
Abstract
Objectives
The aim of the study was to examine ethnic differences in participation in colorectal cancer screening by flexible sigmoidoscopy (FS). It assessed both intentions to be screened and actual screening uptake, and considered whether demographic, health and psychosocial factors mediated the ethnic differences. The setting of this study follows a subset of participants from the UK FS Trial.
Methods
A postal questionnaire assessed ethnicity, demographic characteristics, health, attitudes to screening and FS screening intentions. Data on screening intentions were available for 17,333 adults aged 55–64 years (Sample 1). Screening uptake was recorded in a subsample of 4303 respondents who were subsequently randomized to receive an invitation to screening (Sample 2).
Results
Screening intentions in Sample 1 were equally high across all the ethnic groups (>80% [13,724/17,042] reported they were interested). In contrast, attendance (Sample 2) was considerably lower among Asians (54% [43/79]) compared with White (69% [2843/4123]) or Black (80% [33/41]) respondents. Multivariate analysis showed that potential explanatory factors, including socioeconomic deprivation, poor health and fearful and fatalistic attitudes did not account for the lower screening attendance among Asians.
Conclusion
Further research is required to identify explanations for the gap between intentions and behaviour in UK Asians if any future FS screening programme is to be introduced equitably.
INTRODUCTION
Evidence from the UK Breast and Cervical Cancer Screening Programmes indicates that screening rates among ethnic minority groups – particularly south-Asians – are lower than in the white-British population. 1–3 The roll-out of faecal occult blood testing (FOBT, a test that examines stool samples for traces of blood which may indicate bowel cancer) is currently in progress, but the large-scale pilot study 4 that preceded its introduction also found lower levels of participation among south-Asians. 5 More recently, an evaluation of the second round of the English FOBT Pilot reported poorer uptake of screening in areas with a higher proportion of residents from the Indian subcontinent. 6
Flexible sigmoidoscopy (FS) is a test that involves direct visualization of the distal colon to detect and remove precancerous growths, with the aim of reducing colorectal cancer incidence as well as mortality. It is being evaluated for inclusion in the UK Cancer Screening Programme in the future, and therefore issues of disparities are of considerable interest. Studies from the US indicate that participation in FS screening is lower in ethnic minority groups, 7–9 but these findings cannot be generalized to the UK context because of differences in cultural background and service provision.
The aim of the present analysis was to examine ethnic differences in participation in FS screening in the UK, and explore possible determinants of lower uptake in non-White groups. One potential explanation is socioeconomic position (SEP), which has been strongly linked with lower screening uptake in the general population. 10,11 Ethnic minorities tend to be more socioeconomically deprived, 12 and therefore ethnic differences in screening participation could be due to differences in SEP. Nazroo 13 showed that once adjustments for socioeconomic factors are made, relationships between ethnicity and heart disease are greatly diminished.
Another possible explanation for lower uptake of screening in ethnic minority groups is poorer health. All ethnic minority groups in the UK (with the exception of the Chinese) report worse health than the white majority. 14 Poor subjective health has been associated with lower uptake of screening among the general population, 15 and might therefore explain some ethnic differences.
Cultural differences in attitudes towards screening or cancer could be another explanation. Fatalistic beliefs have been linked with the avoidance of screening, 16,17 and such beliefs have been found to be higher among African Americans than white Americans 18 and high among Bangladeshis living in the UK. 19 Embarrassment, fear and lack of knowledge have also been identified as possible determinants of poor uptake in cervical and breast screening. 20–22 The FOBT Pilot found that south-Asians were less aware of bowel cancer and less confident of the effectiveness of screening than white Europeans, which might explain their lack of enthusiasm for screening. Some non-White groups feel less at risk of developing bowel cancer 23 and are less likely to know someone with the disease. 5 This is not entirely surprising because there are ethnic differences in the risk of developing bowel cancer, 24–26 and people from lower-risk groups would have less direct experience of the disease among their family and friends. However, lower perceived risk is a concern if it is a deterrent to screening participation, particularly when bowel cancer rates in south-Asians have increased in recent years – most likely due to lifestyle changes – while they have fallen in the rest of the population. 27
The present study examined ethnic differences in both intentions to attend for FS screening and actual attendance. It also considered the evidence for demographic, health and psychosocial mediators of ethnic differences. The data are from the UK FS Trial which was a large-scale trial to assess the efficacy of ‘once-only’ FS as a preventive screening procedure in men and women aged 55–64 years. 28
METHODS
Participants and procedures
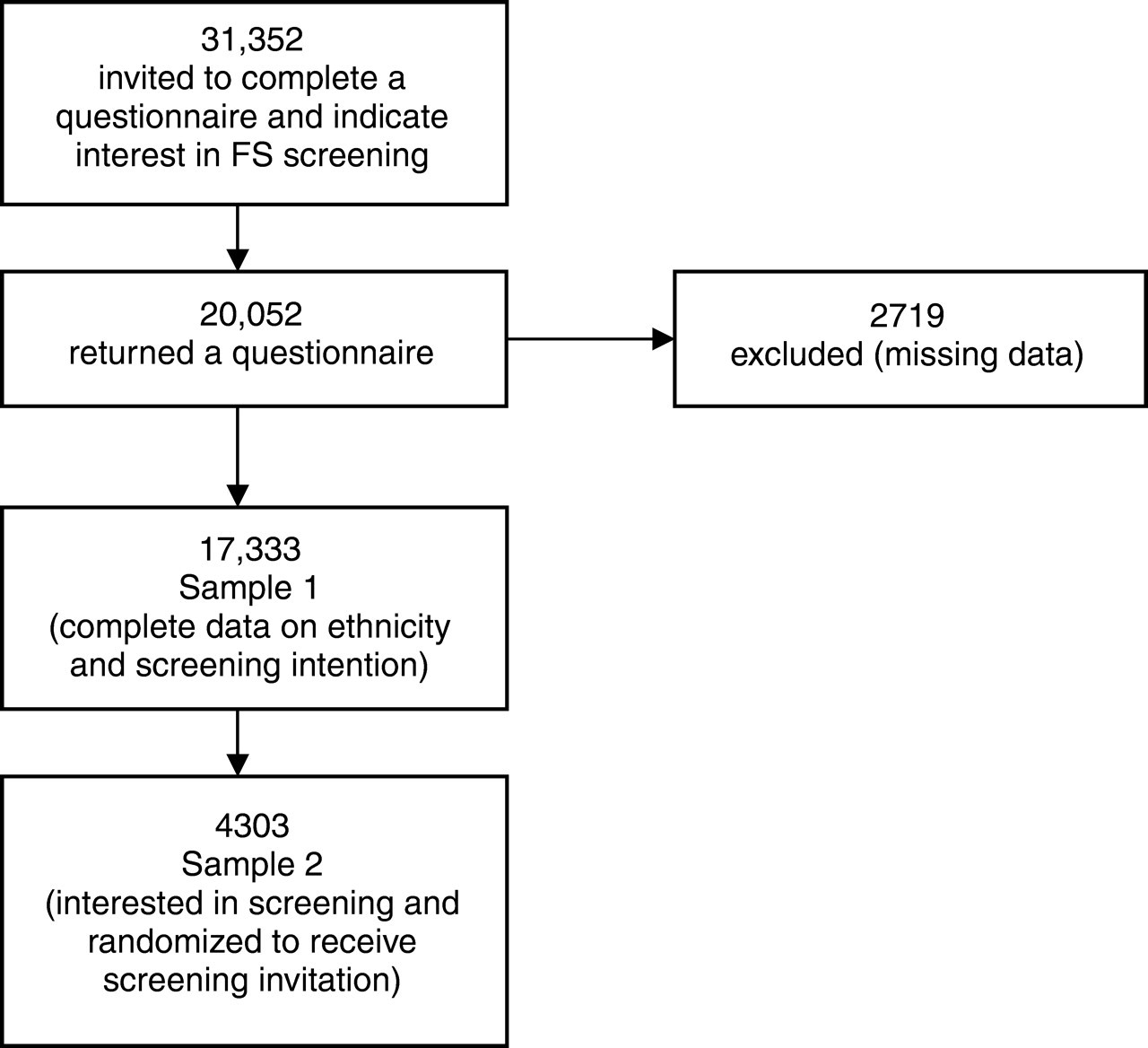
A two-stage recruitment approach was used to maximize statistical power in intention-to-treat-analyses in the UK FS Trial. 29 Potential participants were provided with information about FS screening (Appendix 1), and were first asked to indicate whether they would attend for screening if invited (intention question). Interested participants were then randomized to usual care or screening in a 2:1 ratio, and those in the screening arm were invited for a test. Attendance was recorded at the screening centre. The data for these analyses come from six of the UK FS Trial centres (Glasgow, Leeds, Harrow, Birmingham, Welwyn Garden City and Leicester). Adults aged 55–64 years registered with a participating General Practice (n = 31,352) were mailed a background questionnaire including items on ethnicity, health, attitudes and FS screening intentions. A reminder was sent if there was no response after two weeks. In total 20,052 (64%) responded, but 2719 were excluded because they had missing data on the items used in these analyses (Figure 1). This gave a sample of 17,333 (55% of the total sample and 86% of responders) for examining screening intentions. Sample 2 comprised the subgroup of people who had indicated they were interested in screening and were subsequently randomized to be invited to screening (n = 4303), representing 14% of the total sample and 21% of responders (Figure 1). Those randomized to screening were sent an appointment time approximately five weeks in advance.
Recruitment of samples 1 and 2
Measures
The mailed questionnaire was accompanied by a letter from the general practitioner (GP) which included brief information about the ‘Flexi-Scope’ test in five languages (Gujarati, Urdu, Hindi, Punjabi, Bengali) that represent most of the ethnic minority language groups in the UK. They were invited to contact the screening centre if more information in any of the languages was required. The questionnaire was extensively piloted and revised in terms of presentation, readability, comprehensibility, face validity and the time taken to complete.
Screening participation was assessed in two ways: (i) intentions to have the FS test (Sample 1) and (ii) attendance at screening (Sample 2). The screening intention question asked, ‘If you were invited to have a bowel cancer screening test, would you take up the offer?’ with the response options ‘yes definitely’, ‘yes probably’, ‘probably not’, ‘definitely not’. For going forward to the second stage, a positive intention was defined as responding either ‘yes definitely’ or ‘yes probably’. Attendance in the subsample randomized to receive a screening invitation (Sample 2) was based on clinic records. FS screening is not part of the UK National Screening Programme and Trial participants would not otherwise have access to the test, nor was any other bowel cancer screening programme offered at the time.
Demographic factors
Ethnicity was measured in the self-report questionnaire by the item, ‘Which of these best describes your ethnic background?’ with response options, ‘White’, ‘Black’, ‘Asian’, ‘Other’, ‘Do not wish to answer’. In the UK 2001 Census, 45% of the Asian population described themselves as Indian, 32% as Pakistani, 12% as Bangladeshi and 11% as ‘Other Asian’. Among the Black population, 49% described themselves as Caribbean, 42% as African, and 8% as ‘Other Black’. In Sample 1, 218 people responded ‘do not wish to answer’ to the ethnicity question and 73 responded ‘other’, and in Sample 2, 14 people had said ‘do not wish to answer’ and 4 responded ‘other’. These cases were excluded from the analysis because the focus was on differences between ethnic groups. Age and gender were known from the GP records. The marital status item was, ‘What is your marital status?’ and for the present analyses, responses were dichotomized to married/living as married versus not married. Items on education (‘Do you have any educational qualifications?’; responses ‘yes’ or ‘no’), housing tenure (‘Do you own or rent your home?’; response options ‘own it/buying it’ and ‘rent it’) and car ownership (‘Does your household have a car?’; response options ‘no’, ‘yes, 1', and ‘more than 1’) were combined to produce a socioeconomic deprivation score ranging from 0 (affluent: educational qualifications, home owner, more than 1 car) to 3 (deprived: no qualifications, renting home, no car). This socioeconomic deprivation score was developed for the analysis of the UK FS Trial data. 10
Health
Perceived health status was assessed with the question ‘Would you say that for someone of your age your own health in general is: excellent; good; fair; poor’. 30 For the analyses responses were recoded as excellent and good versus fair and poor. Bowel symptoms over the past three months were assessed with a list of seven symptoms (constipation, haemorrhoids, diarrhoea, wind, pains in abdomen, incontinence and blood in stools) and each was rated for frequency ‘no’, ‘occasionally’, ‘frequently'. For the analyses bowel symptoms were recoded as no bowel symptoms versus at least one bowel symptom.
Attitudes towards the test
Attitudes were measured with a list of possible beliefs about the test that had been developed following extensive piloting. There were two positive items (‘The test would give me peace of mind’, ‘The test would reassure me that everything was ok’) and four negative items (‘Having the test would be embarrassing’, ‘The test would be uncomfortable’, ‘Having the test would be tempting fate’, ‘The test may make me worry about cancer’). Response options were on five-point scales from ‘strongly disagree’ to ‘strongly agree’, with higher scores representing more positive or negative attitudes.
Bowel cancer risk and worry
Perceived risk was assessed with the item, ‘Compared with other men and women of your age, do you think you chances of getting bowel cancer are: ‘lower’, ‘about the same’, ‘higher’. 31 The bowel cancer worry item asked, ‘How worried are you about getting bowel cancer?’ with response options ‘not worried at all’, ‘a bit worried’, ‘quite worried’, ‘very worried’. 32
Family history
Family history of bowel cancer was assessed with the question, ‘Have any members of your family (BLOOD relatives, not relatives by marriage) had bowel cancer?’ Options were mother, father, son(s), daughter(s), sister(s) and brother(s), and participants were required to respond ‘yes; no; do not know’ for each relative. These responses were coded into the categories of none or one or more.
Statistical analyses
All analyses were carried out using SPSS 14.0. χ 2 Tests and one-way analysis of variance were used to examine the relationships between ethnicity and demographic factors, attitudes, perceived risk, bowel cancer worry, health and family history. Tukey tests were used to make post hoc comparisons. Multivariate logistic regression was used to examine the relationship between ethnicity and intentions, controlling for demographic factors and health. Multivariate logistic regressions were used to examine the relationship between ethnicity and attendance, controlling for the predictor variables.
RESULTS
Intentions to have flexible sigmoidoscopy screening (Sample 1)
Sample 1 was 96.8% White, 0.8% Black and 2% Asian. Data obtained from the 2001 Census for England show that for men and women aged 55–64 years, the proportions were: 95.2% White, 1.5% Black and 2.6% Asian; thus, the current sample under-represented the ethnic groups within England.
The demographic characteristics of Sample 1 are described in Table 1. In the White and Black groups there were more female than male participants, while among the Asians, only 44% were female. There were no age differences across ethnic groups. Black respondents were the least likely to be married or living as married (55%) and Asians were the most likely to be married (83%). Asians had the fewest respondents in the most deprived group. There were significant ethnic differences in perceived health status, with 67% of the White group reporting their health to be ‘excellent’ or ‘good’, compared with only 58% of Black and 50% of Asian respondents.
Characteristics of Sample 1 by ethnic group
Intentions to participate in FS screening were uniformly high across all ethnic groups, with over 80% of participants reporting being definitely or probably interested (Table 2). χ 2 Test revealed that interest in FS screening was not significantly different between ethnic groups, although Black respondents showed the strongest intentions with 60% saying they would be ‘definitely’ interested, compared with 53% of Asian and 50% of White respondents.
Intentions to have flexible sigmoidoscopy screening by ethnic group
Table 3 presents univariate and multivariate logistic regressions examining the association between ethnicity and intentions. The univariate odds ratios reflect the χ 2 test results in Table 2 and show no differences in intentions across ethnic groups. A multivariate analysis was used to determine whether the relationship between ethnicity and screening intention was modified by adjustment for demographic factors (gender, age, marital status, deprivation) and perceived health. The relationship did not change in the multivariate analysis; all three ethnic groups had similar intentions to be screened.
Logistic regression models predicting intentions to be screened in Sample 1
*Multivariate odds ratios adjusted for gender, age, marital status, deprivation and perceived health
Attendance at FS screening (Sample 2)
Sample 2 was 97% White, 1% Black and 2% Asian, which again under-represented ethnic minorities in 55–64-year-olds in England.
Participants who described themselves as Black had attendance rates of 80%, while the White group had 69% attendance. Asian participants were significantly less likely to attend than the other groups, with only 54% having the test (χ 2 [3, 4243] = 10.2, P = 0.006).
There were no significant differences in gender, age or socioeconomic deprivation across ethnic groups (Table 4) and therefore socioeconomic factors were unlikely to explain the ethnic differences in participation. Asian participants were more likely to be married (87%) compared with 75% of White and 58% of Black participants. However, marital status has already been shown to be positively associated with screening attendance 33 and therefore this did not explain the lower uptake among Asians.
Characteristics of Sample 2 by ethnic group
*Fewer than 5 counts per cell
Possible psychosocial explanations for the difference in attendance across ethnic groups
Table 5 illustrates the relationships between ethnicity and potential predictors including attitudes towards the test, perceived risk and worry, health and family history. In terms of practical concerns such as embarrassment or belief that the test would be uncomfortable, there were no differences across ethnic groups. Similarly, positive attitudes that the test would give ‘peace of mind’ and would be reassuring were equally endorsed by all ethnic groups. However, there were significant differences in beliefs that having the test would be ‘tempting fate’ or would cause worry about cancer. In order to determine which means were significantly different, post hoc Tukey tests were used to compare all possible pairs of means. Tukey tests revealed that for ‘tempting fate’, Black and Asian groups were both significantly more fatalistic than the White group (both P < 0.001). For the belief that the test would cause worry, post hoc Tukey tests showed that Asians anticipated more worry than the White group (P = 0.042). Perceived risk did not vary across ethnic groups. There was also a significant difference in worry about bowel cancer across the ethnic groups, and post hoc tests showed that Asians had significantly higher worry than the White group (P = 0.004).
Possible explanatory factors for differences in attendance across ethnic groups (Sample 2)
*Response options were on five-point scales: 1 = ‘strongly disagree’ to 5 = ‘strongly agree’. Higher scores represent more positive or negative attitudes
† χ 2 tests report differences across ethnic groups for those rating their health as fair or poor versus excellent or good, reporting no bowel symptoms versus at least one bowel symptom, and having at least one blood relative versus having no blood relatives
‡Fewer than five counts per cell
As with Sample 1, the White group were the most likely to report having ‘excellent’ or ‘good’ health (Table 5), but there were no ethnic differences in bowel symptoms. It was not possible to determine if there were significant differences in family history of bowel cancer because there were too few counts per cell among the non-White groups, but the White group reported the highest proportion of relatives affected by bowel cancer.
The first column of Table 6 shows the univariate odds ratios for the association between health and psychosocial variables and attendance. These results confirm the χ 2 test result, showing that people from Asian backgrounds were significantly less likely to attend FS screening than the White group. Participants reporting ‘fair’ or ‘poor’ health were significantly less likely to attend screening than those reporting ‘excellent’ or ‘good’ health. Bowel cancer worry was not related to attendance. Belief that having the test would ‘tempt fate’ or cause worry were associated with lower attendance.
Logistic regression analysis of the relationship between ethnicity and attendance at screening (Sample 2)
*Controlling for gender, age, marital status and deprivation
†Statistically significant at P ≤ 0.005
‡Odds for 1 point increase in score
Table 6 describes a multivariate logistic regression which was used to assess the relationship between ethnicity and attendance while controlling for potential demographic (gender, age, marital status, deprivation) and psychosocial (perceived health, cancer worry, attitudes) explanatory factors. However, controlling for these factors did not diminish the observed ethnic differences in screening attendance and Asians continued to show significantly lower odds of attending screening compared with the White group.
DISCUSSION
The study is the first to present data on the relationship between ethnicity and participation in FS bowel screening in the UK. Encouragingly it showed that intentions to attend for FS screening were high across all ethnicities (>80%). This finding supports previous work reporting high levels of interest in FS screening and similar levels of intentions across the main UK ethnic groups. 34
In contrast, the data on uptake showed that these positive intentions were differentially translated into behaviour. Both Black and White respondents had significantly higher attendance rates than Asians (80% versus 69% versus 54%). Similar results for south-Asians had been reported in the FOBT Pilot, with initial interest levels equivalent to the White sample, but subsequent return of kits and attendance at follow-up colonoscopy being significantly lower. 5
The FOBT Pilot did not have data on other ethnic groups, but other studies have reported high rates of screening attendance for cervical and breast cancer among African-Caribbean women, 32,35 which would concur with our findings in FS screening. Given that this test was for both sexes and there were no sex differences in participation, these results suggest that African-Caribbean men have similar levels of enthusiasm for cancer screening to African-Caribbean women. This is a very positive finding indicating engagement with cancer prevention in the African-Caribbean community.
The finding of lower FS screening uptake among Asians remained significant after controlling for socioeconomic status, unlike results for ethnicity and coronary heart disease, 13 where the relationship became non-significant once socioeconomic factors were controlled. This suggests that Asians' lower attendance is independent of their level of deprivation, although we cannot rule out the possibility that other indices of socioeconomic status may explain the relationship between ethnicity and screening.
Attitudinal factors varied by ethnic group, with Asian respondents reporting more fatalism and worry about the test, and more worry about cancer. In the UK FS Trial, fear and fatalism were both associated with intention to attend screening 10 and the FOBT Pilot reported similar findings. 5 However, these factors did not appear to be the cause of the ethnic differences in uptake in this sample. The problem appears to be more related to the ‘gap’ between intentions – which were high and the same across all groups – and action. Inconsistencies between intentions and actions are well recognized in the psychological literature. 36 We did not assess self-efficacy or perceived behavioural control which have been found to be important in translating intentions into action, 37,38 and these may vary by ethnic background. Other potential explanations include forgetting or ambivalence due to conflicting intentions or goals such as wanting to be screened but not wishing to take time off work. Given that UK Asians are more likely to be self-employed, particularly Pakistanis, among whom 22% report being self-employed compared with 10% of white-British and < 10% of Black people, 39 the competing goals of screening and work warrant further investigation.
There are of course limitations to the study. Ethnicity was defined using broad categories and there is likely to be variability within groups in terms of SEP, cultural beliefs and religion, which may limit the validity of using groupings such as Asian or Black. It would have been helpful to have assessed religion in the present study because it can provide a stronger cultural identity than ethnicity. A further limitation was that although the proportions of ethnic groups approximated the general population, there were more white-British and fewer Blacks and Asians, so the findings cannot be fully generalized to all the ethnic groups. Furthermore, having a sample that approximates the general population gives small samples of ethnic minority groups. It is possible that with larger samples some of the results may have reached statistical significance and future studies should consider over-sampling ethnic minority groups to increase the sample size and the reliability of the results. Previous work has found that ethnic minority groups tend to be more deprived, 12 but among the FS Trial participants, Asians were either no different from Whites or had higher SEP. Of course, our data are restricted to people who were willing to complete the questionnaire and so we do not know about the non-represented groups' views of FS screening. Nevertheless, it is notable that even in this self-selected and highly motivated group, ethnic differences in screening participation emerged, and it indicates the need to look beyond socioeconomic deprivation for an explanation.
CONCLUSIONS
Intentions to attend for FS screening were equally high in White, Black and Asian ethnic groups, but actual attendance was lower among Asian respondents than either of the others. This finding highlights the difficulty of exploring barriers to cancer screening by using surveys or focus groups that focus only on intentions. Multivariate analysis showed that potential explanatory factors, including socioeconomic deprivation, poor health and fearful or fatalistic attitudes did not account for the lower screening attendance among Asians. Further research is required to identify explanations for the gap between screening intentions and screening behaviour in Asians.
Footnotes
ACKNOWLEDGEMENTS
Support from the Department of Health and Cancer Research UK is gratefully acknowledged. The MRC funded the UK Flexible Sigmoidoscopy Trial.