British women aged 25–64 years, as part of an ‘omnibus survey’. We first asked about cervical screening uptake. Women were then given information about HPV and asked about their likelihood of accepting an HPV test. A subset of respondents with a daughter aged up to 16 years also reported their willingness to have their daughter immunized against HPV. Sociodemographic factors, screening history, and usual sources of health information, were considered as potential predictors of acceptance of testing and vaccination.
METHODS
Participants
Data were collected by including questions in the NatCen (National Centre for Social Research) omnibus survey between November 2006 and February 2007. Addresses in England, Scotland and Wales (n = 6100, of which n = 5585 were eligible) were selected using stratified random probability sampling of the Postcode Address File. Face-to-face interviews were carried out at 2981 addresses. The questions on HPV were asked only of female respondents. NatCen abide by the Social Research Association Ethical guidelines.
Materials and measures
At the beginning of the interview, women were asked about attendance at cervical screening. They were asked to indicate which statement was closest to their situation: ‘I regularly have cervical cancer screening and do not need reminding’, ‘I regularly have cervical cancer screening but do need reminding’, ‘I do not have regular cervical cancer screening in spite of reminders to do so’ and ‘I have never had a cervical cancer screening test’. Women who responded with the first two options were coded as regular attenders.
Respondents were then given brief information about HPV and cervical cancer and the potential availability of testing and vaccination (the vaccine was mentioned as an option for the future, because no announcement on vaccination had been made in the UK). They were asked how likely they would be to accept an HPV test if they were offered one at their next cervical screening appointment, with responses on a five-point scale (very unlikely, unlikely, not sure, likely, very likely). Women with a daughter aged up to 16 years old were also asked how willing they would be to accept HPV vaccination for their daughter, with responses on a 10-point scale from ‘not at all willing’ to ‘extremely willing’.
Sociodemographic factors including age, marital status, ethnicity, education level and income were assessed by asking respondents to place themselves in one of several predefined categories. These were combined to create appropriate group sizes for analysis. The proportion of ethnic minorities in this sample was 6%, which is slightly lower than the UK population rate (8%). This meant that numbers were too small to examine differences between ethnic minority groups, so respondents were categorized as white (British, Irish or other backgrounds) and non-white (mostly Asian/Asian British or Black/Black British backgrounds).
To assess women's sources of information on female health issues, they were asked to select as many responses as appropriate from a list (doctor/general practitioner, gynaecologist, other specialist, nurse or pharmacist, leaflets in doctor's clinics, friends and relatives, media sources including newspapers, magazines, television or radio, the internet).
Analysis
Data were analysed using SPSS 14.0 (SPSS Inc., Chicago, IL) and were weighted to account for number of adults in the household and non-responder demographics. Because responses to testing and vaccination were highly skewed towards acceptance, outcomes were recoded into binary variables. Respondents were allocated to one of two groups for HPV testing and vaccination. Respondents who reported being likely or very likely to accept an HPV test were coded as ‘acceptors’, all other respondents were coded as ‘hesitant’. The overall distribution for the 10-point scale of willingness to accept HPV vaccine for a daughter is shown in Figure 1. Women who rated their willingness as seven or above were considered to be ‘acceptors’ and all other respondents were coded as ‘hesitant’. Univariate logistic regression analyses were used to identify sociodemographic predictors of screening attendance and intended acceptance of HPV testing and vaccination. Significant variables were also entered into a multivariate logistic regression model. Analyses were repeated with only those who responded ‘very likely’ as acceptors of HPV testing and using 8, 9 and 10 as cut-off points for mothers accepting HPV vaccine for a daughter. These additional analyses produced the same pattern of results with only very small differences in the odds ratios (OR), indicating that the results were not a function of the way that we categorized acceptance.
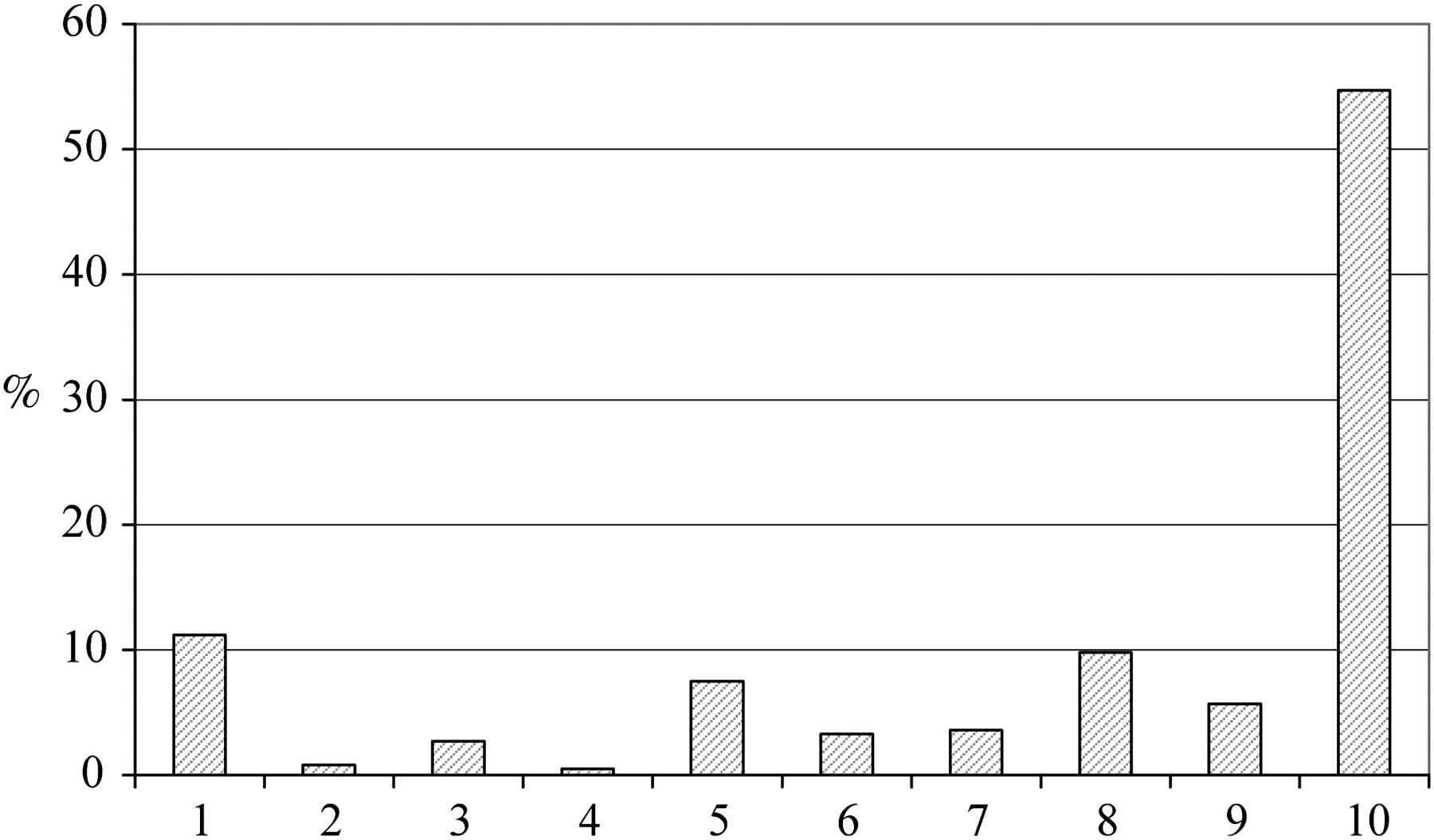
This distribution of responses for willingness to vaccinate daughter
RESULTS
Face-to-face interviews were carried out at 2981 addresses (response rate = 53.4%). For the purpose of this study only data from women aged 25–64 were included (n = 994). The characteristics of the sample are shown in Table 1.
Sample characteristics
Note: Because the data were weighed frequencies were not whole numbers, they have therefore been rounded up to the nearest whole number.
Cervical screening
The majority of women in the screening age range reported regular attendance at cervical screening (89%, n = 866). There were no differences in screening attendance on the basis of age, ethnicity or reported income, but women who were married or cohabiting were more likely to attend for screening than those who were single (OR = 2.04, confidence interval [95% CI]: 1.37–3.02). There were also some differences by education level; with women who had at least minimum educational qualifications (GSCEs) being more likely to attend screening than those with no qualifications (OR = 1.81, 95% CI: 1.18–2.79). Women who reported reading leaflets to find out about female health issues were more likely to attend cervical screening regularly than those who did not read leaflets (OR = 2.08, 95% CI: 1.38–3.15). When marital status, education level and reading leaflets were entered into a multivariate model, all three remained significant predictors of self-reported screening attendance (Table 2).
Predictors of screening attendance and intention to accept an human papillomavirus (HPV) test (25–64 year olds)
OR, odds ratio; CI, confidence interval
HPV testing
After reading a page of information about HPV, women were asked about their willingness to accept an HPV test. Respondents who said they were likely or very likely to accept the test are described as ‘acceptors’ and the remaining respondents are described as ‘hesitant.’ Overall, 70% were accepting of HPV testing and 30% were hesitant about the test. In univariate logistic regression analyses, screening attendance, ethnicity and education were significant predictors of accepting an HPV test. Women who reported regular attendance for cervical screening were more likely to accept an HPV test (OR = 2.01, 95% CI: 1.33–3.05). Women from a white background (OR = 2.66, 95% CI: 1.53–4.64) and those with at least some educational qualifications (OR = 1.63, 95% CI: 1.17–2.27) were also more likely to be ‘acceptors’. Women who reported using some common sources of health information to find out about female health issues, including leaflets (OR = 1.54, 95% CI: 1.15–2.06), friends (OR = 1.48, 95% CI: 1.09–2.01) and the media (OR = 1.47, 95% CI: 1.09–1.97), were also more likely to be ‘acceptors,’ but getting information from health professionals made no difference to anticipated acceptance. When these six variables were entered into a multivariate model, screening attendance, ethnicity and talking to friends about female health issues remained significant predictors of HPV test acceptance (Table 2).
HPV vaccination for daughters
Women who had a daughter up to 16 years (n = 296, 30% see Table 1 for subsample characteristics) were included in an additional analysis to assess maternal acceptance of HPV vaccination for their daughter (Table 3). They were asked to rate on a 10-point scale how willing they would be to vaccinate their daughter against HPV. The mean rating was 7.9 (standard deviation = 3.1), the distribution of responses is shown in Figure 1. Given that the distribution was extremely skewed we defined women who responded seven or above as ‘acceptors’ of the vaccination (74%) and the others as ‘hesitant’ (26%). Anticipated acceptance of HPV vaccination for a daughter was not associated with screening attendance, marital status, ethnicity, education or income. The only variable associated with acceptance was the age of the woman's youngest daughter. Mothers whose youngest daughter was 13–16 years were more likely to be ‘acceptors’ of HPV vaccination than those with younger daughters (OR = 2.91, 95% CI: 1.27–6.65).
Predictors of human papillomavirus vaccine acceptance for a daughter (mothers of upto16 year olds)
OR, odds ratio; CI, confidence interval
DISCUSSION
Over the past 20 years, cervical screening in the UK has been highly successful, preventing thousands of cancers each year. HPV testing and vaccination offer new opportunities for cervical cancer prevention. As these are introduced into the cancer prevention services in the UK, it will become increasingly important to identify predictors of acceptance of these new technologies. This study used a survey methodology to identify population groups who were most likely to report screening attendance and intention to participate in HPV testing or vaccination.
Self-reported screening uptake in this study was higher than the UK figure for 2006 (89% compared with 79%). 16 This could be due to social desirability bias in response to the screening question or because women who respond to surveys may simply be more likely to ‘take part’ more generally, and therefore could be over-represented in the sample. Marit al status and education were significant predictors of screening attendance – with more educated women and married women being more likely to attend. This is consistent with findings from a previous ONS survey (collected in 1999), which also found marital status and education level to be the two sociodemographic predictors of self-reported screening attendance in a multivariate model. 4
Regular attendance at cervical screening was an important predictor of HPV test acceptance in both the univariate and multivariate model. This could be because the question referred to accepting the test while attending for screening and it is possible that HPV self-testing could overcome this barrier. Self-testing has been shown to be highly acceptable among British women 17 and a recent study in Sweden achieved 58% self-test return rate among women who were not attending for conventional cervical screening. 18 There were two interesting differences between screening attendance and intended acceptance of an HPV test. Firstly, while ethnicity was not associated with reported screening attendance, it was a predictor of HPV test acceptance, with higher acceptance among respondents from white backgrounds. This is consistent with qualitative work that has identified specific cultural barriers to HPV testing among women from some ethnic minority groups. 9 The second difference is that marital status, which was associated with reported screening attendance, was not important in relation to HPV testing. Existing research suggests that women who are single are less likely to attend for cervical screening. 4 This is worrying because single women are less likely to be in a monogamous relationship and may therefore be at higher risk of HPV and pre-cancerous changes. However there was no association between marital status and HPV test acceptance. One possible explanation for this is that understanding the sexually transmitted nature of HPV and cervical cancer could make detection methods more acceptable to those in higher risk groups.
In this study we used a 10-point scale to assess acceptability of HPV vaccination. The mean acceptability score was 7.9, which was slightly higher than the mean score of 6.6 found in a USA study using the same scale. 19 The data for the USA study were collected in 2005 and so this small difference is not unexpected. Previous surveys assessing HPV vaccine acceptability in the UK have found that between 75% and 80% of parents are likely to accept the vaccine and our survey findings identified 74% of parents selecting a rating of seven or above in our 10-point scale.
There was a lack of association between sociodemographic factors and acceptance of HPV vaccination among mothers, and although we recognize that our subsample may have been underpowered to detect small differences as significant, the findings are consistent with results from other surveys assessing anticipated HPV vaccine acceptance in the UK. 14,15 If HPV vaccine acceptance spans all sociodemographic groups, then it has the potential to decrease disparities in cervical cancer in the long term. Because screening will need to continue in order to detect cervical cancers caused by high-risk types other than HPV 16 and 18, there are likely to be some persistent differences due to socioeconmic status (SES) differences in screening participation. 4,5 The only significant predictor of HPV vaccine acceptance was age of youngest daughter, with mothers of 13–16 year olds being most likely to accept vaccination for their daughter. Daughter's age has been highlighted as an important factor in previous research, 20,21 and therefore, emphasizing the importance of vaccinating at the recommended age (12–13 years old) will be important to ensure administration of the vaccine is not delayed.
Respondents who reported reading leaflets, using the media, or talking to friends as sources of information for finding out about female health were more likely to be accepting of an HPV test. This may be indicative of an interest in health issues more broadly. However, these factors were not associated with acceptance of vaccination for a daughter, which suggests that any campaign to promote vaccination may need to involve alternative methods of communication.
One major limitation of this survey was that the response rate, though adequate, was not high (53.4%). Given the over-representation of screening attenders in the sample, it is possible that the findings over-estimate the acceptability of HPV testing and vaccination. The absolute levels of acceptability should therefore be interpreted with some caution. However, unlike most previous surveys of HPV vaccine acceptability, our questions formed part of a general survey on a range of issues, so specific attitudes to this topic are unlikely to have biased participation.
To our knowledge this is the first study to use data from a nationally representative British sample to examine the predictors of public interest in HPV testing and vaccination. The results are consistent with findings from studies in the USA 13 and from specific populations in the UK, 14,15 which indicate that acceptance is likely to be good even before any public education campaigns. Sociodemographic factors predicted acceptance of an HPV test, but there appeared to be less association between SES and willingness to vaccinate a daughter against HPV. Vaccinating young girls against HPV may have the potential to reach groups that would be unlikely to attend screening, therefore decreasing disparities in cervical cancer. Future work should continue to explore this possibility in the context of actual vaccine uptake in the years to come.
Footnotes
ACKNOWLEDGEMENTS
The NatCen survey was funded by GlaxoSmithKline Biologicals. Laura Marlow and Jane Wardle and are supported by Cancer Research UK. Jo Waller has an ESRC/MRC fellowship.