
Abstract
Background
Previous studies have shown that of all the tests requested of hospital laboratories, 25-40% are thought to be unnecessary. Our hospital laboratory observed that a significant number of requests from the medical admissions unit (MAU) were probably inappropriate. In an attempt to improve requesting behaviour this observation was investigated and an educational intervention employed.
Methods
We performed a survey of requesting behaviour by the MAU and a local protocol was designed as an audit standard. The influence of the educational intervention on requesting behaviour was audited.
Results
The generation of local guidelines and an educational intervention to promote them, significantly changed requesting behaviour. The main effect was the reduction in requesting of thyroid function tests, lipid profiles and coagulation screens.
Conclusions
This process highlighted inappropriate requesting behaviour from the MAU which, following a process of investigation and education, resulted in a significant change with an associated cost benefit.
Introduction
Previous studies have shown that of all the tests requested of hospital laboratories, 25-40% are thought to be unnecessary. 1 The number of potentially unnecessary requests varies per practitioner, hospital and country and the definition of what is deemed to be unnecessary. 2 Within biochemistry, the number of unnecessary tests has been shown to be between 26% and 98%. 1
Biomedical scientists in our laboratory observed that there were a significant number of requests generated by the medical admissions unit (MAU) which were unlikely to be clinically indicated given the acute nature of the patients admitted there. A retrospective review of requesting data was performed from September 2008 until August 2009, to identify whether this was the case and three request sets were identified - thyroid profile, lipid profile and coagulation screen, as being potentially inappropriately requested. The MAU is based in a district general hospital and admits on average 950 patients per month. Patients presenting with suspected poisoning were admitted directly to a separate specialist ward. The biochemistry laboratory received a mean of 7156 set requests per month over this time period, including a mean of 309 thyroid profiles per month, 481 lipid profiles per month (with a mean of 28.9% of these profiles including HDL-cholesterol) and 818 coagulation screens.
Methods
Following initial data analysis, the patient journey through the MAU was observed. It was clear that the majority of requests were made at the time of triage and the request forms and phlebotomy were completed by nursing staff. The three request sets were confirmed as not clinically appropriate following discussion between laboratory staff (BND) and the lead medical consultant in the MAU. Following this, in agreement with the medical teams, a local protocol for requesting was agreed. This protocol was applied to all medical admissions to our hospital, apart from those admitted to the poisons unit. During August 2009, a laboratory-led educational intervention was delivered to the clinical staff, and posters illustrating the protocol were displayed (Figure 1a). The author (BND) delivered two educational sessions to the nursing and health-care support workers for the unit and presented the protocol and subsequent audit data to the Medical Directorate Governance and Safety meeting. The use of the protocol was encouraged by senior nursing staff and the lead MAU medical consultant. The tests available to nursing staff to request were as follows: full blood count, urea, electrolytes and creatinine, liver function tests, bone profile, glucose, C-reactive protein and prothrombin time (if the patient was taking warfarin). No specific protocol for other commonly requested tests from the admissions unit, such as troponin or d-dimer was implemented; however, staff were encouraged to only request these in the context of a relevant clinical presentation. All requests were made on paper request forms. If further requests were made by the medical staff after senior clinical review an additional test request form was sent to the laboratory and analysis carried out on the original sample. There was no IT intervention performed and the educational input was not repeated. Requests from either nursing or medical staff were never refused by biomedical scientist staff, on either the initial or subsequent requests.
(a) Agreed requesting protocol poster displayed within the medical admissions unit. (b)The monthly data for the 12 months preceding the educational intervention and then the following 12 months are displayed. The arrow indicates the point of intervention. The results of the paired t-test are also displayed for the different profiles analysed. U + E, urea and electrolytes; LFT, liver function test; CRP, C-reactive protein; FBC, full blood count; INR, international normalized ratio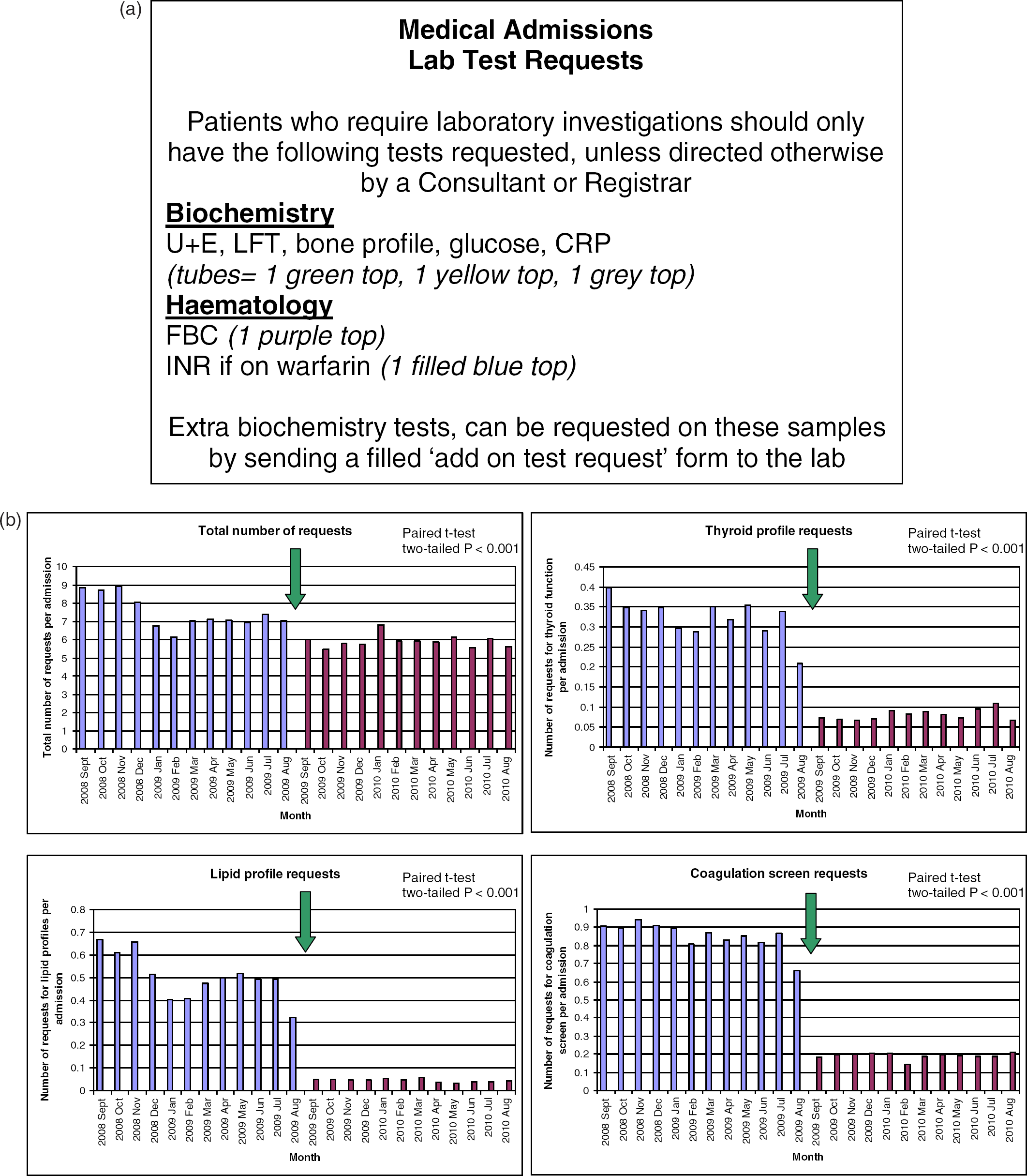
An audit was performed assessing requesting behaviour, using the requesting protocol as the audit standard during the subsequent 12 months.
Results
The number of requests made before and after the intervention were compared calendar month-for-calendar month (to allow for any seasonal variation), divided by the number of admissions in that month using a two-tailed paired t-test. This comparison showed a significant change between the total number of sets requested per admission before (mean = 7.5, SD = 0.87) and after the intervention (mean = 5.9, SD = 0.33), P < 0.001. There was also a significant reduction in the mean number of requests per admission for the three particular profiles highlighted as being over-requested: thyroid profile from 0.32 (SD = 0.05) to 0.08 requests per admission (SD = 0.01), P < 0.001; lipid profile from 0.50 (SD = 0.10) to 0.04 requests per admission (SD = 0.01), P < 0.001; and coagulation screen from 0.85 (SD = 0.07) to 0.19 requests per admission (SD = 0.02), P < 0.001 (Figure 1b). There appeared to be an initial reduction in requesting between late 2008 and early 2009. We were unable to identify a specific reason to explain this observation, but we have noted some seasonal variation in requesting in previous years, thought to be related to junior doctor changeover.
Conclusions
This study showed that an educational intervention can effectively influence requesting behaviour and hence improve quality use of pathology. Previous education-based strategies have resulted in 38% reductions in biochemistry requests. 1 The impact of the intervention was not only financial (with an estimated saving of ∼ £12,000 per year in marginal costs) but also resulted in more appropriate requesting and hence improved patient care. There would have been time saved for doctors interpreting any inappropriately requested results, and then the saving of any further unnecessary investigations due to misinterpretation. Resources would have been saved, for example the coagulation test tubes.
Our observation was that this educational intervention was well received and valued by nursing staff, who had previously found test selection difficult, due to lack of guidance. Prior to the education they had not perceived that for most admissions the profiles we have highlighted were generally not required by the medical staff. It appears that this has been important in sustaining the value of a limited intervention. Future work will look at presentation specific request panels in order to assess if this can further improve appropriate test selection.
In one critical review of demand management, it is suggested that for modifying test-requesting behaviour, education and training are invaluable; however the biggest challenge besides achieving changes is to maintain them. 2 Barth et al. 3 suggested in their study that local protocols to change requesting behaviour can be implemented but suggested that an aide-mémoire is also necessary. In our study, the effect of a single educational intervention, reinforced by a poster which remained on display, was associated with quality improvement which was sustained over the subsequent 12 months.
In a district general hospital with a similar system of triage and requesting in their admissions units it may be possible to perform a similar intervention to us. This would have potential cost-savings but also improve the quality use of pathology.