
Abstract
Background
Measurement of fractionated plasma or urine metadrenalines is the recommended screening test in the diagnosis of phaeochromocytoma, with clinical cut-offs geared towards diagnostic sensitivity. Current practice at Salford Royal Hospital is to add urine catecholamines onto samples with raised urine metadrenalines, with the aim of adding specificity to a diagnosis of phaeochromocytoma.
Methods
This practice was reviewed by identifying a series of patients with raised urine metadrenalines who had catecholamines reflectively added. A total of 358 samples were identified from 242 patients, of which 228 had urine catecholamines measured.
Results
A diagnosis of ‘phaeochromocytoma‘ (n = 41) or ‘no phaeochromocytoma‘ (n = 90) was obtained in 131 of 228 patients, giving raised urine metadrenalines a positive predictive value for phaeochromocytoma of 31%. The finding of increased urine catecholamines in samples with raised urine metadrenalines increased specificity for phaeochromocytoma to 70%. However, 95% diagnostic specificity for phaeochromocytoma could be achieved by the introduction of a second cut-off for urine metadrenalines geared towards maximizing specificity.
Conclusions
Consideration of the degree of increase in urine metadrenalines is a superior method of determining the likelihood of phaeochromocytoma than measurement of urine catecholamines.
Introduction
Phaeochromocytoma may present with variable and nonspecific symptoms, making diagnosis dependent on biochemical demonstration of excess catecholamines or metadrenalines in urine or plasma. Metadrenalines have been widely reported as superior diagnostic markers of phaeochromocytoma, 1 due to their specificity as metabolites of adrenomedullary catecholamine metabolism. 2 Measurement of fractionated metadrenalines is the recommended first-line test in screening for phaeochromocytoma, with reference intervals designed to ensure maximal diagnostic sensitivity. 3 Though this approach avoids the potentially severe consequences of a missed diagnosis, distinguishing true-positive and false-positive results poses a problem. Current practice at Salford Royal Hospital is to reflectively measure catecholamines in 24-h urine samples with raised urine fractionated metadrenalines, with the aim of increasing the specificity of a diagnosis of phaeochromocytoma. The utility of this protocol was reviewed for a series of patients with raised urine metadrenalines.
Methods
A total of 358 samples with raised urine metadrenalines were identified from 1 January 2008–31 October 2010, derived via an in-house high-performance liquid chromatography (HPLC) 4 method (normetadrenaline reference ranges <4.3 μmol/24 h [women], <5.3 μmol/24 h [men], metadrenaline <2.0 μmol/24 h). These 358 samples related to 242 patients. Where patients had more than one sample with raised urine metadrenalines, the first specimen received was used. A total of 228 of 242 samples had urine free catecholamines measured reflectively, using a separate HPLC method (reference range noradrenaline <1.0 μmol/24 h, adrenaline <0.2 μmol/24 h). Reference ranges were previously defined in-house and were designed to provide maximal diagnostic sensitivity. All patients with urine metadrenalines below the reference range were presumed not to have phaeochromocytoma. Clinical outcomes in patients with increased urine metadrenalines were sought via case-note review or by contacting the referring laboratory.
Results
Follow-up data were obtained in 147/228 patients. Of these, 16 patients had an unclear diagnosis, were lost to follow-up or were being monitored for recurrence of phaeochromocytoma. A definite diagnosis of ‘phaeochromocytoma’ (n = 41) or ‘no phaeochromocytoma’ (n = 90) was obtained in 131/228 (57.5%) patients. A total of 115 patients had raised urine normetadrenaline and 41 patients had raised urine metadrenaline (25 patients had both increased urine normetadrenaline and metadrenaline).
Separate receiver operator characteristic curves were constructed for normetadrenaline/noradrenaline and metadre-naline/adrenaline to compare the diagnostic specificity of catecholamines and metadrenalines. Results are shown in Figure 1.
Receiver operator characteristic curves for normetadrenaline/ noradrenaline (a, n = 115) and metadrenaline/adrenaline (b, n = 41) in patients with raised urine normetadrenaline. (a) 1 = Noradrenaline 1 μmol/ 24 h, specificity 71%. 2 = Noradrenaline 1.73 μmol/24 h, specificity 95%. 3 = Normetadrenaline 14.0 μmol/24 h, specificity 95%. (b) 4 = Adrenaline 0.2 μmol/24 h, specificity 70%. 5 = Adrenaline 0.36 μmol/24 h, specificity 95%. 6 = Metadrenaline 5.4 μmol/24 h, specificity 95%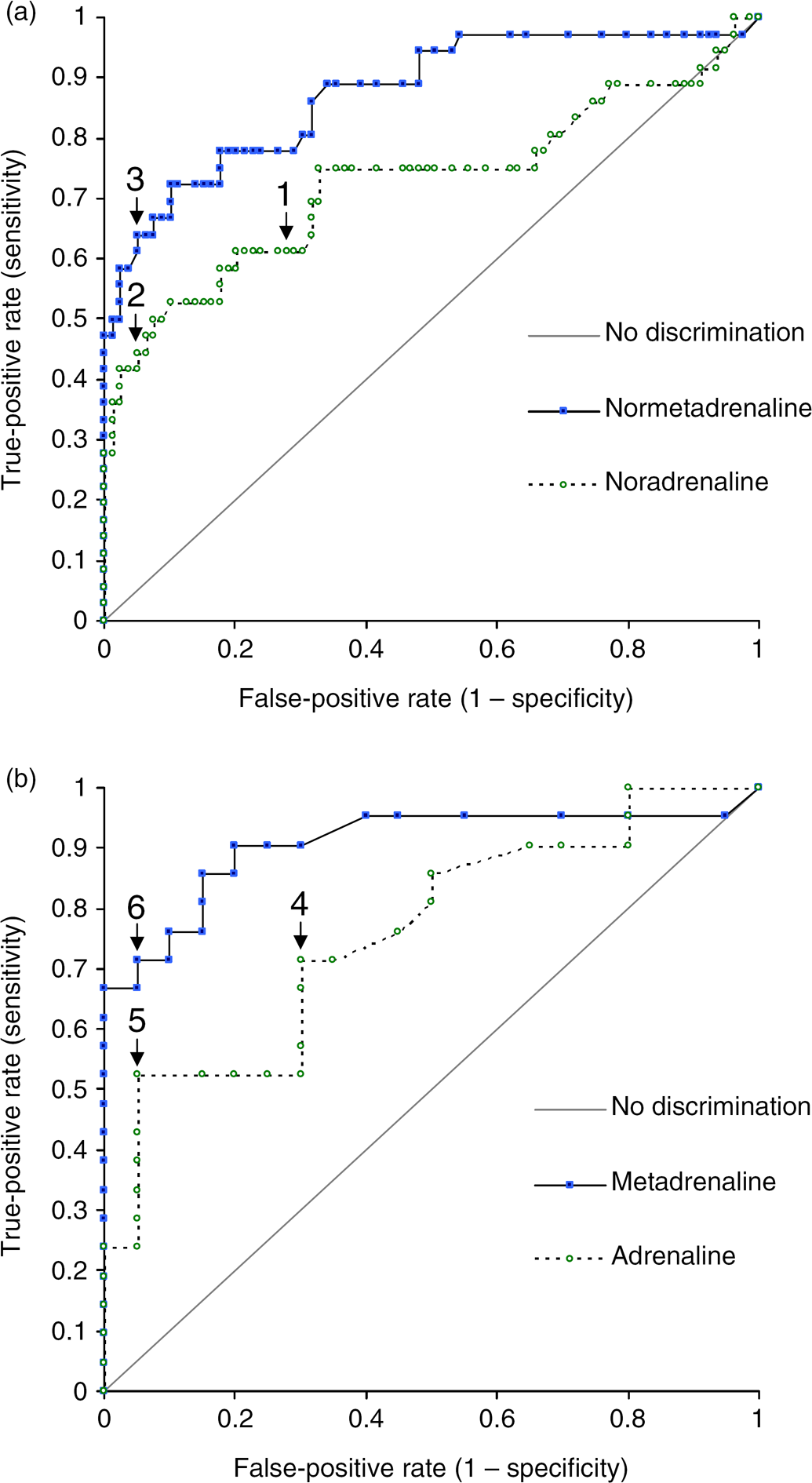
Of the 115 patients with raised urine normetadrenaline, 36 were found to have phaeochromocytoma, giving the test a positive predictive value (PPV) of 31.3%. The finding in addition of a raised urine noradrenaline (>1 μmol/24 h, 45 patients) increased specificity for phaeochromocytoma to 71% (PPV 49%). A urine noradrenaline value of 1.73 μmol/24 h (20 patients) provided 95% specificity for phaeochromocytoma (PPV 80%). For urine normetadrenaline, a value of 14.0 μmol/24 h (27 patients) provided 95% specificity for phaeochromocytoma (PPV 85%).
Of the 41 patients with raised urine metadrenaline, 21 were found to have phaeochromocytoma, giving the test a PPV of 51.2%. The finding in addition of a raised urine adrenaline (>0.2 μmol/24 h, 21 patients) increased specificity for phaeochromocytoma to 70% (PPV 71%). A urine adrenaline value of 0.34 μmol/24 h (12 patients) provided 95% specificity for phaeochromocytoma (PPV 92%). For urine metadrenaline, a value of 5.4 μmol/24 h (16 patients) provided 95% specificity for phaeochromocytoma (PPV 94%).
Discussion
Of the 131 patients with raised urine metadrenalines in whom a definite diagnosis was obtained, 41 were found to have phaeochromocytoma, giving the test a diagnostic specificity of only 31.3%. This emphasizes the need for a testing strategy that is able to distinguish true-positive from true-negative results. Lenders et al. 1 comprehensively demonstrated that measurement of metadrenalines in urine or plasma provided superior diagnostic sensitivity for phaeochromocytoma. However, they also detailed the superior diagnostic specificity of urine catecholamines in comparison to urine fractionated metadrenanlines (88% versus 69%). This small study sought to determine whether an approach of reflective catecholamine measurement in samples with raised urine metadrenalines increases specificity for phaeochromocytoma.
Although demonstration of increased urine catecholamines did increase the likelihood of phaeochomocytoma in this group, this study suggests that consideration of the degree of increase in urine metadrenalines is a more useful approach in determining the likelihood of phaeochromocytoma than the additional measurement of catecholamines, and that increased specificity for phaeochromocytoma could be attained simply by defining a second cut-off value for metadrenalines. A more simplistic interpretive approach may also be of benefit to clinicians unaware that metadrenalines are the internationally recommended first-line test of choice in the detection of phaeochromocytoma, 3 particularly as many UK-based laboratories appear to have been slow to adopt this recommendation and continue to use catecholamines as a first-line test. 5
Patients in whom urine metadrenalines exceed a 95% specificity cut-off (normetadrenaline 14 μmol/24 h, or metadrenaline 5.4 μmol/24 h) should be investigated promptly for phaeochromocytoma with imaging studies. Patients with raised urine metadrenalines, but with values below the cut-offs described above, may require further biochemical investigation via repeat measurement of metadrenalines in plasma or urine. This study demonstrates the importance of avoidance of utilizing a ‘binary approach’ in biochemical diagnosis of phaeochromocytoma, as has been highlighted elsewhere. 3
Conclusion
Reflective measurement of urine catecholamines on samples with raised urine metadrenalines is of little use and the practice should be discontinued. Instead, consideration of the degree of increase in urine metadrenalines provides superior diagnostic specificity in the diagnosis of phaeochromocytoma.
Declarations
Footnotes
Acknowledgements
The authors are grateful to the laboratories throughout the UK who kindly provided follow-up outcome data for their patients.