
Abstract
Background
Availability of whole blood creatinine estimation for patients scheduled to undergo radiological contrast investigations can provide information to aid patient care by reducing adverse effects and improving departmental efficiencies.
Methods
We performed imprecision studies, different patient sample type comparison in 40 participants, and a limited interference study with dopamine and dobutamine on the i-Stat and StatStrip point-of-care enzymatic analysers with the Beckman DxC800 Jaffe assay.
Results
Imprecision results showed that the i-Stat performed better. Patient comparison data indicated that the i-Stat provided better correlation than the StatStrip for all the different sample types with correlation coefficients (r2) being 0.995-0.996 and 0.918-0.995, respectively. The i-Stat results had a small positive bias of 6-9% for the three different sample types, which required different reference intervals. The StatStrip method showed greater scatter and overall small negative bias of 26% for the whole blood samples and a 10% positive bias with the plasma samples. Dopamine caused significant positive interference with the i-Stat only while dobutamine caused a small negative bias with the StatStrip method only.
Conclusions
The findings indicated there are differences offered by the two systems. The StatStrip requires a very small finger prick capillary sample, calculates estimation of the glomerular filtration rate and has an adjustment option to improve correlation with the local method. The i-Stat offers better analytical imprecision and patient comparison with the laboratory method with the three sample types but showed significant interference from dopamine. A final consideration was the availability of middleware to capture patient results with the i-Stat. Based on all the study data, the i-Stat was recommended.
Introduction
Blood plasma creatinine measurement and estimation of the glomerular filtration rate (eGFR) from the blood creatinine result using the modification of diet in renal disease equation are very useful parameters in preventing contrast-induced nephropathy (CIN). CIN is directly related to a number of pre-existing patient risk factors such as renal insufficiency (RI) with or without diabetes, advanced age, congestive heart failure, hypertension and dehydration. 1 CIN is the third leading cause of hospital-acquired renal failure and is associated with significant morbidity and mortality. 2 In a recent study, it was estimated that 5.3% of patients presenting requiring contrast studies did not have a recent creatinine/eGFR value. 3 It has also been pointed out that it is important to measure plasma creatinine 12–48 h post contrast infusion to check if CIN exists, as was found to be the case in 18% of patients in one study. 4 Furthermore, this study found that even after 30 d, 7% of patients had remained with renal damage. Undoubtedly, the incidence of CIN will be influenced by the level of RI.
Having access to point-of-care (POC) creatinine methods in Radiology Departments where such contrast compounds are administered allows for rapid estimation of both of these parameters to identify patients at risk of developing CIN and perhaps checking if CIN has developed post contrast infusion in order to implement appropriate treatments or management. The most commonly available and evaluated POC systems have been the Abbott i-Stat5,6 and the StatStrip.5,7–9
Less frequently, laboratories need to cross-check results from Jaffe methods with enzymatic methods that may not quite fit the clinical picture or are affected by compounds such as cephalosporins, 10 high bilirubin 11 and other non-creatinine compounds such as proteins, ketones and glucose, 12 albumin, IgG and haemoglobin F. 13 Enzymatic methods are based on different cascades of enzyme reactions. The end product for the i-Stat and the StatStrip is peroxidase that eventually generates a current to determine the concentration of creatinine. These enzymatic methods have been shown to be affected by compounds such as dopamine 14 and acetominophen at above therapeutic concentrations. 9
There have been several evaluations of both the i-Stat5,6 and StatStrip5,7–9 creatinine methods and they have mainly used leftover whole blood samples or plasma and compared with plasma samples.
In our tertiary level hospital, contrast compounds are commonly administered for diagnostic purposes. The primary aim of this study was to recommend for the Radiology Department, a POC system to enable the rapid estimation of these two parameters (creatinine and eGFR) in order to identify patients at risk and expedite the patient throughput. A secondary aim was to determine the effects of different sample types on the accuracy and precision of results with these POC methods.
Materials and methods
Creatinine methods
The comparative or reference creatinine method was the Beckman DxC800 Jaffe method (Beckman Coulter Diagnostics, Brea, CA, USA) using lithium heparin plasma samples, which has been shown to closely correlate with a high-performance liquid chromatography method. 11 This method is also calibrated using a standard directly traceable to the isotope dilution mass spectrometry method. Both POC methods, i-Stat (Abbott Diagnostics, East Windsor, NJ, USA) and StatStrip (Nova Biomedical, Waltham, MA, USA), are enzymatic.
Imprecision
Imprecision studies (consecutive and between-day) were carried out using manufacturer-specific quality controls, levels 1 and 3. The results are shown in Table 1. The analysers were checked using two levels of control materials prior to any participant blood sampling, as part of the between-day imprecision protocol. The Royal College of Australasia External Quality Assurance Program (RCPA EQAP) limits of <8 μmol/L when the plasma creatinine value is ≤100 μmol/L and <8% when the value is >100 μmol/L were used as a guide to determine if imprecision was acceptable.
Creatinine precision data for the StatStrip and i-Stat analysers using their respective quality control materials
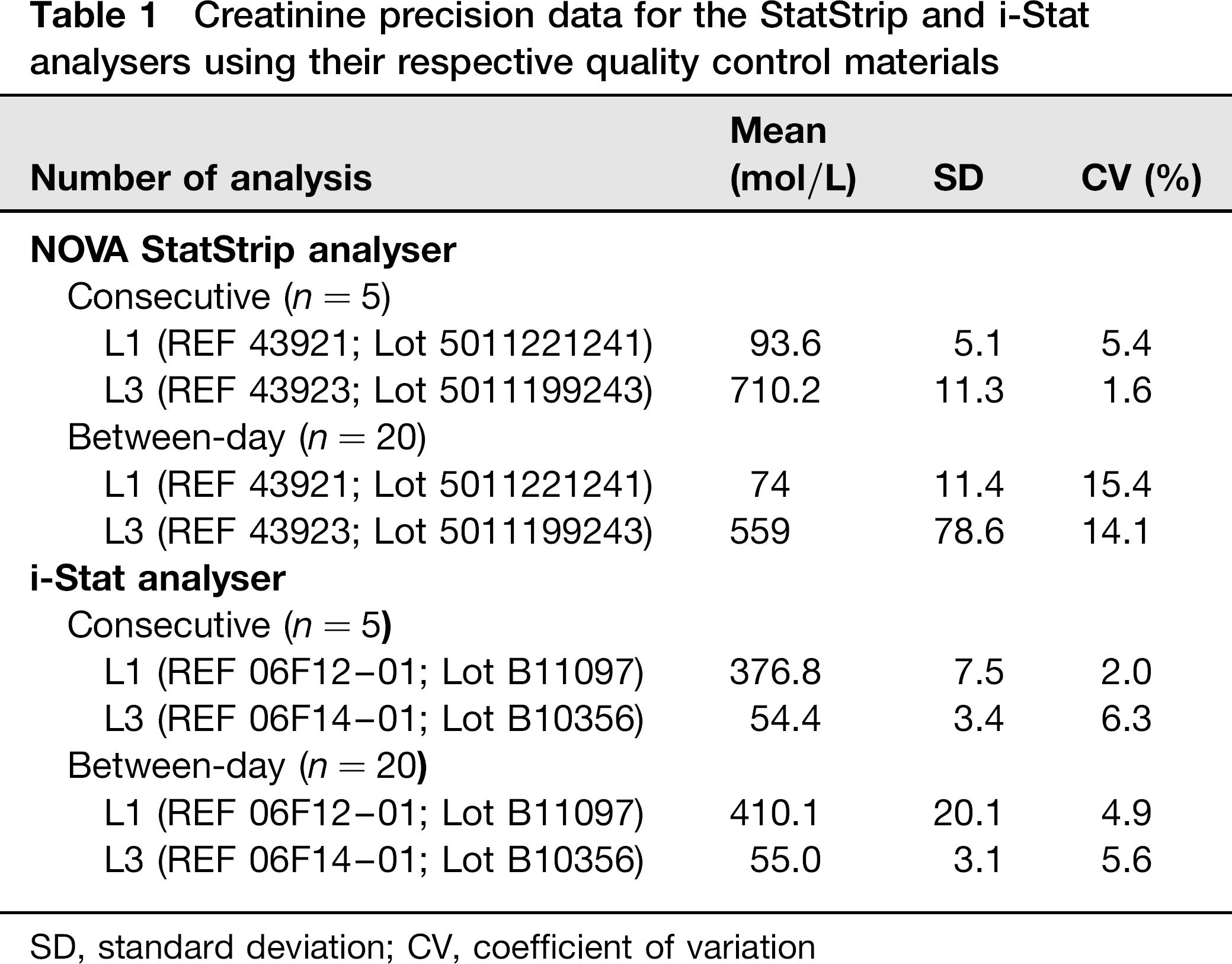
SD, standard deviation; CV, coefficient of variation
Samples
Blood samples were collected with consent, as approved by Princess Alexandra Hospital Ethics Committee, from 40 participants all >18y of age, consisting of healthy laboratory staff and renal outpatients. The venous samples were collected by an experienced phlebotomist into blood gas syringes (Blood Gas Syringes, REF: 4648PE; Smiths Medical, St Paul, MN, USA) and Greiner Vacuette lithium heparin tubes (Cat no. 456083; Greiner Bio-One, Kremsmuster, Austria). The tubes were processed as per the manufacturer's recommendations. Whole blood in the Greiner tubes was analysed on both the StatStrip and i-Stat analysers and then the tubes were immediately centrifuged for 10 min at 3000 g, 20°C. The plasma samples from the Greiner lithium heparin tubes were analysed within ∼60 min of the two POC analysers by the comparative method on a Beckman DxC800 general chemistry analyser using a Jaffe method (Beckman Coulter Diagnostics). The capillary samples were collected by either of two different experienced laboratory staff (VT and BWJ). The finger collection site of each participant was cleaned with an alcohol wipe, and allowed to thoroughly dry before piercing with a spring-loaded sterile lancet. There was minimal squeezing or milking of the selected finger. The blood was applied directly onto the StatStrip. Attempts were also made to collect capillary blood into a capillary collection device (Capillary Tubes, REF 10325868; Siemens, Munich, Germany) for i-Stat analysis. The different whole blood sample types were analysed in random order on the two analysers followed by the plasma. For the StatStrip, all analyses were performed using a single strip lot number (Creat Test Strips, REF 43272; Lot 4911013249) and for the i-Stat two different lot numbers were used (Creat cartridge, REF 06F10-01; Lot U11190 and U11208). Two different limits were used to determine if performance was acceptable. The first was based on Clinical Laboratory Improvement Amendments total allowable error between the test sample creatinine and creatinine measured by the comparative method of >27 μmol/L. The second was based on the commonly accepted diagnostic criteria for CIN looking for a change in baseline creatinine of >44 μmol/L or >25%. 15,16 Both serum creatinine results of >180 μmol/L and eGFR <45 mL/min have been used to screen patients at risk of CIN prior to administration of contrast agents. 15 , 17
Interference
Dopamine and dobutamine have been demonstrated to interfere with peroxidase chromophore assays, including enzymatic creatinine assays. 18 The i-Stat has been shown to be positively interfered by dopamine, 14 yet in our searches there appear to be no data on the StatStrip analyser.
A normal serum pool was prepared and aliquoted. Aliquots were spiked with different concentrations of dopamine (Dopamine 200 mg/5 mL; Hospira, Melbourne, Australia) and dobutamine (Dobutamine 250 mg/20 mL; Sandoz, Sydney, Australia). For both compounds, the three spiked sample solutions prepared had final concentrations of 40, 80 and 200 mg/L. A greater than 27 μmol/L difference between baseline creatinine and creatinine measured in the presence of interferent was considered clinically significant. The results are shown in Table 2.
Interference study with dopamine and dobutamine
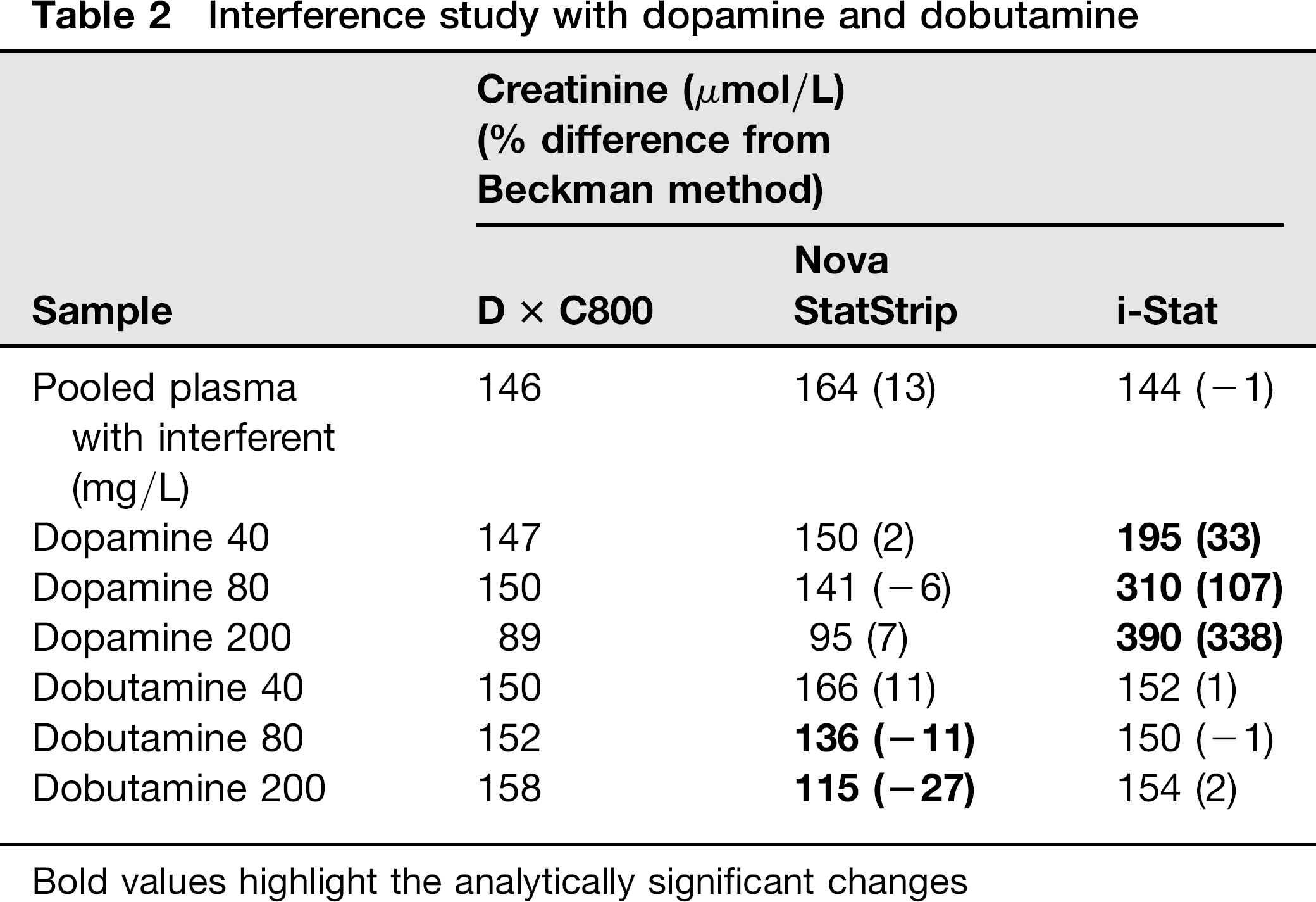
Bold values highlight the analytically significant changes
Statistics
Sample comparison studies were performed using Analyse-it software (Analyse-it Software, Leeds, UK) to calculate the Passing–Bablok regression data and obtain the difference plots, and Microsoft Excel version 2003 (Microsoft, Redmond, WA, USA) for the remaining data analysis.
Results
Precision
Please see Table 1.
Patient comparison
The concentration range of the samples tested by the Beckman method was 43–693 μmol/L. One result was not obtained with the capillary sample on the StatStrip method due to sample flow error. All of the samples with eGFR <30 L/min were from renal-impaired patients. The patients’ correlation data are shown in Table 3 and Figure 1. The effect of the higher creatinine results with the i-Stat analyser on the estimated eGFR for both women and men at two different ages and at two different creatinine levels is shown in Table 4.
Bias plots. Creatinine difference plots and the Passing–Bablok regression data with the StatStrip and i-Stat analysers using different sample types. (Only eight capillary samples were able to be collected into the capillary tubes for the i-Stat, data insufficient for meaningful calculations.) (a) Lithium heparin whole blood StatStrip; (b) blood gas syringe whole blood StatStrip; (c) capillary (finger prick) StatStrip; (d) lithium heparin plasma StatStrip; (e) lithium heparin whole blood i-Stat; (f) blood gas syringe whole blood i-Stat; (g) lithium heparin plasma i-Stat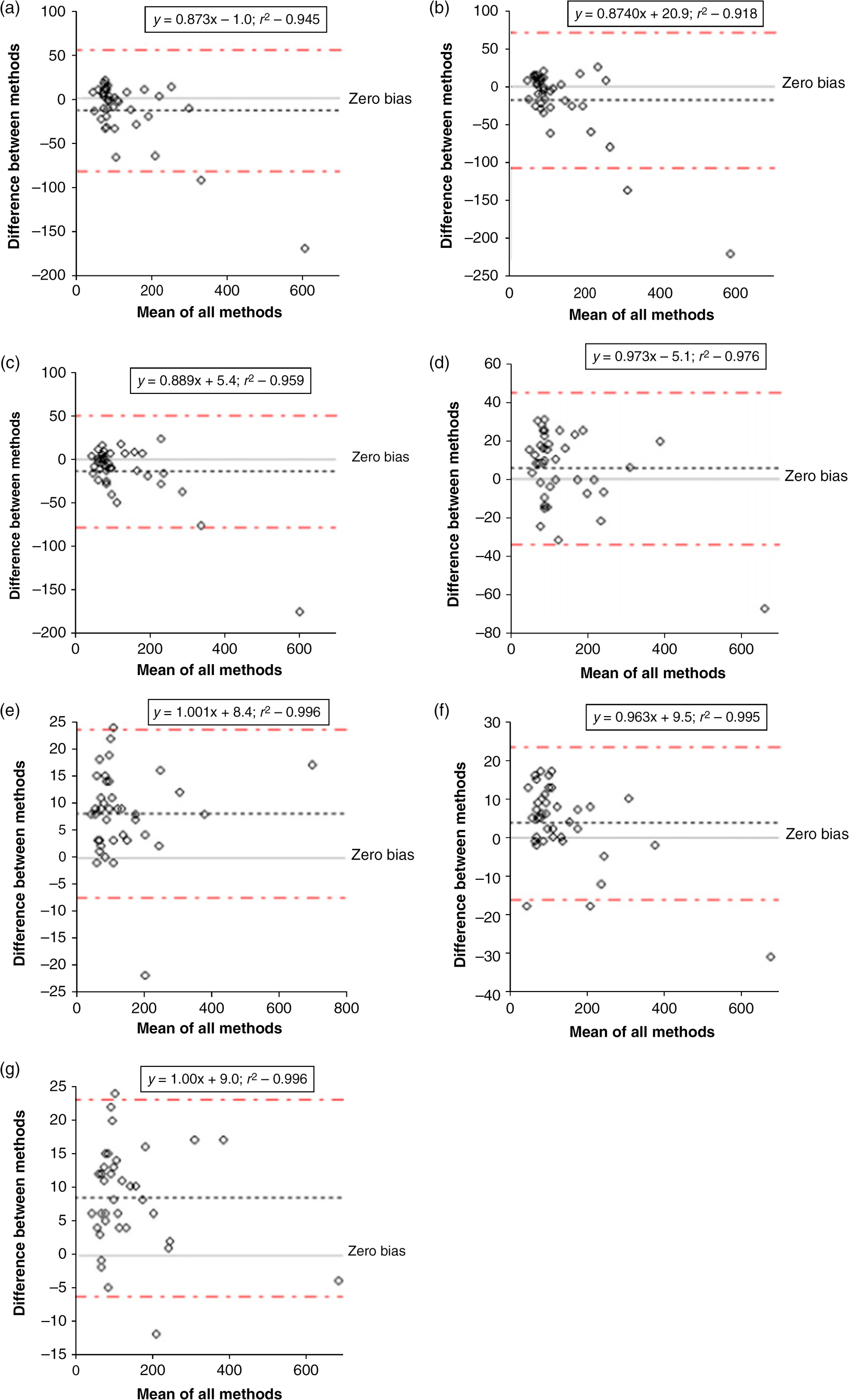
The number of creatinine results exceeding the 27 and 44 μmol/L acceptability limits
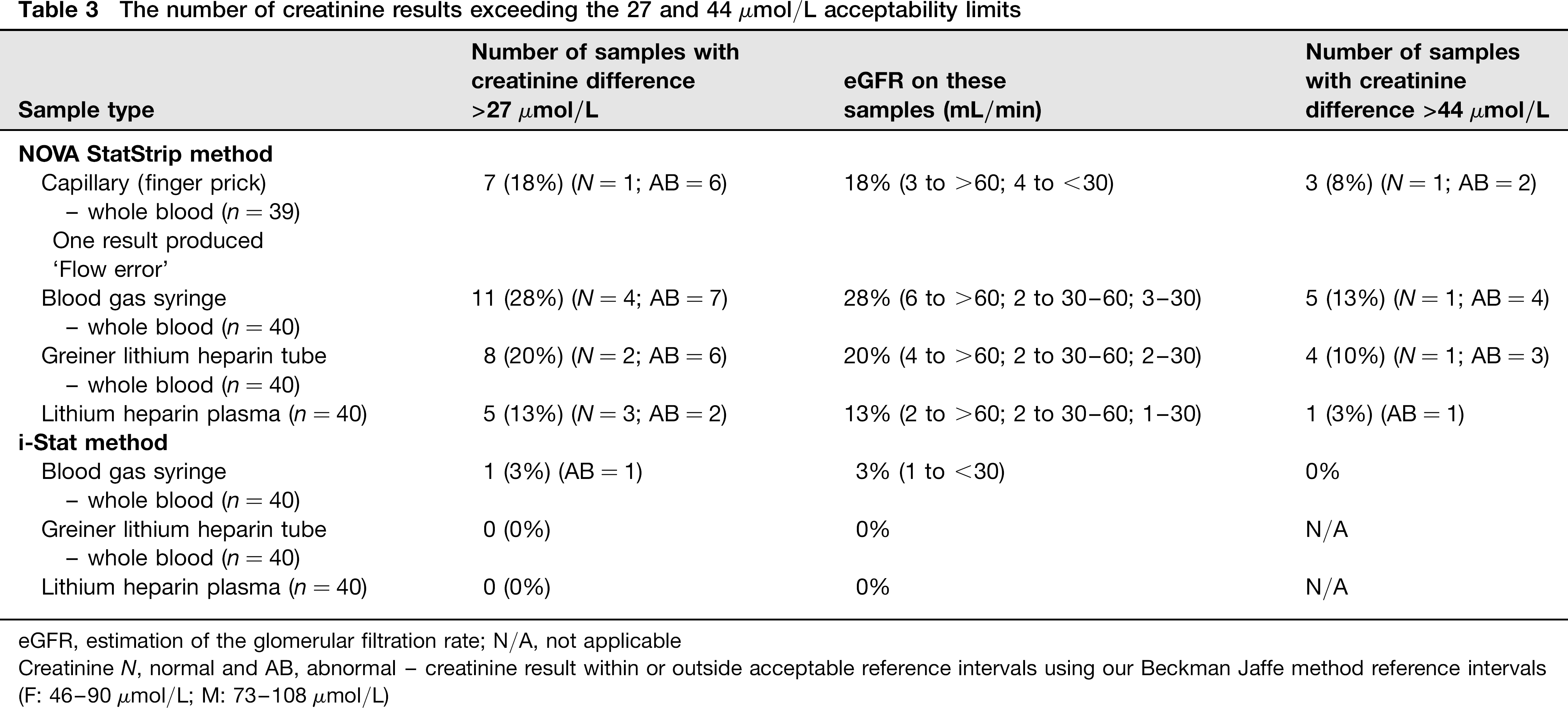
eGFR, estimation of the glomerular filtration rate; N/A, not applicable
Creatinine N, normal and AB, abnormal – creatinine result within or outside acceptable reference intervals using our Beckman Jaffe method reference intervals
(F: 46-90 μmol/L; M: 73-108 mmol/L)
Expected eGFR estimations based on the ∼6% increase in creatinine results with the i-Stat analyser with two age groups for both women and men at two different creatinine concentration levels
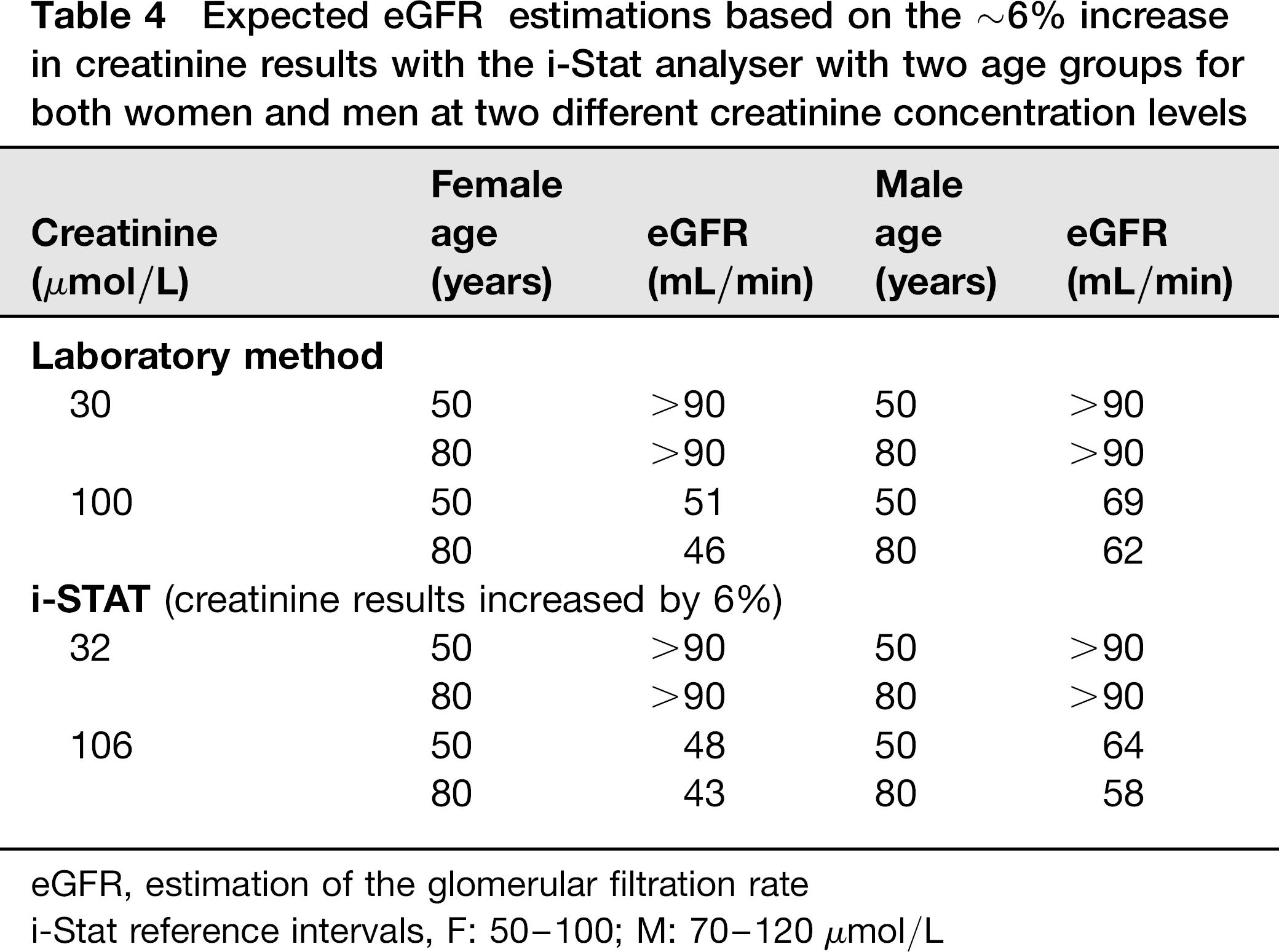
eGFR, estimation of the glomerular filtration rate
i-Stat reference intervals, F: 50–100; M: 70–120 μmol/L
Interference
Please see Table 2.
Discussion
This evaluation study showed that only imprecision data outside the desirable limits was the StatStrip between-run.
The patient comparison study demonstrated the i-Stat analyser creatinine and eGFR results to have superior correlation compared with the StatStrip with the laboratory Jaffe method with all three sample types. Like other studies,5,9 the results in this study for POC creatinine were slightly higher (6% for the sample of choice, blood gas syringe) than the comparative laboratory plasma methods. The study by Lee-Lewandrowski et al. 3 showed that the i-Stat results were slightly lower for values greater than 177 μmol/L, which suggests that this difference is method-dependent. It was decided to provide separate reference intervals (F: 50–100; M: 70–120 μmol/L) for the i-Stat method which may lead to some samples’ eGFR calculations being lower by ∼6% and patients may be potentially misclassified.
The findings in our study are in line with a recent study which found that using the StatStrip plasma rather than whole blood provided closer correlation with the comparative laboratory method. 7 Analysis of those results exceeding the 27 μmol/L difference indicated that the StatStrip results were mostly in patients’ samples with results above the laboratory creatinine reference intervals for the Beckman Jaffe method. These results (Table 3) clearly indicated that the sample type influenced the StatStrip method far more than the i-Stat method, which suggests that there are other sample factors influencing the accuracy.
The interference study demonstrated very significant positive interference from dopamine with the i-Stat method but no interference was observed with the StatStrip method. Dobutamine had no significant effect on the i-Stat method but had negative bias on the StatStrip method and this bias increased with rise in the dobutamine concentration. Such high concentrations of these compounds would only be encountered on very rare occasions or due to contamination of the sample if collected from the infusion line. Our results are in line with the findings by Saenger et al. 14 What is unknown is if metabolites of these drugs are capable of causing interference. As Panteghini 12 points out, although enzymatic methods are said to be more accurate, they are not free from interferences. Having the two creatinine methods (Jaffe and enzymatic) now in routine use affords the laboratory an easy option to crosscheck clinically suspect results.
Some of the other differences between the two systems are: the StatStrip requires very small sample volume (1.2 μ) which is much more convenient as finger prick capillary collection and results are available in 30 s. The i-Stat requires 2-3 drops and takes >120 s and we were only successful in obtaining sufficient finger prick blood in eight participants. Unlike the StatStrip analyser, the i-Stat does not provide software capability to automatically calculate the eGFR. The StatStrip affords an ability to enter a slope and intercept offset to match local laboratory plasma methods. This, however, may have an opposite effect; it may improve comparison with the laboratory plasma method for some results but deteriorate comparison for others. 8 One final point for consideration was connectivity, availability of middleware software to directly transfer patient results in the laboratory information system patient files. This was available for the i-Stat only. This transfer does not occur in realtime; thus to overcome this shortfall and provide immediate eGFR estimates, the Radiology Department computers were set up with links to the Kidney Australia website 19 for the rapid calculation of the eGFR.
There is one published study where the i-Stat analysers were implemented in a Radiology Department: the laboratory had trained radiology technicians performing the analysis. To us it was evident that nurses were the most appropriate staff to perform the sample analysis as they were the ones who cannulize the patients. Samples for creatinine analysis are collected and performed immediately after the cannula is inserted and blood collected into a blood gas syringe, before any fluids are infused. Each nurse underwent hands-on and electronic training/competency and password lockout before being provided with access to use the analyser for sample analysis. Currently, the Radiology Department performs 3-10 samples per day. The laboratory maintains and provides support (ordering of consumables, maintenance and trouble shooting, internal and external quality checks, etc.) to maximize quality of service. This ensures that the highest efficiency is realized with clinical and operational resources. With cardiac patients commonly undergoing contrast procedures, these same patients are also frequently on dopamine, thus interference with the i-Stat estimated creatinine is a real possibility. Therefore, it has been clearly highlighted to the Radiology Department nursing staff that unexpectedly high creatinine results may be false and must be immediately re-checked in the laboratory by the Jaffe method. Another patient group of interest is Parkinson's disease where methyldopa is commonly prescribed. Methyldopa is converted to dopamine and may cause false high creatinine results with the i-Stat method.
With the incidence of hypertension and diabetes mellitus increasingly linked with an aging population and changes in lifestyle, the incidence of renal dysfunction among the general population follows the same trend. Hence, the number of patients requiring contrast investigations will no doubt follow the upward pattern. One report states the occurrence of CIN to be 0.5% among people with normal renal function, 5% among people with moderate RI and 50% among people with serious RI. 10 In patients admitted with acute kidney injury, contrast media was responsible for or contributory in 11-15.5% of cases. 17 However, Katzberg and Newhouse indicated that this is an over-estimation with more modern procedures. 15 Either way, this suggests radiology and other clinical units infusing contrast compounds should follow up patients and measure creatinine and eGFR pre and ∼2-5 days post contrast procedure. This has implications for both patients and clinical units. Shiragami et al. 20 point out that CIN typically presents with an acute rise ∼24 h after contrast, peaking at 3-5 d and returning to baseline by 7-10 d. Contrast infusion is usually not performed if the eGFR is <30 mL/min. However, there are times when clinical need for information necessitates contrast infusion in patients with a low eGFR. In such instances, the dose of contrast is minimised and the patient is well hydrated in order to reduce the risk of CIN.
Although most of the time CIN reflects mild transient impairment of renal function, a small proportion of patients who develop CIN have an increased risk of potentially serious complications such as cardiovascular events and mortality. The mortality rate in cases of CIN has been reported by one publication to be 14%. 21 These publications indicate that patient follow-up is to be seriously considered to identify patients who may have developed both transient and long-term CIN. At this stage, our hospital does not proactively monitor outpatients or inpatients to see if CIN has been developed post contrast infusion; equally, literature is also scarce on recommendation of follow-up. Furthermore, it may even be useful to have outpatients pretested days in advance rather than just before the procedure to determine if it is safe to proceed rather than disappoint patients at the last minute and cause inconveniences such as re-scheduling the procedure and create inefficiencies in workflow in Radiology Departments.
In summary, the findings from this study indicated that there are various differences offered by the two systems. The StatStrip offers a simplified testing process with a very small finger prick capillary sample, calculates eGFR and has an adjustment option to improve correlation with the local method. However, the StatStrip exhibits poorer precision. In contrast, the i-Stat offers better analytical imprecision and patient comparison with the laboratory method across the different sample types. However, the i-Stat showed significant interference from dopamine. A final consideration in our decision was the availability of middleware to capture patient results and store in the laboratory information system. Based on all the data from the study and the availability of middleware, the i-Stat analyser was recommended.
Declarations
Footnotes
Acknowledgements:
Sincere thanks to our phlebotomy staff for their assistance with the specimen collections.