
Abstract
Objectives
Evaluation and comparison of the performance of organized and opportunistic screening mammography.
Methods
Women attending screening mammography in Denmark in 2000. The study included 37,072 women attending organized screening. Among these, 320 women were diagnosed with breast cancer during follow-up. Opportunistic screening was attended by 2855 women with 26 women being diagnosed with breast cancer. Data on women attending screening were linked with information on cancer status. Each woman was followed with respect to diagnosis of breast cancer (invasive as well as in situ) for a period of two years. Screening outcome and cancer status during follow-up were combined to assess whether the result of the examination was true-positive, true-negative, false-positive or false-negative. Based on this classification, age-adjusted sensitivity and specificity of organized and opportunistic screening were calculated.
Results
Defining BI-RADS™ 4-5 as a positive screening outcome, the overall sensitivity of opportunistic screening was 33.6% and the specificity was 99.1%. Using BI-RADS™ 3-5 as positive, the sensitivity was 37.4% and the specificity was 97.9%. Organized screening (which was not categorized according to BI-RADS™) had an overall sensitivity of 67.2% and a specificity of 98.4%.
Conclusion
Our study showed a considerably higher sensitivity in organized screening than in opportunistic screening, while the specificity was fairly similar in the two settings. The findings support implementation of population-based breast screening programmes, as recommended in the ‘European guidelines for quality assurance in breast cancer screening and diagnosis’.
Introduction
It is recommended in the ‘European guidelines for quality assurance in breast cancer screening and diagnosis’ that population-based breast screening programmes with mammography are implemented throughout the Europe. It is furthermore recommended that a screening radiologist should undertake to read a minimum of 5000 screening cases per year. 1 Several European countries nevertheless still have opportunistic breast screening with many mammograms being taken and read in small clinics. A mixed model with small clinics and low volume reading radiologists being integrated into organized screening programmes exists in France, 2 Luxembourg 3 and Switzerland. 4 In Austria,5,6 the benefit of organized versus opportunistic mammography screening is still being debated despite the now well disseminated European guidelines for population-based mammography screening programmes.
The quality of organized mammography screening has been evaluated in several countries 7 with Sweden8–10 and the Netherlands 11 as prime examples. Due to its decentralized nature and lack of systematic reporting, the quality of opportunistic mammography screening is more difficult to evaluate. We have taken advantage of the linkage possibilities between the Danish health care registers and compared the quality of organized mammography screening with that of opportunistic screening. Our quality indicators are the sensitivity and the specificity of the screening mammograms within two years of the screening date.
Material and methods
In 2000, two out of 15 Danish administrative regions had organized mammography screening programmes. A total of 100,000 women aged 50-69 residing in these regions were invited to biennial screening. Diagnostic mammography is available to all Danish women free of charge after referral from a general practitioner. Some of these examinations may be in asymptomatic women, although opportunistic screening is not widely used in Denmark. 12 Indication for diagnostic mammography is normally not registered in Denmark, and in most clinics it is therefore not possible to distinguish between examinations of symptomatic women and examinations of asymptomatic women. In two clinical settings it has, however, been possible to separate out the mammograms taken in asymptomatic women. This study is therefore limited to a comparison between the performances of mammograms from the organized screening programmes and mammograms taken in asymptomatic women in the two diagnostic settings, i.e. opportunistic screening examinations. The two datasets are in the following called organized and opportunistic screening, respectively.
A personal identification number is provided to all Danish citizens along with registration in the Central Population Register (CPR). The CPR contains personal information including dates of death and emigration. The two organized screening programmes registered data on all women attending screening in 2000 with personal identification number, and date and result of the examination. Invitation to mammography is administered slightly different in the two regions offering screening, and there was consequently a small difference between the regions in age of attending women. In both regions though, some women may turn 70 before they are actually examined. Women older than 70 years were excluded from the analysis, as were women previously diagnosed with breast cancer, women without a breast cancer diagnosis who died or emigrated during the two-year follow-up period, and a few women attending opportunistic screening before organized screening. In all, a total of 38,967 screening examinations were performed in the organized programmes in 2000. All examinations were read twice by two different radiologists, and data on 37,072 women were included in the analysis. For the analysis, a woman was defined as having a positive screening outcome if further assessment was advised, if not, the outcome was defined as negative.
Data on opportunistic breast screening in Denmark in 2000 were collected from the two clinics, where it was possible to separate out the mammograms taken in asymptomatic women. Like in the organized setting, data included personal identification number along with examination date and result. A total of 4970 examinations were performed in 4947 patients. Ultra sound examinations, men, women earlier diagnosed with breast cancer, women without a breast cancer diagnosis who died or emigrated during the two-year follow-up period, women having participated in the organized screening programmes in 2000 prior to the examination, and multiple examinations in 2000, all except the first were excluded. The final dataset included 2855 women aged 50-70 having had examination of both breasts. The majority of excluded women (n = 1938) were excluded due to their age. The outcomes of opportunistic mammograms were originally reported by the radiologist in free-text. These reports were collected and coded according to the American five-point BI-RADS™ classification system. 13 Each breast was scored separately, but only the highest score for each woman was used for the analysis. A score of 1-3 was defined as a negative outcome, whereas a score of 4 or 5 was defined as positive.
The cohort of all screened women was followed for two years after the date of examination to assess the subsequent breast cancer status. A two-year period is the commonly used follow-up period to determination of interval cancers in mammography screening as it corresponds to the time between examinations in the organized programmes. 14 If a woman was rescreened before the end of the two-year period, follow-up ended at the new examination date. Information on breast cancer status was obtained using the personal identification number and linking the cohort with data from the Danish Breast Cancer Group (DBCG), the Danish Cancer Register (DCR), and the Danish Registry of Pathology (DRP). DBCG includes information on all invasive and in situ breast cancers, 15 DCR includes information on all invasive cancers 16 and DRP includes information on all pathology specimens. 17 Multiple registers were used since DBCG was not fully updated for 2002 at the time of analysis. Incident breast cancer was defined as all invasive or in situ breast cancer observed in the follow-up period.
The performance of mammography screening was measured by calculating sensitivity and specificity. Sensitivity was defined as true-positive/(true-positive + false-negative) and specificity as true-negative/(true-negative + false-positive), where true-positive denotes women with a positive screening outcome and a breast cancer diagnosis during follow-up, true-negative denotes a negative outcome with no breast cancer, false-positive denotes a positive outcome with no breast cancer and false-negative denotes a negative screening outcome and diagnosed breast cancer. Both sensitivity and specificity were adjusted for age at screening (above or below 60 years) using a regression model. 18
Results
Among the 37,072 analysed women attending organized screening, 729 mammographics were positive and 36,343 were negative (Table 1). During the two-year follow-up, 320 breast cancers were diagnosed. In all, 36,245 screenings were true-negative, 222 were true-positive, 98 were false-negative, and 507 were false-positive (Table 2). In the opportunistic setting, 21 of the 2855 mammographics had a positive outcome and 2834 mammographics were negative. In 26 cases, the woman was diagnosed with breast cancer during follow-up; 2817 screenings were true-negative, 9 were true-positive, 17 were false-negative and 12 were false-positive.
Number of women * screened with mammography in denmark in 2000
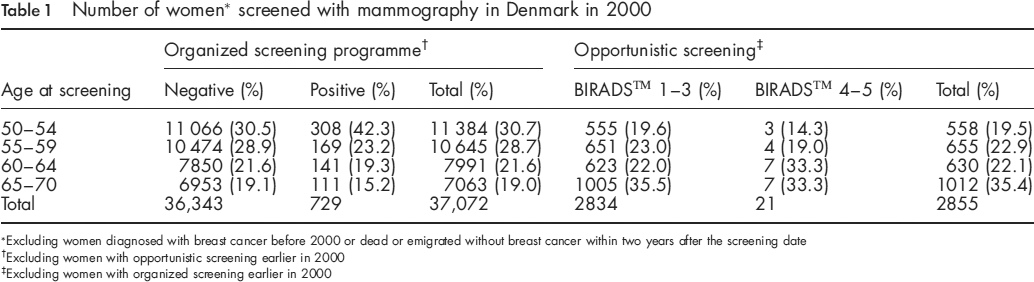
Excluding women diagnosed with breast cancer before 2000 or dead or emigrated without breast cancer within two years after the screening date
Excluding women with opportunistic screening earlier in 2000
Excluding women with organized screening earlier in 2000
Women screened with mammography in Denmark in 2000 by breast cancer status two years later

Sensitivity and specificity of organized and opportunistic screening

Alternatively, a BI-RADS™ score of 3-5 was defined to be positive and the sensitivity of opportunistic screening was then 37.4% with CI (22.6, 61.7). The specificity was 97.9% with CI (97.4, 98.4).
Discussion
Our study compared the performance of organized and opportunistic mammography screening in Denmark in 2000. The organized programme had a considerably higher sensitivity than the opportunistic screening. The specificity of the organized programme was higher, 0.5, than that of the opportunistic screening when BI-RADS™ codes 3-5 were considered positive and lower, 0.7, when only BI-RADS™ codes 4-5 were considered positive.
Our study is based on a comprehensive registration of all mammograms undertaken in the two settings in 2000. Information on the diagnostic outcome two years later was collected via linkage with nationwide health registers. Our study is therefore unlikely to be affected by selection and/or reporting biases. Each of the organized screening centres included in this study has double-reading of mammograms for a minimum of 20,000 screened women per year divided between two to four radiologists. In comparison, a total of 51,337 women had diagnostic mammography in Denmark in 2000 divided between 47 clinics. 19
Although the ‘European guidelines for quality assurance in breast cancer screening and diagnosis’ recommends implementation of population-based breast screening programmes and a minimum reading volume for radiologists of 5000 screening cases per year, Frede 5 argued in favour of opportunistic screening based on Austrian data. He reported 79.6% of cases found by opportunistic screening to be ductal carcinoma in situ (DCIS) or lymph node negative, and claimed a participation rate of 75% of the target population (women aged 35 and older). This estimate was, however, very speculative and based on the numbers provided in the paper it seemed to be closer to 50%. The European guidelines recommend a participation rate of 75%. In comparison, the first three invitation rounds of one of the Danish organized screening programmes had an average participation rate of around 83%, and found 74.6% of cases to be DCIS or lymph node negative. 20
In conclusion, the specificity was fairly similar in the organized screening and in the opportunistic screening. Both were at an acceptable level, the relative size varied with the cut-off point used for positive finding. The sensitivity was, however, much better in the organized screening, thus in total resulting in a superiority of the organized programmes. In order to ensure the quality of breast cancer screening, our findings therefore support implementation of population-based breast screening programmes, as recommended in the European guidelines.
Footnotes
Acknowledgement
This work was financially supported by the Danish Cancer Society.