
Abstract
Background
Transjugular intrahepatic portosystemic shunts (TIPSs) have become a widely accepted tool in the treatment of patients with symptomatic portal hypertension. The aim of our study was to assess the value of cardiac markers before and after TIPS insertion for the prediction of one-year mortality in cirrhotic patients.
Methods
The study population consisted of 55 patients (38 men and 17 women, aged 55.6 ± 8.9 y, range 37-74) with liver cirrhosis treated with transjugular portosystemic shunting. Biochemical markers were measured before and 24 h after TIPS. High-sensitivity cardiac troponin T (hs-cTnT) was tested by high-sensitivity immunoassay for Elecsys analyser (Roche Diagnostics). Concentrations of creatine kinase MB isoenzyme, myoglobin (MYO), glycogenphosphorylase BB isoenzyme (GPBB) and heart type of fatty acid binding protein (FABP) were measured by the Evidence Investigator protein biochip system (Randox Laboratories).
Results
In patients before TIPS insertion, hs-cTnT was increased above the cut-off (0.014 μg/L) in 39.2% of patients. Higher hs-cTnT and FABP concentrations were associated with poor survival in patients before TIPS (hs-cTnT: P = 0.018; FABP: P = 0.016). Twenty-four hours after the TIPS procedure, we found a significant elevation in serum GPBB in comparison with preprocedural values (P < 0.001). There was an association between postprocedural concentrations of cardiac markers (MYO, hs-cTnT, FABP) and overall survival.
Conclusions
Measurement of cardiac markers, mainly hs-cTnT and FABP, may be useful for mortality prediction in cirrhotic patients after TIPS. Cardiac markers are better mortality predictors than other risk factors such as age, gender or Child-Pugh score.
Introduction
It has been known for more than four decades that liver cirrhosis is associated with cardiovascular abnormalities. 1 Cardiovascular complications of cirrhosis include cardiac dysfunction and abnormalities in the central, splanchnic and peripheral circulation, as well as haemodynamic changes caused by humoral and nervous dysregulation. Cirrhotic cardiomyopathy implies systolic and diastolic dysfunction and electrophysiological abnormalities. 2
The transjugular intrahepatic portosystemic shunt (TIPS) is a decompressive treatment for portal hypertension. It is based on the creation of intrahepatic connection between the portal vein and the right hepatic vein. TIPS has significant effects on systemic haemodynamics. It rapidly shifts a large volume of blood from the splanchnic area to the heart, thus increasing cardiac preload. 3 TIPS is thus an important stressful haemodynamic stimulus.
The clinical significance of cardiovascular complications of TIPS and cirrhotic cardiomyopathy is an important research topic. 2 Several studies have reported changes in echocardiography and haemodynamic monitoring results after TIPS insertion.1,4,5 Diastolic dysfunction has been associated with poor survival in patients with cirrhosis and TIPS. 3
Some authors have detected alterations in cardiac markers in cirrhotic patients. On the other hand, no studies published so far have measured cardiac necrosis markers in relation to TIPS procedures. In cirrhotic patients, levels of natriuretic peptides are elevated due to their increased cardiac release.6–8 Similarly, cardiac troponin I, a troponin isoform increased in myocardial injury, has been reported to be elevated in patients with predominantly alcoholic cirrhosis. 9
The prediction of the outcome of patients treated with TIPS is important, because some patients will have a very short survival after the procedure. 3 The armamentarium of cardiac markers has expanded to include several molecules that are potentially useful for the diagnosis of cardiac injury and are awaiting validation for routine clinical applications. 10 These novel analytes include glycogen Phosphorylase BB isoenzyme and heart-type fatty acid-binding protein.11,12
The aim of our study was to assess the prognostic value of cardiac markers before and after TIPS insertion for the prediction of one-year mortality in cirrhotic patients.
Materials and methods
Study population
The study population consisted of 55 consecutive patients (38 men and 17 women, age 55.6 ± 8.9 y, age range 37-74) with liver cirrhosis treated with elective TIPS. The causes of liver disease were alcohol consumption in 36 (65%) patients, viral hepatitis in seven (13%) patients, nonalcoholic steatohepatitis in six (11%) patients, autoimmune hepatitis in two (4%) patients and unknown in four (7%) patients. Baseline patient characteristics are shown in Table 1. Patency of the shunt was evaluated using Doppler ultrasound of the liver tissue during regular follow-up appointments. All patients were in stable condition, with no known gastrointestinal bleeding in the 15 days preceding TIPS insertion. Medication affecting hae-modynamics, such as β-blockers and vasodilators, was stopped for at least 10 days before TIPS. Diuretics were maintained in a constant dose during the week before TIPS insertion. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, and was approved by the ethical committee of our institution. Informed consent was obtained from each patient. We have assessed mortality (all-cause mortality, without sub-classification) from the central hospital data register.
Patient demographic characteristics
NASH, non-alcoholic steatohepatitis
Biochemical analysis
Serum cardiac markers were measured in peripheral venous blood before and 24 h after the procedure. Blood samples were obtained by venepuncture, immediately shipped to the laboratory and centrifuged (2500 g, 10 min) within one hour of collection. Serum samples were stored at − 70°C until analysis (within 9 months).
Cardiac troponin T was measured by high-sensitivity electrochemiluminiscence imunoassay using the Troponin T hs STAT assay for Elecsys 2010 analyser (Roche Diagnostics, Mannheim, Germany). 13 The high-sensitivity cardiac troponin T (hs-cTnT) assay had an analytical range from 0.003 to 10 μg/L. The cut-off value according to the manufacturer was 0.014 μg/L (the 99th percentile of healthy reference population values, n = 616, coefficient of variation [CV] = 9.0%).
Concentrations of other cardiac markers were determined by the Evidence Investigator protein biochip system (Randox Laboratories, Crumlin, UK). The cardiac array included the following markers: creatine kinase MB isoenzyme (CKMB), myoglobin (MYO), glycogenphosphorylase BB isoenzyme (GPBB) and heart type of fatty acid binding protein (FABP). Concentrations of all cardiac markers are given in μg/L. The assay analytical parameters (analytical range, cut-off value) were as follows: CKMB: 0.4-100 μg/L, 3.9 μg/L; MYO: 1.8-700 μg/L, 59.0 μg/L; GPBB: 2-290 μg/L, 7.3 μg/L; and FABP: 0.15-150 μg/L, 4.5 μg/L. The inter-assay coefficients of variability (n = 10) were in accordance with data provided by the manufacturers in the range of CV = 2.0-9.8% with the exception of MYO assay where the measured CV was 11.6-15.6% (CKMB: 3.9 μg/L - 7.5%, 30.9 μg/L - 8.6%; MYO: 86.3 μg/L -13.5%, 120.7 μg/L - 15.6%; GPBB: 8.4 μg/L - 6.6%, 68.1 μg/L - 7.9%; FABP 3.2 μg/L - 5.0%, 43.8 μg/L -8.7%). Internal quality control measurements were carried out using samples provided by the kit manufacturers.
Statistical analysis
Serum cardiac marker concentrations are reported as median and interquartile range. Normality was tested by chi-square test. Statistical comparisons were carried out using the paired Wilcoxon test (data with non-normal distribution). Degree of data association was tested by the rank correlation test. The survival curves were generated as univariable Kaplan-Meier estimates. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated by constructing first a univariable and subsequently a multivariable Cox proportional hazards regression model, with survival time as the dependent variable. For all tests, P = 0.05 was considered to be statistically significant. We used receiver operator characteristic (ROC) analysis for assessing prognostic power of parameters.
Results
Child-Pugh score was used for assessing the severity of liver cirrhosis (Table 1). Child-Pugh score is a validated tool for assessing cirrhosis severity and prognosis.14,15 This score employs five clinical measures of liver disease - serum bilirubin, albumin, ascites, hepatic encephalopathy and international normalized ratio for prothrombin time (INR). Each measure is scored 1-3, with 3 indicating most severe derangement.
Serum concentrations of cardiac markers in patients before and 24 h after TIPS are shown in Table 2. During baseline measurement in patients before TIPS insertion, hs-cTnT was increased above the 99th percentile of healthy reference population (0.014 μg/L) in 39.2% patients. Serum FAPB, GPBB and MYO were increased in 25.0%, 12.0% and 10.7% of patients. CKMB was below the limit of detection (<0.4 μg/L) in most patients.
Table 2 Serum concentrations of cardiac markers (μg/L): median (interquartile range)
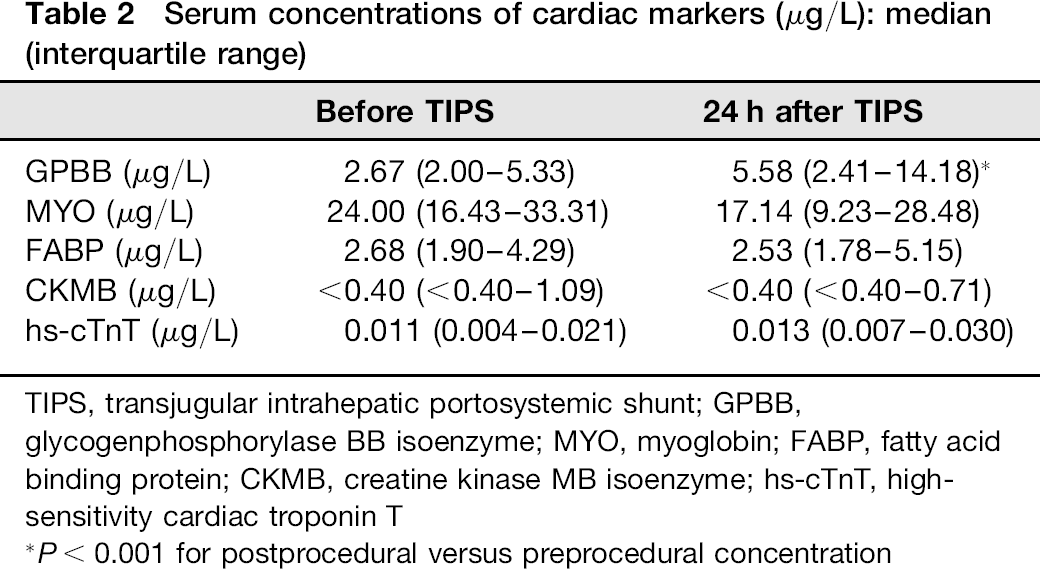
TIPS, transjugular intrahepatic portosystemic shunt; GPBB, glycogenphosphorylase BB isoenzyme; MYO, myoglobin; FABP, fatty acid binding protein; CKMB, creatine kinase MB isoenzyme; hs-cTnT, high-sensitivity cardiac troponin T
P< 0.001 for postprocedural versus preprocedural concentration
Twenty-four hours after the TIPS procedure, we detected significant elevation in serum GPBB concentration compared with preprocedural values, with 40% of patients having concentrations above the cut-off value of 7.3 μg/L (P < 0.001) (Table 2). There were no significant changes in the concentrations of other cardiac markers after TIPS. There was a significant correlation between pre- and postprocedural serum FABP and hs-cTnT and patient age (P = 0.005).
We investigated the predictive value of cardiac marker concentrations for one-year mortality. Univariable Cox regression analysis demonstrated no statistically significant association between one-year mortality and Child-Pugh score, gender or age (Table 3). However higher hs-cTnT and FABP concentrations before TIPS were associated with poor survival (Table 3, Figure 1). Spearman correlation coefficients between the marker concentrations and the survival time were as follows: hs-cTnT, r = — 0.480 (P < 0.001); FABP, r= -0.347 (P = 0.012). The survival was significantly better in patients with cardiac marker concentrations below the median (hs-cTnT: 0.011 μg/L; FABP: 2.92 μg/L) compared with patients with higher levels. Statistical significance was calculated by log-rank test with the following P values: hs-cTnT, P = 0.018; FABP, P = 0.016. Figure 2 shows the corresponding Kaplan-Meier survival curve for hs-cTnT. No significant association was found between mortality and preprocedural serum GPBB and MYO concentrations. ROC analysis for one-year mortality showed that preprocedural serum FABP (area under curve [AUC] = 0.76) and serum hs-cTnT (AUC = 0.74) had the best prognostic value (Figure 3). AUC for the other risk factors - age and Child-Pugh score - were 0.61 and 0.59, respectively (Figure 3).
Association of preprocedural high-sensitivity cardiac troponin T (hs-cTnT) with survival time, hashed lines - 95% confidence interval, solid lines - 95% prediction interval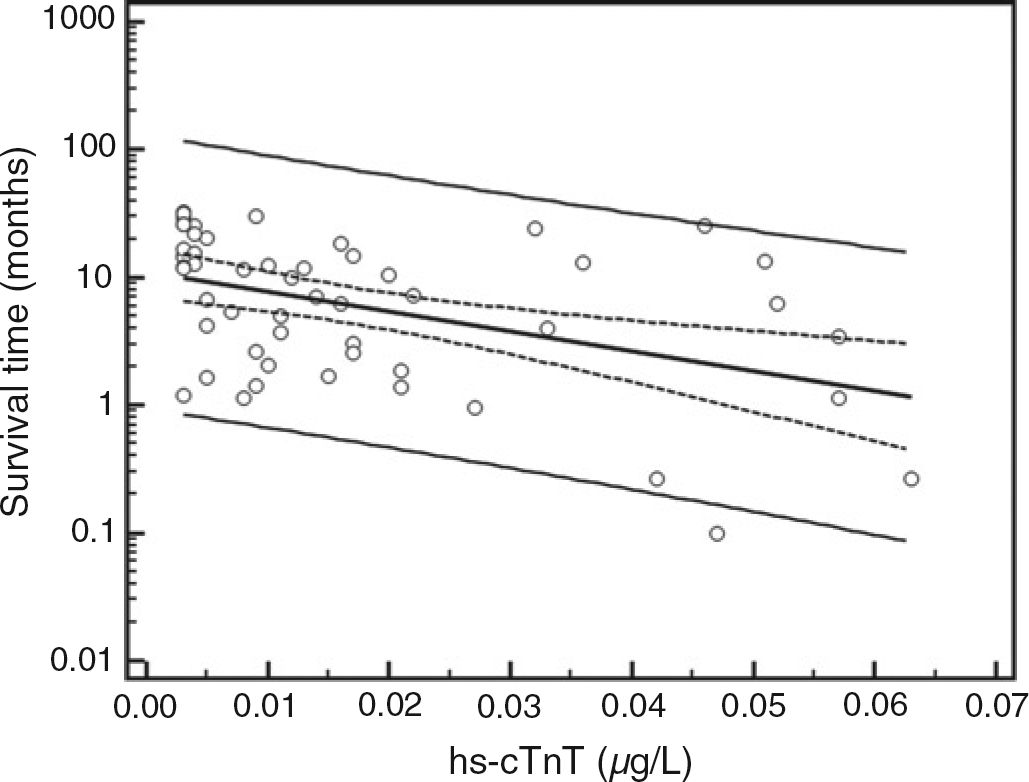
Kaplan-Meier survival curve of preprocedural highly sensitive cardiac troponin T (hs-cTnT) (μg/L). We used the median 0.011 μg/L as the differentiator, line 1: hs-cTnT < median, line 2: hs-cTnT > median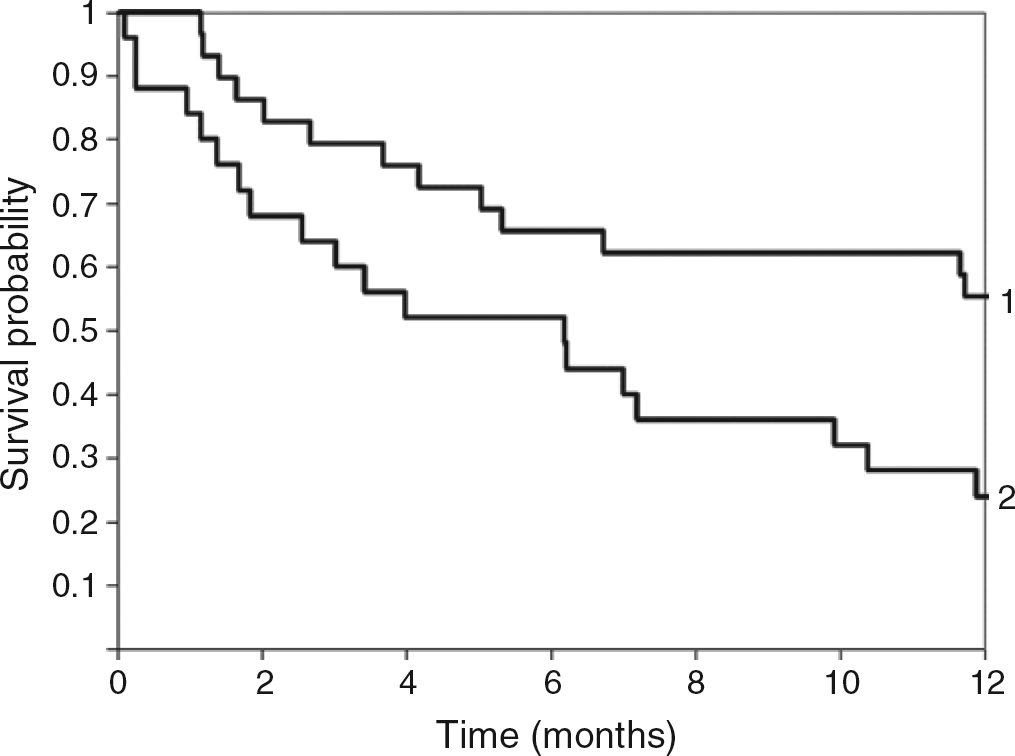
Receiver operator characteristic analysis for one-year mortality (area under curve [AUC] = 0.74) and fatty acid binding protein (FABP) (AUC = 0.76) versus Child-Pugh score (AUC = 0.59)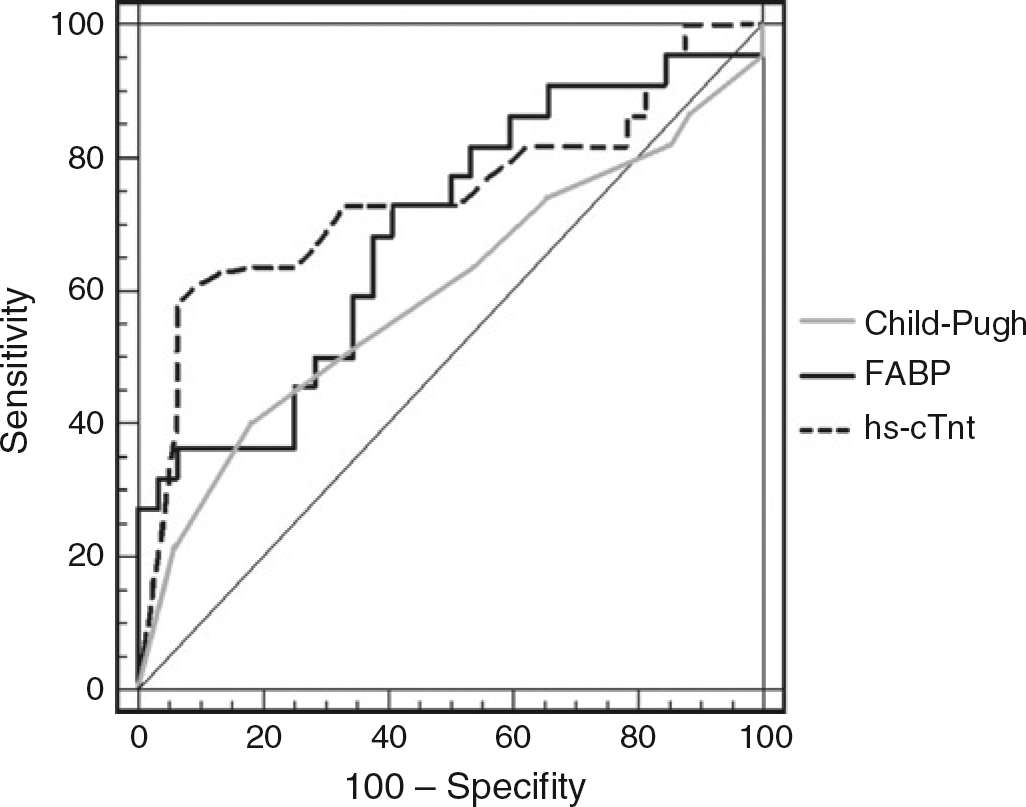
Univariable and multivariable Cox analysis including all factors noted to be significant on univariable analysis
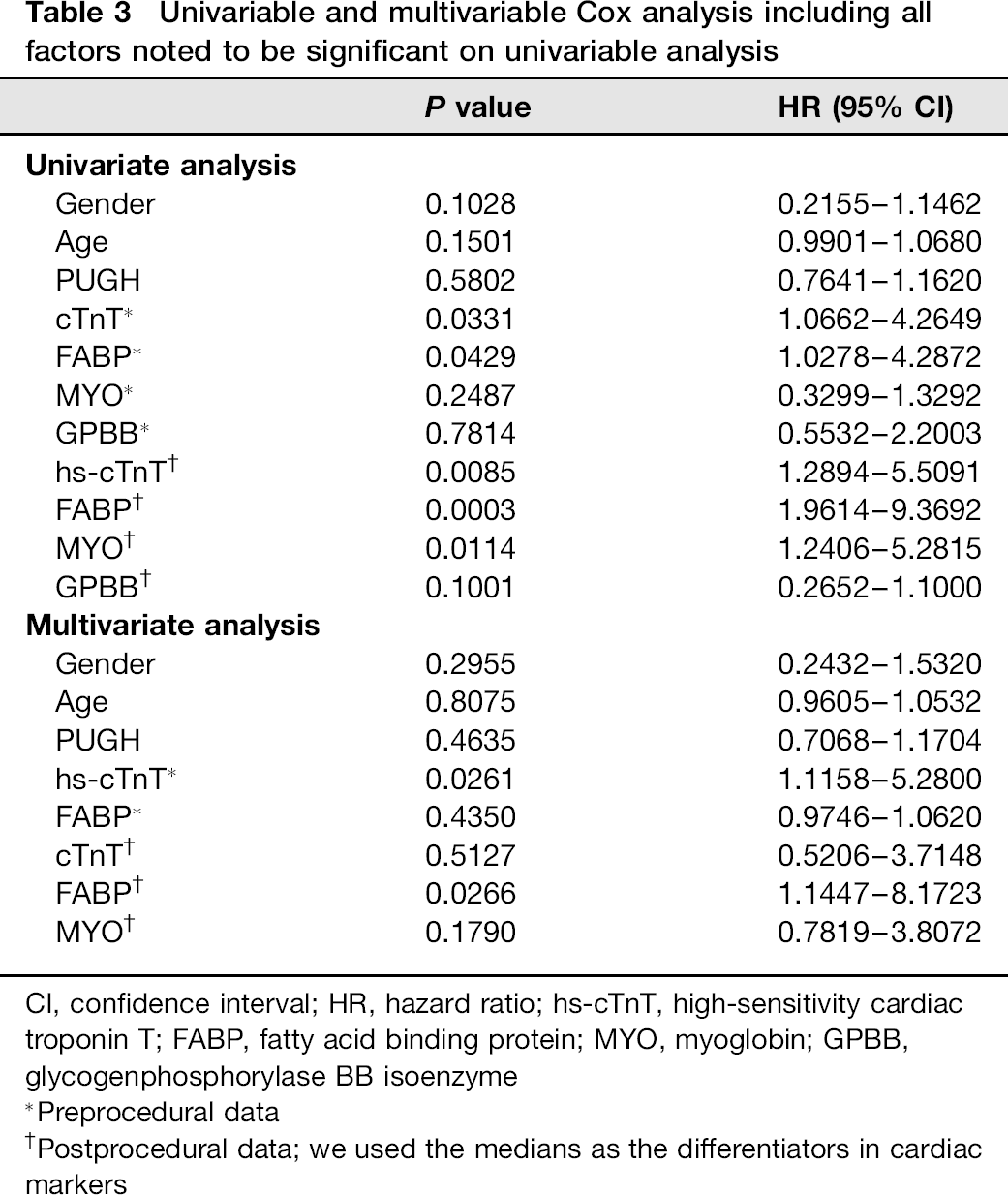
CI, confidence interval; HR, hazard ratio; hs-cTnT, high-sensitivity cardiac troponin T; FABP, fatty acid binding protein; MYO, myoglobin; GPBB, glycogenphosphorylase BB isoenzyme
Preprocedural data
Postprocedural data; we used the medians as the differentiators in cardiac markers
An association between postprocedural concentrations of cardiac markers (MYO, hs-cTnT, FABP, GPBB) and survival time was detected, with the following Spearman's correlation coefficients: FABP, r= -0.495 (P < 0.001); MYO, r= -0.404 (P = 0.004); hs-cTnT, r= -0.309 (P= 0.024); GPBB, r= -0.301 (P= 0.030). The rate of one-year mortality was significantly higher in patients with cardiac markers (MYO, hs-cTnT, FABP) above median (hs-cTnT: 0.013 μg/L; MYO: 18.61 μg/L; FABP: 2.62 μg/L) compared with lower concentrations. Results of the log-rank test were as follows: FABP, P < 0.001; hs-cTnT, P =0.006; MYO: P = 0.006.
The rates of one-year mortality in patients stratified by combination of medians (GPBB: 5.74 μg/L; MYO: 18.6 μg/L; hs-cTnT: 0.013 μg/L; FABP: 2.62 μg/L) are shown in Figure 4.
The one-year mortality stratified by combination of medians. 0-4 is number of cardiac markers with a concentration elevated above median (log-rank test P values: 0 versus 2, P = 0.003, 0 versus 3, P < 0.001, 0 versus 4, P< 0.001)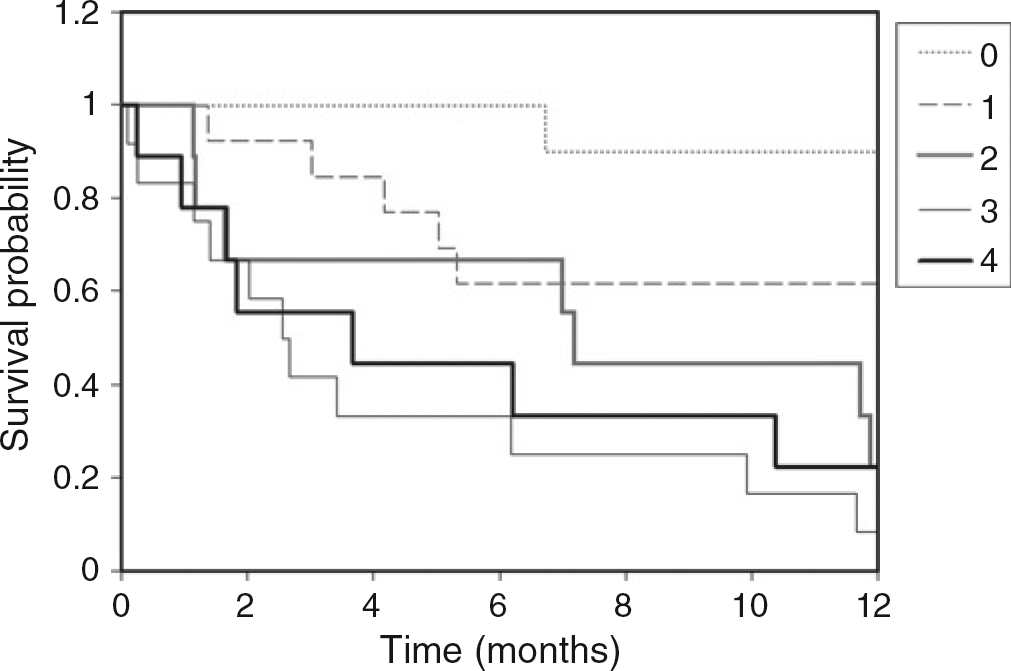
All cardiac markers that were significantly associated with risk in univariable analysis were then included in a Cox multivariable proportional hazards regression model which showed that preprocedural hs-cTnT and postproce-dural FABP concentrations remained statistically significant predictors of one-year mortality (Table 3).
Discussion
Liver cirrhosis is associated with significant changes in the cardiovascular system. It is accompanied by a hyperdynamic circulation due to increased plasma and blood volume, increased heart rate, cardiac output and a decrease in systemic vascular resistance. These changes in the cardiovascular system may be latent, but can be unmasked by physical and pharmacological strain. Due to its effects on cardiovascular haemodynamics, TIPS may unmask latent cirrhotic cardiomyopathy. Therefore, there is a need for risk stratification of patients considered for the TIPS procedure.
Measurement of biochemical markers of myocardial necrosis plays an important role in the diagnosis of acute coronary syndromes.16,17 A biochip-based assay is a novel method for rapid biochemical diagnosis of cardiac injury and risk stratification in patients with cardiovascular diseases. To our knowledge, this is the first report of a multi-analyte approach using a protein biochip assay for the measurement of cardiac markers for risk stratification of patients undergoing TIPS insertion. Relatively few studies have assessed the prognostic value of risk factors in patients with liver cirrhosis. Sersté et al. 18 reported that Child-Pugh score had a higher area under receiver operating curve for predicting mortality than MELD score (Model for End-stage Liver Disease, a scoring system using serum bilirubin, creatinine and INR).
We found a significant elevation in GPBB concentrations after TIPS. GPBB is a glycolytic enzyme that plays an essential role in the regulation of carbohydrate metabolism in the myocardium and is a very sensitive marker for the diagnosis of myocardial necrosis and ischaemia in patients with acute coronary syndromes. The BB isoenzyme is also the predominant isoenzyme of the human brain. Much lower GPBB concentrations have been reported in leukocytes, platelets, spleen, kidney, bladder, testis, digestive tract and aorta. When glycogen is broken down with the onset of tissue hypoxia, GPBB is converted from structurally bound form into a cytoplasmatic one and released from cardiomyocytes. 11 In our study there were no significant changes following TIPS in the concentrations of other cardiac markers (Table 2).
There was an association between the cardiac marker concentrations before and after TIPS insertion and one-year mortality. High preprocedural hs-cTnT and FABP concentrations and high postprocedural hs-cTnT, FABP, MYO and GPBB concentrations were associated with worse survival. Given the rise in GPBB postprocedure, it is perhaps unsurprising that the postprocedural GPBB should be associated with increased mortality. In contrast, however, although the MYO concentration did not increase post-TIPS, the post-TIPS concentration (but not the pre-TIPS concentration) was associated with worse survival. The postprocedural change in serum MYO concentration was minor and although not statistically significant (P = 0.09), may have impacted on the association of MYO concentration with survival. Differences between cardiac marker concentrations in relation to mortality may be explained by differing protein functions in the metabolism and physiology of the myocardium.
The preprocedural hs-cTnT concentration was a better mortality predictor than FABP, whereas of the postprocedural cardiac markers FABP was the best predictor. Both hs-cTnT and FABP performed better than Child-Pugh, a commonly used clinical measure of cirrhosis severity and prognosis.
Cardiac marker tests are cheap and relatively non-invasive. Measurement of cardiac markers may be useful for mortality prediction in cirrhotic patients after TIPS insertion. Serum FABP and hs-cTnT were better predictors of one-year mortality than the GPBB, MYO and the other conventional risk factors such as age, gender or Child-Pugh score.