
Abstract
Leiomyoma of the nipple is a rare, benign, non-epithelial tumor that is thought to arise from smooth muscle fibers in the subareolar tissue of the breast. We report an unusual case of leiomyoma of the nipple in a 32-year-old woman in whom the diagnosis was made by ultrasound-guided core needle biopsy. She came to our hospital complaining of a recently enlarged nipple with discharge and erosion in the region of the left nipple-areolar complex. This mass was evaluated by mammography, ultrasonography, and magnetic resonance imaging (MRI). To the best of our knowledge, this is the first case of a leiomyoma of the nipple examined by MRI. MRI showed an oval mass with circumscribed margins that appeared as an intermediate signal intensity on both T1- and T2-weighted images. A dynamic MRI study showed a rim-enhancing oval mass with delayed persistent enhancement. Ultrasound-guided core needle biopsy revealed spindle cell proliferation consistent with leiomyoma of the nipple.
Leiomyoma is a benign tumor of smooth muscles. It is most commonly diagnosed in the uterus, small intestine, and esophagus. It is very rarely reported in the breast. Since most of the breast lesions originate from smooth muscles in the nipple, these tumors are located in the subareolar region (1). Only 31 cases of leiomyoma of the nipple have been reported to date (2).
The mammographic and sonographic features of nipple leiomyoma have been described. However, to the best of our knowledge, nipple leiomyoma magnetic resonance imaging (MRI) findings have not been reported before.
Herein, we present a rare case of a leiomyoma of the nipple that was examined by MRI.
Case report
A 32-year-old woman visited the surgery outpatient clinic in our hospital with a recently enlarged left nipple with discharge and erosion. The patient has been aware of the asymmetrically prominent left nipple for 6 years.
She did not have fever at the time of the visit, and no history of breast trauma. Additionally, there was no family history of breast cancer. On physical examination, she had a 2-cm pinkish superficial nodule in the left nipple-areolar complex. The nodule was firm and quite tender. The remainder of the breast examination revealed no abnormalities. The laboratory findings were normal.
The left mediolateral oblique mammogram revealed an enlarged nipple (Fig. 1). Ultrasonography of the left breast showed a 2-cm sized well-circumscribed oval hypoechoic mass with posterior acoustic enhancement in the nipple (Fig. 2a). A Doppler sonogram of the left nipple mass demonstrated increased peripheral blood flow in the mass (Fig. 2b). No other abnormal findings were seen neither by mammography nor ultrasonography.
A 32-year-old woman with leiomyoma of the nipple. A left mediolateral oblique mammogram shows an enlarged nipple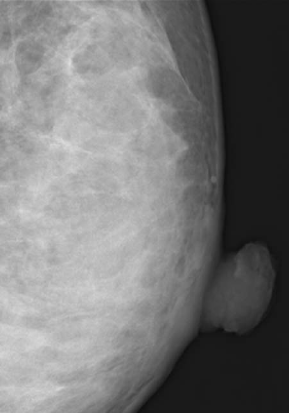
A 32-year-old woman with leiomyoma of the nipple. (a) Ultra-sonography of the left breast shows a well-circumscribed, ovoid, hypoechoic mass with posterior acoustic enhancement of roughly 2 cm in the nipple. (b) A Doppler ultrasound sonogram of the left nipple mass demonstrates increased peripheral blood flow in the mass
To exclude abnormalities in the subareolar region since the parenchyma in this patient was extremely dense, breast MRI was performed.
MRI revealed an oval mass with circumscribed margins in the left nipple-areolar complex. This mass showed intermediate signal intensity on both T2-weighted images (Fig. 3a) and T1-weighted images (Fig. 3b). A dynamic MRI study showed a peripheral rim enhancement (Fig. 3c). The mass in the left nipple-areolar complex had a higher diffusion-weighted imaging (DWI) signal intensity and lower apparent diffusion coefficient (ADC) value than the right nipple (Fig. 3d). A kinetic curve demonstrated delayed persistent enhancement (Fig. 3e). No other abnormal findings were observed.
(a) An axial T2-weighted image demonstrates an intermediate signal intensity mass in the left nipple. (b) An axial fat-suppressed T1-weighted image demonstrates an intermediate signal intensity mass in the left nipple. (c) An axial contrast-enhanced T1-weighted image demonstrates a rim-enhancing mass in the left nipple. (d) Diffusion-weighted imaging (DWI) shows a high intensity lesion (arrow), and an apparent diffusion coefficient (ADC) image shows a low signal intensity (arrow) in the nipple. The ADC value was 1.28 × 10−3. (e) The kinetic curve demonstrates delayed persistent enhancement
An ultrasound-guided core needle biopsy was performed using a 14-gauge needle. The core needle biopsy demonstrated spindle cell proliferation consistent with leiomyoma of the nipple (Fig. 4).
Pathology shows (H&E x40) a well-demarcated tumor consisting of interlacing bundles of smooth muscle cells in the dermis
Finally, on the basis of the histopathological and radiological findings, this case was diagnosed as leiomyoma of the nipple.
Discussion
Leiomyoma of the nipple was first described by Virchow in 1854 (3). The condition is rare, and as far as we could ascertain, only 31 cases have been reported in the literature, 10 of which have been in men and 21 in women (2). Leiomyoma of the nipple may be asymptomatic for long periods; it can also present as a mass or with recurrent spontaneous severe pain on pressure application or after exposure to cold (4). Pain is also a common feature of cutaneous leiomyoma occurring in locations other than the nipple, and is thought to be due to contraction of neoplastic smooth muscles (4). Examination may reveal a single, small, firm subcutaneous papule that enlarges the nipple. Our patient presented with an enlarged left nipple with discharge and erosion.
The mammographic appearance of a nipple leiomyoma has been reported as having spiculated margins and being associated with localized skin thickening (5) or as an enlarged nipple (6). In our case, the mammographic appearance of the leiomyoma showed an enlarged nipple compared with the contralateral nipple.
A previously published sonography finding has reported leiomyoma to be well-marginated and slow growing with isoechoic and slightly hyperechoic features that lack increased blood flow (7). Posterior echoes may be lacking, decreased, or slightly enhanced. In our case, the tumor was a well-circumscribed, hypoechoic lesion with posterior acoustic enhancement.
However, no reports of MRI findings of a nipple leiomyoma have been published. In our case, the MRI showed a circumscribed oval mass that appeared with intermediate signal intensity on both T1- and T2-weighted images. A dynamic MRI study showed a rim-enhancing oval mass with delayed persistent enhancement. Findings of leiomyoma of the breast on MR images are an oval circumscribed lesion of high intensity in both T1- and T2-weighted images with a gradual increasing pattern after gadolinium administration (8).
The differential diagnoses of nipple leiomyoma are adenomas, solitary intraductal papillomas, and Paget's disease of the nipple. Adenoma of the nipple (erosive adenomatosis, papillary adenoma, florid papillomatosis) is a rare neoplasm that arises from the lactiferous ducts and milk sinuses (9). On MR images, adenoma of the nipple appears with focal, intense enhancement within the nipple on contrast-enhanced T1-weighted images. Additionally, the tumor usually shows calcifications in the subareolar breast tissue and within the nipple on mammography. These findings are helpful for differential diagnosis.
Solitary intraductal papillomas are discrete benign tumors of the mammary duct epithelium. By MRI, intraductal papillomas often present as small smooth masses with strong enhancement with type 2 (initial rapid increase in signal intensity, followed by less than 10% change in signal intensity in the delayed phase) or type 3 (initial rapid increase in signal intensity, followed by more than 10% reduction in signal intensity in the delayed phase) time intensity curves (10). Intraductal papillomas often present as small, smooth masses, dilated ducts, or micro-calcifications by mammography and as smooth, homogenously hypoechoic intraductal masses within a dilated duct by ultrasonography.
Paget's disease of the breast is a rare pathology of the nipple-areola complex that is often associated with an underlying in situ or invasive carcinoma. On MR images, Paget's disease of the nipple often appears as an abnormal nipple enhancement and linear clumped enhancement indicative of ductal carcinoma in situ in association with Paget's disease (11). Paget's disease shows malignant calcifications at the level of the nipple or elsewhere in the breast, skin thickening, nipple retraction, and a discrete mass or masses in mammography.
In conclusion, we report a rare case of a leiomyoma of the nipple examined by MRI. MRI revealed an oval mass with circumscribed margins that appeared as an intermediate signal intensity on both T1- and T2-weighted images. A dynamic MRI study showed a gradual enhancement pattern with peripheral rim enhancement on the mass.