
Abstract
Background
Plasma alphafetoprotein (AFP) concentrations are high at birth and decline progressively to reach adult levels between eight and 24 months of age. AFP is an important tumour marker for hepatoblastoma but may also increase following hepatic resection. The liver and intestine have similar embryonic origins from endoderm, so we postulated that plasma AFP may also rise after extensive bowel resection.
Methods
AFP was measured postoperatively in plasma in four infants who had undergone resections of large amounts of intestine. AFP was measured twice in two babies and multiple times in the other two.
Results
In three of the four infants, the AFP concentrations were markedly above the expected levels for age, and in all four babies, AFP concentrations rose when they may have been expected to fall.
Conclusion
Rising plasma AFP concentrations post extensive bowel resection in infants is a new finding which is possibly due to intestinal regeneration.
Introduction
Alphafetoprotein (AFP) is synthesized predominantly in hepatocytes after the eighth week of gestation. 1 At birth, plasma concentrations of AFP are very high, with a mean value of approximately 40,000 kIU/L in term infants2,3 and 131,000 kIU/L in premature babies. 3 Thereafter, in normal babies, plasma AFP concentrations fall progressively and reach adult levels between eight and 24 months of age.2,3
A postnatal rise in AFP is considered to indicate underlying pathology. Marked elevations occur in infants who develop hepatoblastoma. 4 Smaller rises are seen in neonatal hepatitis, intra- and extrahepatic cholestasis, ataxia telangiectasia and with regeneration of hepatocytes following hepatic necrosis.5–7
We recorded marked rises in plasma AFP concentration in four infants who underwent substantial bowel resection. This is an as yet unpublished cause of increasing plasma AFP levels following birth.
Patients and methods
During the years 2006-2011, four infants born between 32 and 40 completed weeks of gestation required laparotomy and subsequent resection of necrotic small and/or large bowel greater than 150 mm (6 inches) in length. Postoperative care was individualized for each infant and all received total parenteral nutrition (TPN) as part of management. Blood samples were collected on the orders of the attending medical staff for the purpose of patient management and, for this study, estimations of plasma AFP were performed where superfluous serum samples were available for analysis. Approval to undertake a more formal study of plasma AFP concentrations following extensive gut resection was also obtained from the Ethics Committees of the Institutions involved.
We measured plasma AFP levels (in kIU/L) in these infants on various occasions, ranging between 9 and 305 days, following their surgery. AFP was measured in singlicate (with dilutions, as required) using three different analysers, according to the institution and year of analysis. The analysers were an AxSym, an Architect i2000 (both from Abbott Laboratories, Abbott Park, IL, USA) and a Siemens Advia Centaur (Siemens Medical Solutions Diagnostics, Walpole, MA, USA). Coefficients of variation (CV) for AFP concentrations greater than l00 kIU/L for the three instruments were as follows: AxSym 6.8%, Architect 3.0% and Centaur 5.7%.
Pearson correlation was used to compare log AFP concentrations with bilirubin and alanine aminotransferase (ALT) values.
Results
The highest recorded AFP result for each infant and the lowest result prior to the increase are shown in Table 1, together with clinical and outcome data, plus liver function tests (LFTs). In Figure 1, each AFP result is plotted on a graph which also shows the expected decline of AFP values postnatally in premature and term infants. All four subjects show unexpected rises in AFP, and in patients 1, 2 and 4, all results are much higher than expected for corrected postnatal age. Following the recorded peak levels in infants 3 and 4, the concentrations declined with half-lives of 8.0 and 8.4 days, respectively.
Plasma alphafetoprotein (AFP) concentrations are expressed as logarithmic values on they axis. For each subject (indicated by number) there is a line linking all the infant's recorded AFP values. The straight line, derived from data from a cohort of premature and term babies,
8
indicates the expected decline in AFP concentration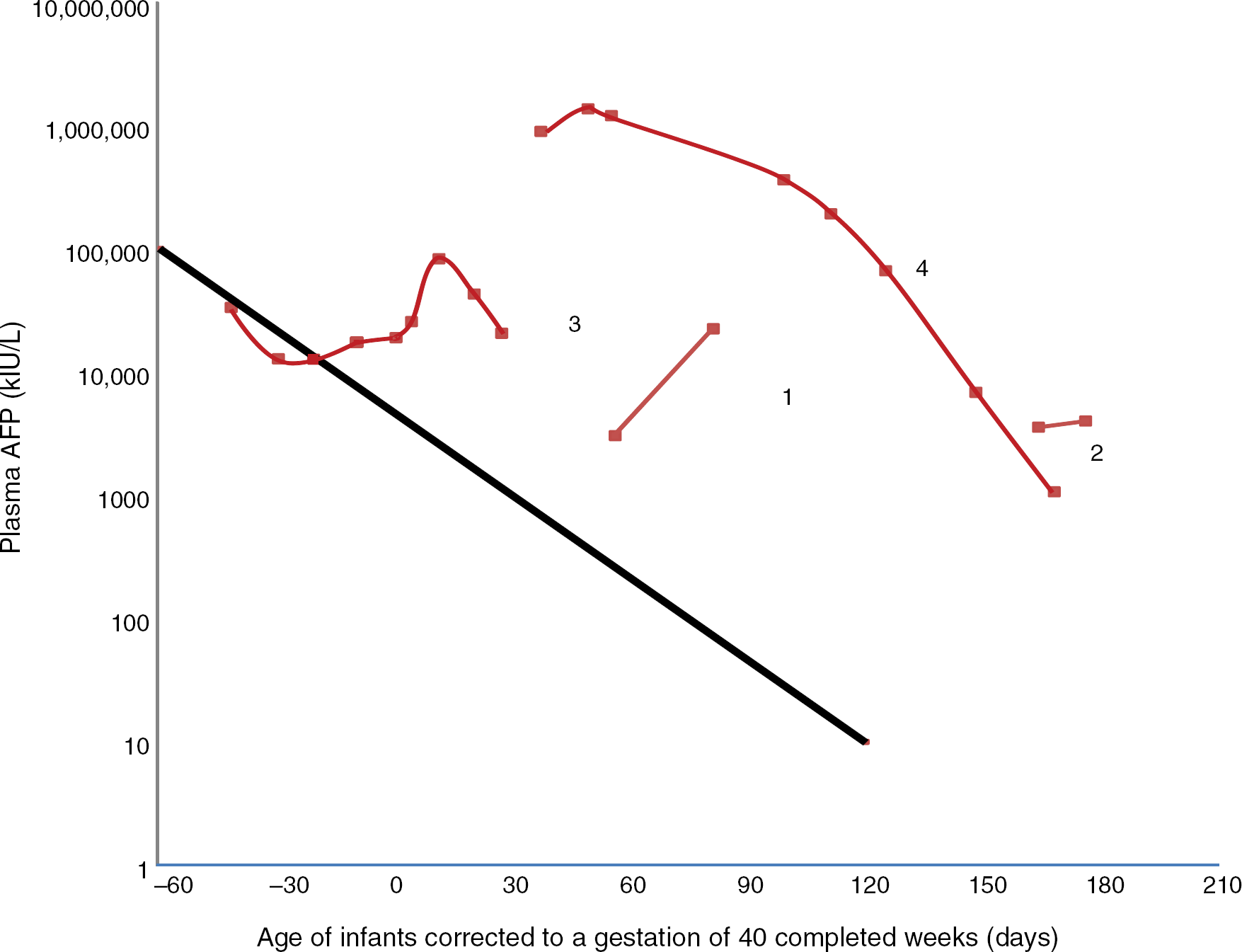
Summary of the clinical and biochemical features of the four infants
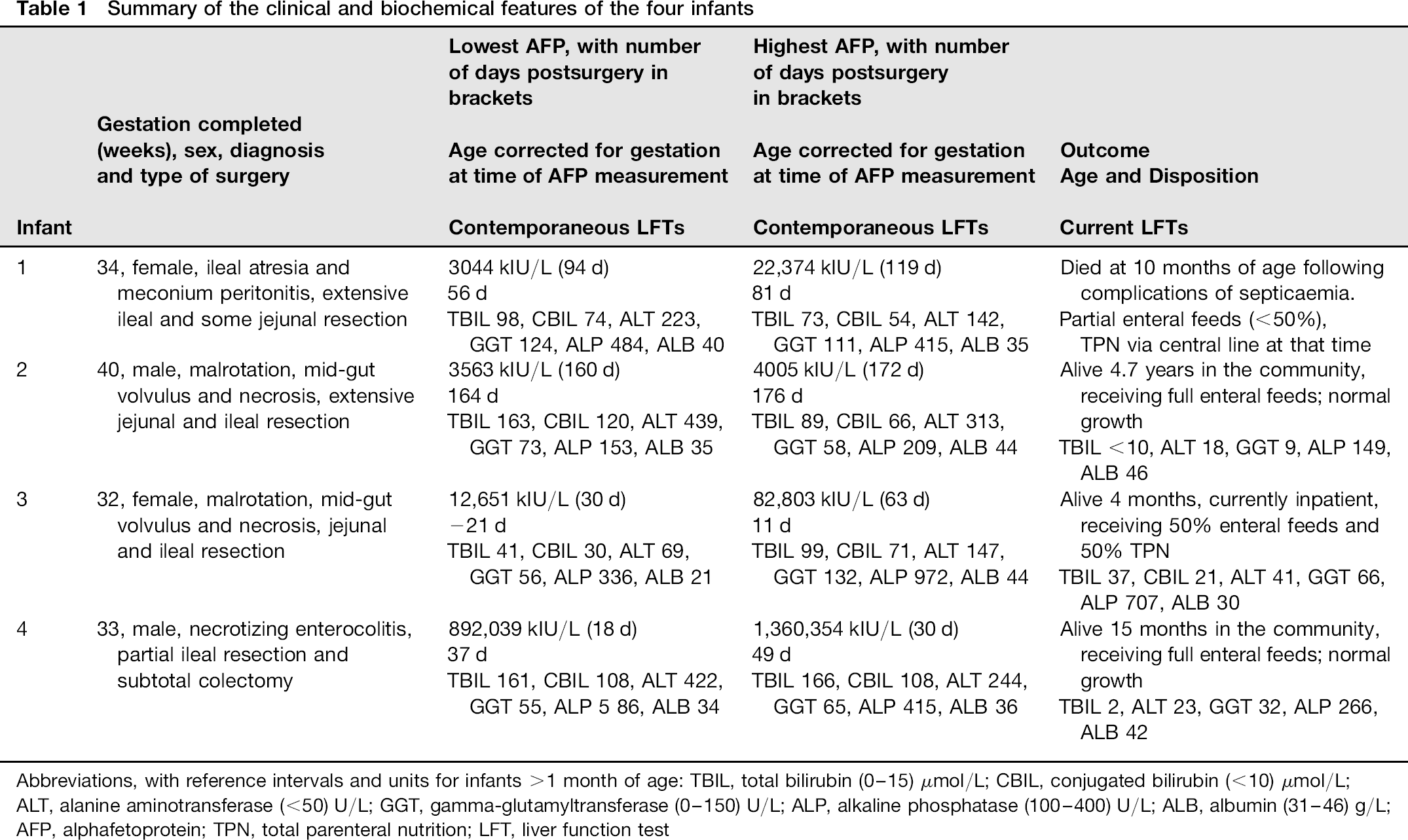
Abbreviations, with reference intervals and units for infants >1 month of age: TBIL, total bilirubin (0-15) μmol/L; CBIL, conjugated bilirubin (<10) μmol/L; ALT, alanine aminotransferase (<50) U/L; GGT, gamma-glutamyltransferase (0-150) U/L; ALP, alkaline phosphatase (100-400) U/L; ALB, albumin (31 -46) g/L; AFP, alphafetoprotein; TPN, total parenteral nutrition; LFT, liver function test
LFTs documented during the postoperative period for each infant were deranged, in keeping with cholestasis associated with the use of TPN. However, LFTs done at the time of the highest AFP measurement showed improvement over prior LFTs in infants 1 and 2 and little change in infant 4. In Figures 2 and 3, all the AFP results are plotted against contemporaneous total bilirubin (BILT) concentrations and ALT activities. The Pearson coefficient for correlation between log AFP and ALT was not significant (r = 0.302, P = 0.183), while for log AFP versus bilirubin, it just reached significance (r = 0.440, P = 0.046).
Log alphafetoprotein (AFP) concentrations plotted against contemporaneous total bilirubin (TBIL) concentrations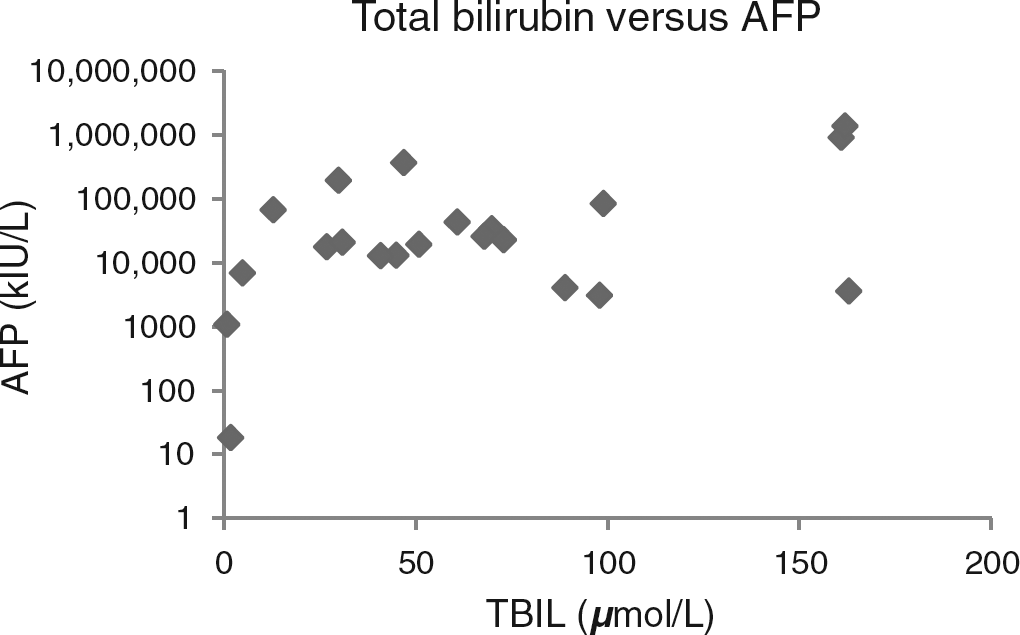
Log alphafetoprotein (AFP) concentrations plotted against contemporaneous alanine aminotransferase (ALT) activities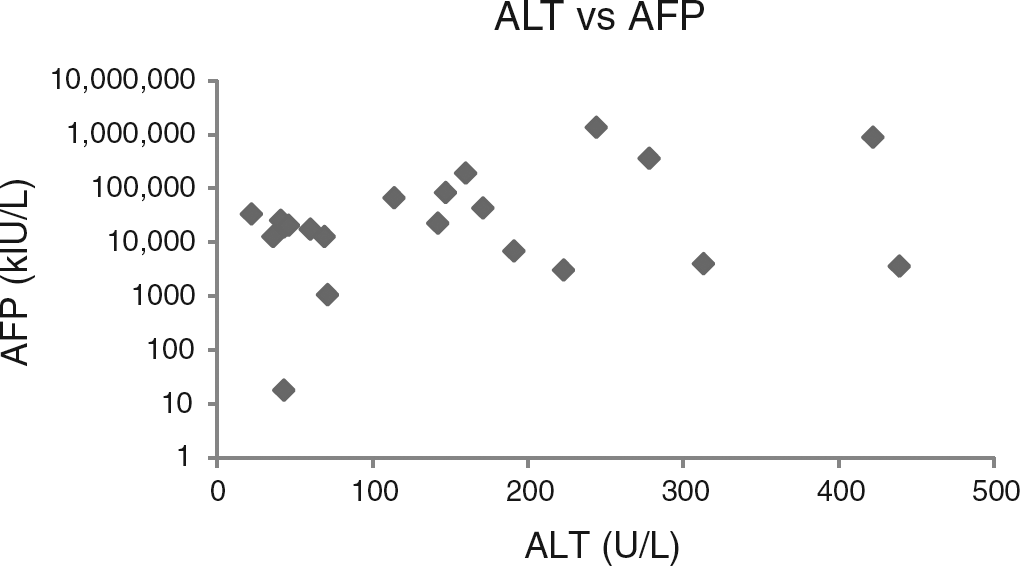
The outcomes for these infants, as of May 2012, are as follows. Infant 1 died at 10 months chronological age (8 months corrected age) from septicaemia while still a hospital inpatient receiving a combination of enteral and parenteral nutrition. Infant 2 is over four years of age, tolerating and growing on full enteral feeds with documented normal LFTs. Infant 3 remains an inpatient receiving 50% of calories and fluids enterally. Infant 4 is 15 months old (13 months corrected age) with normal LFTs and is tolerating full enteral feeds. His last plasma AFP level (18 klU/L) is in the normal range for his age.
Discussion
In considering the reasons for the elevated plasma AFP concentrations in this study, we have eliminated the stress of surgery as a possible cause, as AFP is not an acute phase reactant. 4 The prolonged follow-up periods in patients 2 and 4 show that hepatic tumours or chronic hepatopathies did not cause their abnormal AFP concentrations. In addition, in patient 4, we have documented a significant rise, then spontaneous fall in AFP levels to the normal range.
It may be argued that the very high AFP levels seen in our patients were due to transient derangement of liver function consequent upon TPN-induced cholestasis. Review of previous literature regarding AFP and liver disease does not support this contention. In a series of infants with intra-and extrahepatic cholestasis, AFP concentrations were reported to overlap with the normal reference range. 9 Andres et al. 10 reported a mean AFP concentration of 42,900 kIU/L in seven patients with neonatal hepatitis under the age of four months and 8200 kIU/L in 24 infants with biliary atresia. These investigators re-assayed one patient diagnosed with neonatal hepatitis whose AFP concentration fell from 170,500 kIU/L at one month of age to 25 kIU/L over four weeks. This pattern is in sharp contrast to the persistently high and rising AFP values seen in patient 3 over a period of 33 days and patient 4 who had levels >850,000 kIU/L measured on three occasions over 18 days.
We therefore postulate that these novel findings are due to a regenerative process in the intestine of infants recovering from acute intestinal necrosis. As both intestine and liver are derived from endoderm, it seems plausible that bowel regeneration could cause a transient rise in postnatal plasma AFP concentration, just as occurs with liver regeneration. Further research, perhaps using animal models, with histological staining for AFP presence in the remaining intestine following extensive bowel resection, would be needed to confirm this hypothesis. At this preliminary stage, we wish to notify other biochemical laboratories of this unusual phenomenon and encourage them to confirm our findings.
Declarations
Footnotes
Acknowledgements:
We thank Dr Rod Hunt, Director of Neonatal Medicine, Royal Children's Hospital, Melbourne, for providing results and clinical details on infant 4.