
Abstract
Background
Inflammatory states are known to cause an imbalance in the redox status. We aimed to study the possible associations between pro-oxidant-antioxidant balance (PAB) and serum high-sensitive C-reactive protein (hs-CRP) concentrations and traditional cardiovascular disease (CVD) risk factors in an unselected Iranian population and in groups of individuals with specific disease.
Methods
The study was conducted among an unselected population of 758 male subjects. Biochemical markers, including hs-CRP and PAB values, were measured.
Results
Serum hs-CRP concentrations were positively associated with serum PAB values (r = 0.260, P ≤ 0.001). Univariate analysis showed that PAB values were statistically higher in individuals who were obese or smokers compared with non-obese and non-smokers individuals (P < 0.01). While serum hs-CRP concentrations were significantly higher in older subjects, subjects with obesity, diabetes mellitus, metabolic syndrome, central obesity, hypertriglyceridaemia, higher low-density lipoprotein cholesterol concentrations, positive history of CVD and lower physical activity than subjects without these risk factors (P < 0.05). Comparing hs-CRP and PAB values in different CVD risk score subgroups showed a significant incremental rise in both parameters as CVD risk score increased (P < 0.05). Using multiple linear regression analysis we found a strong association between PAB values and hs-CRP concentrations.
Conclusions
This study showed that among Iranian subjects, the inflammatory marker, hs-CRP, was strongly and positively associated with a marker of oxidative stress and also with several traditional risk factors of CVD. Moreover, the impact of traditional cardiovascular risk factors on hs-CRP concentrations and PAB values differed.
Introduction
Cardiovascular disease (CVD) is one of the leading causes of death and disability worldwide. 1 The major traditional risk factors for CVD are hypertension, diabetes mellitus, cigarette smoking, advanced age, elevated serum total and low-density lipoprotein cholesterol (LDL-C) and low levels of high-density lipoprotein cholesterol (HDL-C). These risk factors are usually used for the evaluation of predisposition to CVD. 2 However, these established risk factors account for no more than 25-30% of the excess cardiovascular risk, 3 suggesting that other risk factors play an important role in the pathogenesis of atherosclerosis. In recent decades, oxidative stress, 4 inflammation 5 and immune responses 6 have also been considered to be significant risk factors for vascular events.
Oxidative stress is defined as an imbalance between the production of pro-oxidants and antioxidant defenses in favour of pro-oxidants. This imbalance is usually related to the increased reactive oxygen species (ROS) formation, and plays a pivotal role in the development and pathogenesis of CVD and several other pathologies. In patients with CVD, elevated levels of both oxidative stress status parameters (superoxide anion
Despite the diversity of the methods available for estimating oxidative stress, there is no consensus on a universally accepted method to be used in routine clinical practice, or indeed whether this would be clinically useful. We have developed a method which can measure the balance of oxidants and antioxidants simultaneously, by using 3,3’,5,5'-tetramethylbenzidine (TMB) and two different kinds of reactions: 8 one enzymatic reaction where the chro-mogen, TMB is oxidized to a coloured cation by peroxides, and another chemical reaction whereby the TMB cation is reduced to a colourless compound by antioxidants; and this then gives a redox index. It should be noted that the pro-oxidant-antioxidant balance (PAB) assay has been calibrated against some of the most significant known oxidants and antioxidants. A linear decrease in the PAB value has been observed in association with increasing major antioxidants such as bilirubin, albumin, vitamin C, trolox, glutathione, uric acid and ceruloplasmin. On the other hand, increasing concentrations of pro-oxidants such as tert-butylhydroperoxide, hydrogen peroxide, chloramine T and hypochlorite were associated with a linear increase of the PAB value in vitro. The values of the PAB are expressed in arbitrary Hamidi-Koliakos (HK) units, which represent the percentage of hydrogen peroxide in the standard solution. PAB values were found to be correlated with urea, serum creatinine and bilirubin, while there was no correlation with some other parameters such as uric acid.8,9
High concentrations of serum C-reactive protein (CRP) indicate systemic inflammation 10 and CRP is now believed to play a contributory role in CVD. 11 Furthermore, CRP has been positively related to future cardiovascular events in high-risk individuals, and we 12 have previously shown that CRP is associated with CVD in Iranian patients with angiographically defined coronary artery disease (CAD). High-sensitive (hs)-CRP concentrations were found to independently predict the frequency of recurrent coronary events in patients with acute coronary syndromes. 13
We have previously found high levels of inflammatory markers 12 and also PAB values in patients with angiographically defined CAD. 14 It has previously been reported that oxidative stress may be a determinant of CRP concentrations, and may also promote the proatherosclerotic inflammatory process. 15 Moreover, there is some evidence that the systemic response to inflammation may lead to an increase in oxidized lipids in serum and in the enhancement of the oxidative modification of low-density lipoprotein. 16 Elucidating the inter-relationship between inflammation, oxidative stress and traditional risk factors may be beneficial in the management of populations at high risk of CVD, as these emerging risk factors also play an important role in the pathogenesis of CVD.12,14 Thus, we have evaluated the possible associations between PAB values, a marker of oxidative state, and hs-CRP as a marker of systemic inflammation in an unselected Iranian population.
Materials and methods
Study population
This survey was conducted among 758 men aged 20-69 years old who were employees of Shahid Hasheminejad Gas Processing Company (S.G.P.C), Sarakhs, Iran. All demographic and socioeconomic data including age, gender, residual information, educational and marital status, occupational and smoking data were collected using an interviewer-administrated questionnaire. Participants were provided with information about the study both verbally and by written information sheets. Those who had exclusion criteria such as poorly controlled diabetes, severe hypertension, overt signs/symptoms of CVD, endocrine abnormalities, or who preferred not to participate at any point were withdrawn from the study. Each patient gave informed written consent to participate in the study, which was approved by the Mashhad University of Medical Science Ethics Committee. The investigation conformed to the principles outlined in the Declaration of Helsinki.
Anthropometric and other measurements
For all patients, body weight (BW), body mass index (BMI) and body fat mass were measured by body composition analyzer BC-418 (Tanita, Tokyo, Japan) according to a standard protocol. 17 Height and body weight were measured with the subjects dressed in light clothing after an overnight fasting. The body weight of each subject was measured with a standard scale to an accuracy of ± 0.1 kg, and height was measured to an accuracy of ± 0.1 cm. Hip circumference (HC) was measured at the levels of the major trochanters through the pubic symphysis. Waist circumference was measured mid-way between the lateral lower rib margin and the iliac crest with the scale to the nearest ± 0.1 cm. The BMI was calculated as weight (kg) divided by height squared (m2).
Blood sampling
Blood samples were taken from each subject after 12 h of fasting. Following venepuncture, blood samples were collected into Vacutainer® tubes and centrifuged at 5000g for 15 min at 4°C. After separation, aliquots of serum were frozen at — 80°C until analysis. A full fasted lipid profile comprising total cholesterol, triglycerides, HDL-C and LDL-C was determined for each subject. Serum lipid and fasting blood glucose (FBG) concentrations were measured enzymatically with the use of commercial kits using the BT-3000 auto-analyzer machine (Biotechnica, Rome, Italy). hs-CRP was measured by a polyethylene glycol (PEG)-enhanced immunoturbidimetry method using an Alcyon® analyzer (Abbott, Chicago, IL, USA).
Chemicals and determination of pro-oxidant-antioxidant balance assay
TMB powder (Fluka, Buchs, Switzerland), peroxidase enzyme (Applichem: 230 U/mg; A3791,0005, Darmstadt, Germany), chloramine T trihydrate (Applichem: A4331), hydrogen peroxide (30%) (Merck, Darmstadt, Germany). These agents and all the other reagents used were of reagent grade and were prepared in double-distilled water. 18
PAB assay
A modified PAB assay was applied based on a previously described method. 19 The standard solutions were prepared by mixing varying proportions (0-100%) of 250 μmol/L hydrogen peroxide with 3 mmol/L uric acid (in 10 mmol/L NaOH). Sixty-milligrams TMB powder were dissolved in 10 mL dimethylsulphoxide (DMSO); for preparation of TMB cation, 400 μL of TMB/DMSO was added to 20 mL of acetate buffer (0.05 mol/L buffer, pH 4.5), and then 70 μL of fresh chloramine T (100 mmol/L) solution was added into this 20 mL, mixed well, and incubated for two hours at room temperature in a dark place; 25 U of peroxidase enzyme solution was added to 20 mL TMB cation, dispensed in 1 mL and stored at —20°C; in order to prepare the TMB solution, 200 μL of TMB/DMSO was added into 10 mL of acetate buffer (0.05 mol/L buffer, pH 5.8); the working solution was prepared by mixing 1 mL TMB cation with 10 mL of TMB solution, incubated for two minutes at room temperature in a dark place and immediately used. Ten microlitres of each sample, standard or blank (distilled water), were mixed with 200 μL of working solution, in each well of a 96-well plate, which was then incubated in a dark place at 37°C for 12 min; at the end of the incubation time, 100 μL of 2 mol/L HC1 was added to each well; and measured in an ELISA reader at 450 nm with a reference wavelength of 620 or 570 nm. A standard curve was provided from the values relative to the standard samples. The values of the PAB are expressed in arbitrary HK units, which represent the percentage of hydrogen peroxide in the standard solution. The values of the unknown samples were then calculated based on the values obtained from the above standard curve.
Physical activity level
Physical activity level (PAL) of subjects was assessed using a standard questionnaire modified from the SHHS/ MONICA questionnaire, 20 which was coded using the Human Energy Requirement proposed by James and Schofield. 21 According to the PAL values, subjects were classified to extremely inactive (PAL <1.40), sedentary (1.40-1.69), moderately active (1.70-1.99), vigorously active (2.00-2.40) or extremely active (>2.40) subgroups.
Risk factor definitions
The reference population was categorized into different subgroups including smokers and non-smokers, diabetics and non-diabetics, obese and non-obese, dyslipidaemics and non-dyslipidaemics, metabolic syndrome and non-metabolic syndrome cases and finally hypertensive and non-hypertensive subjects. The following conventional cardiovascular risk factors were defined: obesity as BMI ≥30 (kg/m2), dyslipidaemia (total cholesterol ≥200 mg/dL and/or LDL-C ≥130 mg/dL and/or use of cholesterol-lowering drugs), diabetes (FBG ≥126 mg/dL and/or use of pharmacological treatment), arterial hypertension (systolic blood pressure >140 mmHg and/or diastolic blood pressure >90 mmHg and/or use of antihypertensive drugs). 22
The American Heart Association/National Heart, Lung and Blood Institute (AHA/NHLBI) guideline was used to categorize subjects into metabolic syndrome positive and negative subgroups. 23 Metabolic syndrome was defined as the co-occurrence of at least three of the following five metabolic abnormalities: (1) elevated serum fasting glucose (≥100 mg/dL) or use of medication for hyperglycaemia; (2) elevated serum triglycerides (≥150 mg/dL); (3) reduced serum HDL-C (<40 mg/dL in men); (4) elevated systolic (≥130 mmHg) or diastolic (≥85 mmHg) blood pressure or use of medication for hypertension; and (5) elevated waist circumference (≥102 cm in men). Finally, 10-year CVD risk was also measured using National Cholesterol Education Program (NCEP) and Adult Treatment Panel (ATP III) protocol. 24
Statistical analysis
All statistical analyses were performed using the SPSS for Windows™, version 16 software package (SPSS Inc., Chicago, IL, USA). Data were expressed as means (SD) for parameters with a normal distribution or median (interquartile range) for non-normally distributed data. Group comparisons were performed using sample t-test (for normally distributed data) or Mann-Whitney test (for non-normally distributed data). A two-sided P value <0.05 was considered statistically significant. Bivariate correlations between different parameters and serum hs-CRP and PAB values were performed using Spearman's rank correlation. Stepwise multiple linear regression analysis was used to determine which of the conventional risk factors and biochemical markers influences serum hs-CRP and PAB values.
Results
A total of 758 subjects were studied. Clinical and biochemical characteristics and the prevalence of some disease conditions have been summarized in Table 1 for the subjects. There were 116 (15.3%), 503 (66.4%), 72 (9.5%) and 228 (30.1%) subjects with hypertension, dyslipidaemia, diabetes mellitus and metabolic syndrome, respectively.
Demographic and biochemical characteristics of participants (n = 758)
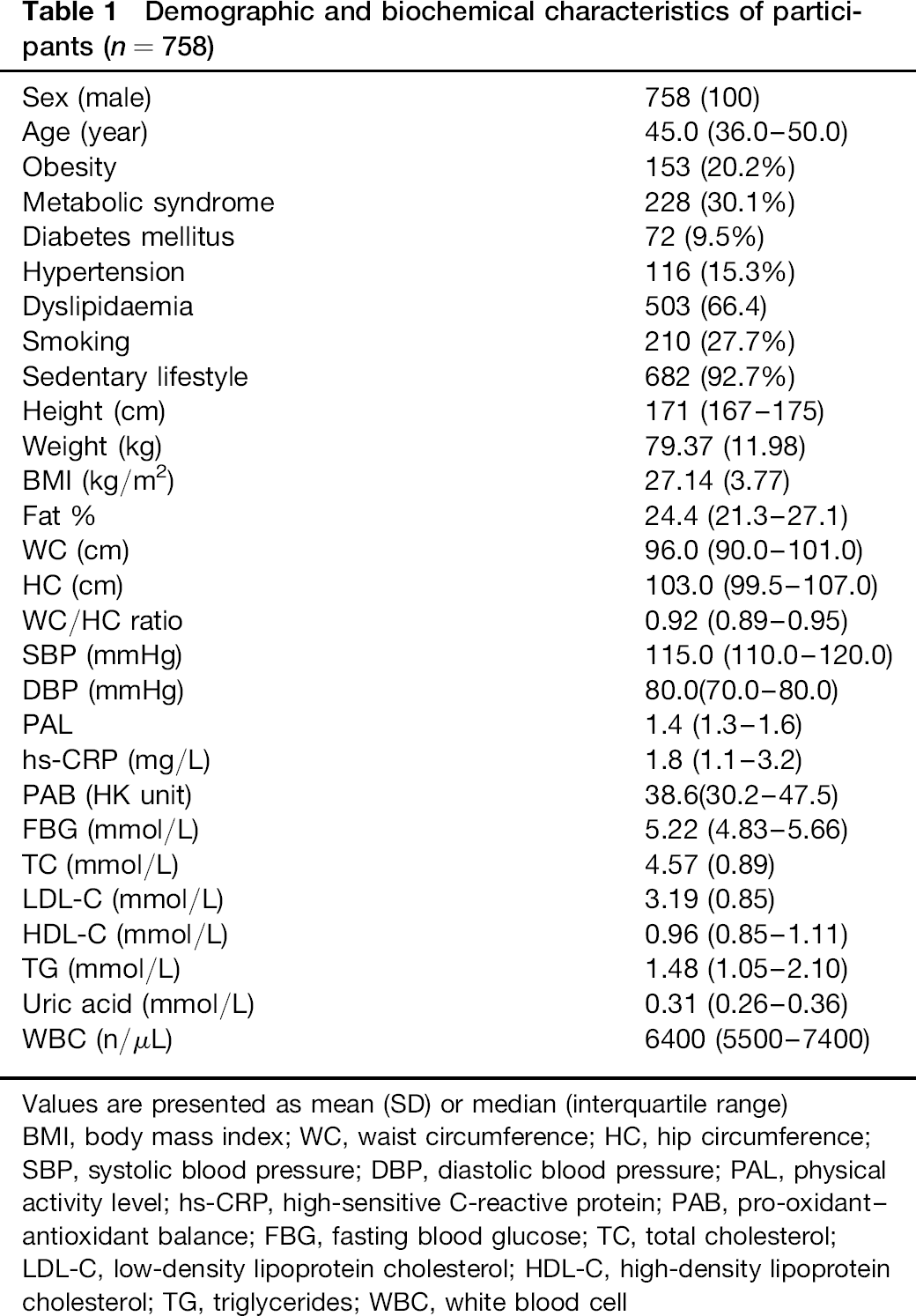
Values are presented as mean (SD) or median (interquartile range) BMI, body mass index; WC, waist circumference; HC, hip circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; PAL, physical activity level; hs-CRP, high-sensitive C-reactive protein; PAB, pro-oxidant-antioxidant balance; FBG, fasting blood glucose; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides; WBC, white blood cell
Spearman's correlation test showed that hs-CRP was strongly associated with PAB values (r = 0.260, P ≤ 0.001). Likewise, hs-CRP concentrations were positively associated with fasting blood glucose, uric acid, total and LDL-C, triglyceride, white blood cell (WBC), systolic blood pressure, fat percentage, BMI and weight, while with PAL score, HDL-C an inverse correlation was found. PAB values were also positively associated with BMI, weight, waist and hip circumference, WBC and number of cigarettes smoked per day. Table 2 summarizes the correlations between PAB values and hs-CRP concentrations with other biochemical factors.
Association between hs-CRP and PAB values with other factors among participants
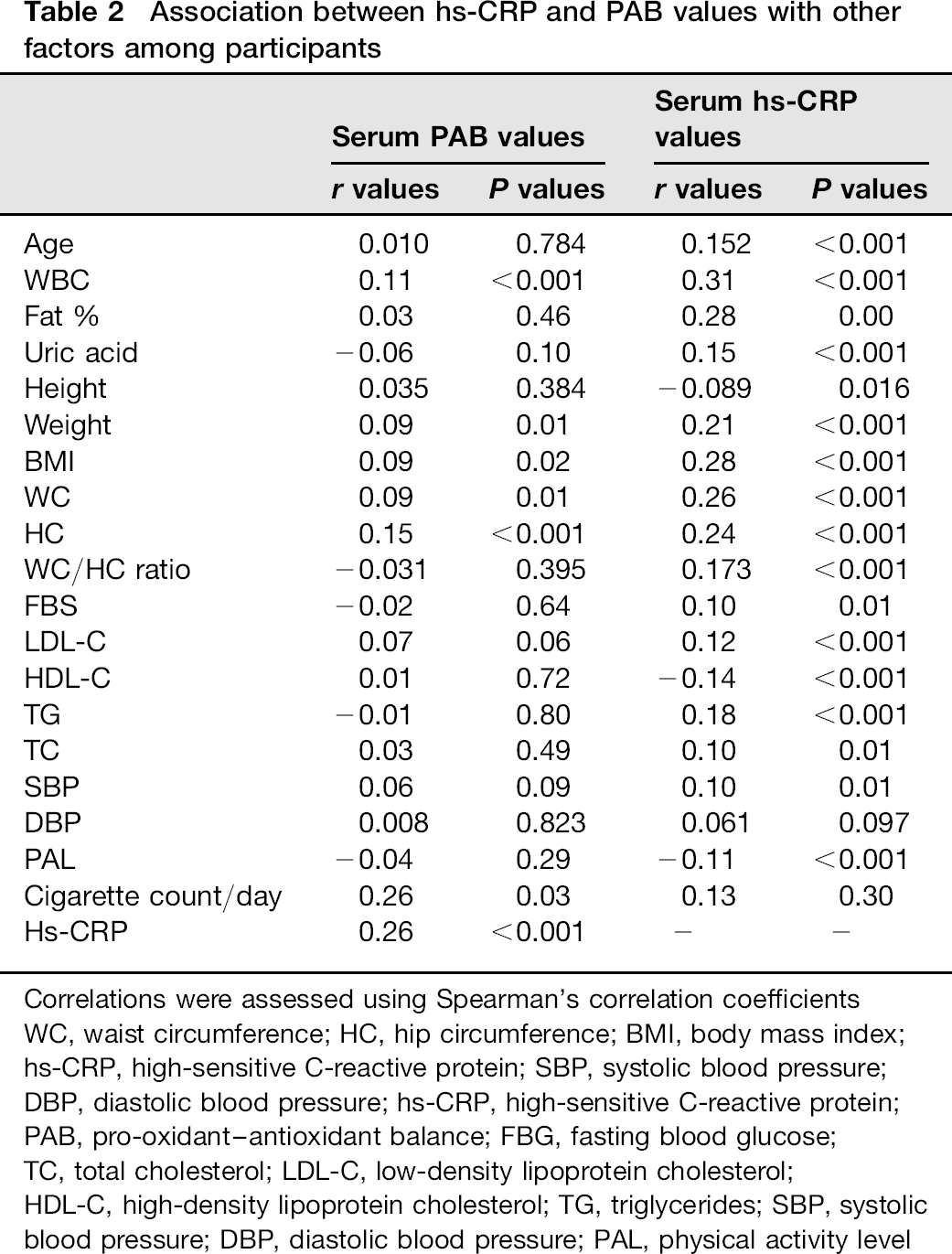
Correlations were assessed using Spearman's correlation coefficients WC, waist circumference; HC, hip circumference; BMI, body mass index; hs-CRP, high-sensitive C-reactive protein; SBP, systolic blood pressure; DBP, diastolic blood pressure; hs-CRP, high-sensitive C-reactive protein; PAB, pro-oxidant-antioxidant balance; FBG, fasting blood glucose; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides; SBP, systolic blood pressure; DBP, diastolic blood pressure; PAL, physical activity level
When univariate analyses were performed between those subjects with and without traditional risk factors for PAB values and hs-CRP, we found that PAB values were statistically different between obese and non-obese, smokers and non-smokers, and between subjects with positive and negative personal history of myocardial infarction (MI) (P < 0.01). PAB values were not significantly different for other parameters, including metabolic syndrome and diabetes mellitus. The univariate analysis for hs-CRP concentrations showed that this inflammatory marker was significantly different in older subjects (P < 0.001), subjects with obesity (P < 0.001), diabetes mellitus (P < 0.001), metabolic syndrome (P < 0.001), central obesity (P < 0.001), hypertriglyceridaemia (P < 0.001), for those with higher levels of LDL-C (P < 0.01), lower levels of HDL-C (P < 0.05), individuals with a positive history of MI (P< 0.001) and low physical activity (P< 0.001). Hypertension was not significantly associated with PAB or hs-CRP values (P > 0.05). Comparing hs-CRP and PAB values in different CVD risk score subgroups showed a significant stepwise increase in both factors as CAD risk score increases (P < 0.05) (Figure 1).
Risk assessment for determination of 10-year CAD risk developing according to panel NCEP ATP III: 613 (81.1 %), 115 (15.2%) and 29 (3.8%) subjects were categorized in group 1 (<10%), group 2 (10-20%) and group 3 (>20%), respectively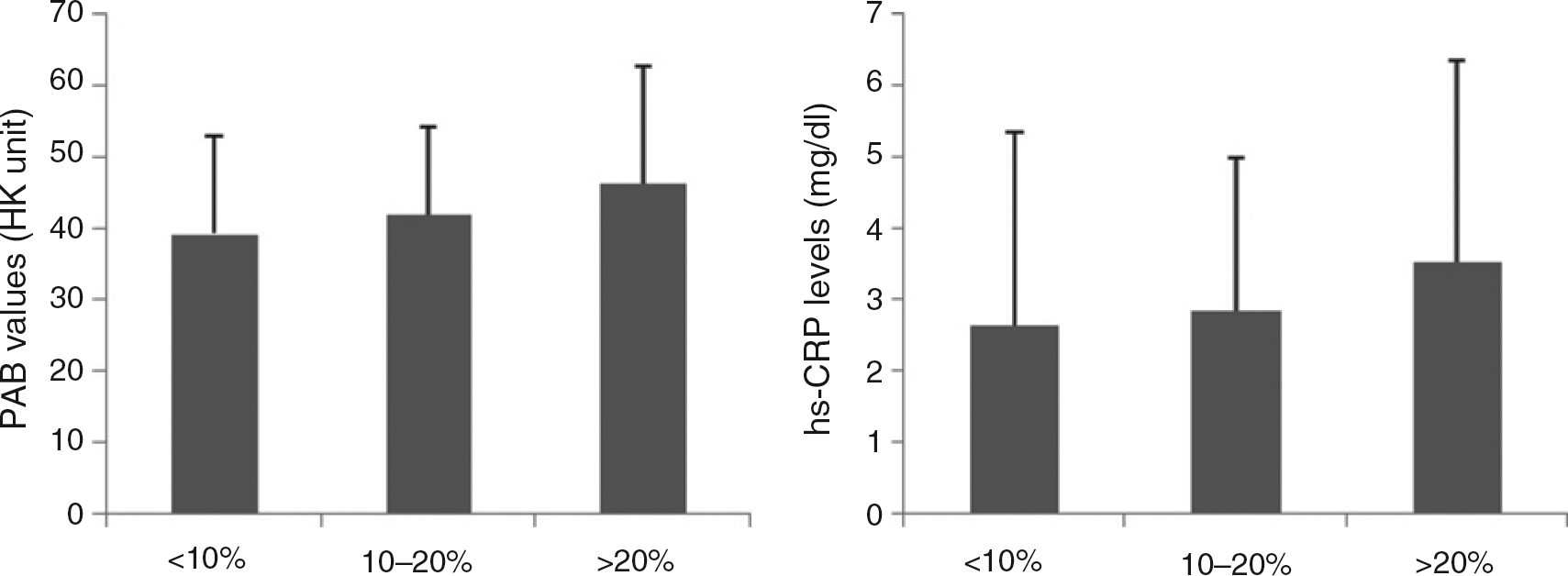
Finally, multiple linear regressions were performed in order to find the determinants of PAB values. The stepwise regression showed that hs-CRP (β = 2.501, P < 0.001) and BMI (β = -1.289, P = 0.012) were significant determinants of serum PAB values. Stepwise regression was also performed for determining the important factors for hs-CRP concentrations. The analysis showed that PAB values (β = 0.073, P< 0.001), fat % (β = 0.124, P = 0.004), uric acid (β = 0.299, P = 0.013) and WBC (β = 0.281, P = 0.029) had a significant effect on hs-CRP concentrations.
Discussion
This study was undertaken to determine the association between serum hs-CRP concentrations and a marker of oxidative stress, PAB values, and generalized and abdominal obesity, body fat composition, the presence of the metabolic syndrome and other traditional cardiovascular risk factors within an Iranian population. Our results indicate that hs-CRP were strongly and positively correlated with PAB values.
When patients with and without traditional risk factors for CVD were evaluated for PAB and hs-CRP values, we found that only smoking and obesity had a significant effect on the marker of oxidative stress, while for hs-CRP values patients with metabolic syndrome, central obesity, hypertriglyceridaemia and lower physical activity had higher levels of hs-CRP. Moreover, regression analysis showed that PAB and hs-CRP concentrations have significant associations with each other. These results imply a significant inter-relationship between oxidative stress, inflammation and traditional cardiovascular risk factors. PAB values were also positively associated with BMI, weight, waist and hip circumference. hs-CRP concentrations were positively associated with PAL score, FBG, uric acid, total and LDL-C, triglycerides, systolic blood pressure, fat percentage, BMI and weight, while with HDL-C an inverse correlation was found.
Other previous studies have reported similar findings, implying that oxidative stress is significantly associated with inflammation. In a study by Dohi et al. 25 investigating the association between CRP, oxidative stress and traditional risk factors in 551 healthy Japanese subjects, they found that CRP concentrations were positively correlated with age, male gender, BMI, blood pressure, smoking habit, creatinine, uric acid, triglycerides and 8-isoprostane, and inversely correlated with HDL-C. Moreover, they found that 8-isoprostane, the marker of oxidative stress, was positively correlated with age, pulse pressure, smoking habit and CRP. Similar to our results, they found in regression analysis that BMI, HDL-C, uric acid and 8-isoprostane were independently correlated with CRP. In another study, among 512 Iranian youths (aged 10-18 years), the authors found a significant association between CRP and oxidative stress markers in healthy young people. hs-CRP and the marker of oxidation, MDA concentrations, were also significantly related with the measure of abdominal obesity. 26
Increased levels of serum CRP have been previously reported among adults with metabolic syndrome, especially in women. 27 The higher levels of hs-CRP in subjects with lower levels of HDL-C, and an inverse association between hs-CRP concentrations and HDL-C is in accordance with previous studies that support the antiinflammatory properties of this lipoprotein, as Cockerill et al. 28 have reported for HDL-C in vitro. We found higher hs-CRP concentrations in patients with lower physical activity. This is in agreement with previous reports indicating the reduction in proinflammatory cytokines such as plasma levels of interleukin-6, tumour necrotizing factor-a and CRP, and increase in plasma levels of adiponectin and interleukin-10 as anti-inflammatory cytokines occur in physically active individuals compared with physically inactive groups.29–32 In addition, it has been demonstrated that long-term exercise significantly attenuates the production of proinflammatory cytokines, while it enhances the anti-inflammatory cytokines in individuals at risk of developing CVD. 33
We have found that hs-CRP concentrations are associated with central and generalized obesity; these results have been previously reported by others. 34 In another study, in an Asian Indian population, a significant correlation of CRP with BMI and waist circumferences in adolescents and young adults was found. 35 Previous studies have also reported higher levels of oxidative stress in obese subjects in comparison with healthy ones.36,37 In an animal study, it has been demonstrated that fat accumulation correlates with markers of systemic oxidative stress in mice. 37 Moreover, a population-based study among adults revealed that abdominal fat accumulation is associated with oxidative stress. 38
Our results shows that in the general population, elevation in PAB and hs-CRP values is associated with an incremental rise in CAD risk score, suggesting that these two factors may have a predictive value. Previous studies have reported that high levels of oxidative stress in combination with high levels of inflammation are predictive of a significant deterioration in endothelial function. 39 Prospective epidemiological studies have shown that high levels of serum CRP are related with increased risk of cardiovascular events and this association becomes even stronger as CRP concentrations increase.13,40 However, it has been reported that using the combination of inflammatory and oxidative markers has the strongest risk prediction power when compared with each of these markers alone. 41
As the results show, even within the reference ranges of inflammatory and oxidative stress markers, values for hs-CRP and PAB may predict the risk of future cardiovascular events. Thus, it may be useful to assess the risk of future CVD in the general population and in subjects with a higher risk of disease, medication therapy such as statins be initiated in order to reduce the risk of disease.
Although there are alternative methods for determining body oxidative status, the PAB assay used in this study to measure the redox state showed its potential as a biomarker of CVD risk. This assay is cheap and easy to use without any technical complexity. We were unable to find a significant association between oxidative stress and the majority of traditional risk factors except smoking and obesity. Similar results have been previously reported in a Japanese population. 25
We found positive association between WBC and PAB, which clearly supports the concept of PAB being associated with inflammation. This is consistent with previous reports implying in some clinical conditions such as essential hypertension and uraemia known to be associated with endothelial dysfunction and accelerated atherosclerosis. Polymorphonuclears are activated and may contribute to oxidative stress and inflammation,42,43 and this is supported by other human and animal studies.44,45
Another interesting finding was the fact that uric acid (measured in part by the PAB assay) correlates with CRP but not PAB values. The correlation between CRP and uric acid is in accordance with previous reports, as it has been previously found that in vascular smooth muscle cells, uric acid is able to induce inflammatory mediators such as CRP and also activates nuclear factor-κB.46,47 However, the association between PAB values and uric acid levels is controversial, which may be caused in part by measuring different markers, as the PAB assay is able to measure the PAB simultaneously, which others can not. It has been speculated that uric acid is produced via the action of xanthine oxidase, an enzyme that is implicated in oxidative processes,48,49 thus it may be possible that uric acid is a marker of inflammation and oxidative stress but, depending on the cellular environment, it may have pro-oxidant or antioxidant properties.49–51
Cigarette smoking was correlated with PAB but not CRP in our study. The association between oxidative stress and smoking is in agreement with previous reports. Agarwal 52 found that plasma and urinary MDA and CRP were significantly increased in smokers reflecting the heightened state of oxidative stress and inflammation. It has been reported that 32 weeks of cigarette smoking in mice was associated with increased leukocyte-specific ROS generation. 53 In a cross-sectional study among subjects recruited by the Physicians’ Health Study, the authors found that plasma levels of CRP were significantly associated with smoking in a stepwise manner, with the number of cigarettes smoked per day correlating with CRP concentrations. 54 However, there are also some reports that have reported the same results as ours, as Tracy et al. 55 found no direct association between the numbers of cigarettes smoked per day and CRP concentrations in a cross-sectional study.
The fact that HDL-C correlates negatively with CRP but not PAB suggests that HDL-C may have an antiinflammatory role, although it is also thought to have antioxidant 56 anti-inflammatory properties. 57 This may be because the PAB assay probably has a bias towards measuring lipophilic antioxidants.
In conclusion, this study showed that among Iranian male subjects, the inflammatory marker hs-CRP is strongly and positively associated with an oxidative stress marker and also with traditional clinical risk factors. These results confirm the results of previous studies25,26 that support the use of oxidative stress and hs-CRP concentrations as markers of CVD risk. Moreover, the impact of traditional cardiovascular risk factors on hs-CRP concentrations and PAB values differed. The lesser association between traditional risk factors and PAB values may indicate that oxidative stress has an independent role in eliciting an antiinflammatory response. One of the limitations of the present study was that we assessed the association between inflammatory and oxidative stress levels in male subjects alone. However, future longitudinal studies are essential to demonstrate whether outcomes are improved when PAB and hs-CRP values are measured together for prognostic assessment and therapeutic decision-making.
Declarations
Footnotes
Acknowledgements
We are particularly grateful to the subjects who volunteered to participate in this study. The results presented in this work have been taken from Akramsadat Razavi's thesis in MUMS, with the following ID number: 89337.