
Abstract
We report two patients with markedly elevated 24-h urine 5-hydroxyindoleacetic acid (5-HIAA) excretion due to over-the-counter (OTC) self-medication with 5-hydroxytryptophan (5-HTP). It is important to recognize that OTC medication may cause increased ‘false-positive‘ 5-HIAA excretion to prevent undue patient anxiety and unnecessary further investigation for carcinoid disease. Discordance between chromogranin A and 24-h urine 5-HIAA results should alert to the possibility of false-positive or -negative laboratory results.
Introduction
Elevated 24-h urine 5-hydroxyindoleacetic acid (5-HIAA) excretion is a marker of carcinoid syndrome.1–3 Flushing often occurs, though not usually in isolation, in carcinoid syndrome, and therefore 24-h urine 5-HIAA is often requested in the investigation of flushing.3,4 Mild elevation in 24-h urine 5-HIAA excretion is well described for tryptophan-rich foods and certain medications.1,3,5–8 We report two cases of markedly elevated 24-h urine 5-HIAA excretion due to over-the-counter (OTC) self-medication with 5-hydroxytryptophan (5-HTP) only uncovered by specifically asking about OTC self-medication.
Case Reports
Case 1
A 61-year-old woman was referred by her general practitioner to the general medical outpatients department with a recent history of facial flushing associated with sweats, tiredness and difficulty sleeping. These symptoms coincided with her being made redundant. Her past medical history included primary hypothyroidism and severe osteoarthritis. She was on thyroxine and fentanyl patches. Apart from obesity (body mass index 44.9 kg/m2), a clinical examination was unremarkable. Investigations revealed a markedly raised 24-h urine 5-HIAA excretion of 290 μmol (reference interval 0–50) raising the possibility of carcinoid syndrome. A subsequent chest X-ray and computed tomography scan of the abdomen and pelvis showed no abnormality; in particular, no evidence of carcinoid disease. A repeat 24-h urine 5-HIAA excretion, after reinforcing appropriate advice regarding avoidance of foods and medicines that may increase 5-HIAA excretion, remained elevated at 323 μmol but serum chromogranin A (CgA) was normal at 5 nmol/L (reference interval 0–6). The discordance in these results suggested the possibility of interference in either the 5-HIAA or CgA assay. On review in the metabolic clinic, when specifically asked about OTC medication, she stated that she was taking Happy Days (equivalent to 100 mg 5-HTP per day) and melatonin supplements for difficulty sleeping. Repeat 24-h urine 5-HIAA excretion, four weeks after stopping OTC preparations, was normal at 17 μmol. Other investigations including serum thyroid function tests (on thyroxine replacement), serum calcitonin, plasma glucose, routine biochemistry and haematology, and inflammatory markers were normal.
Case 2
A 68-year-old woman was referred by her general practitioner to the endocrinology outpatients department with an eight-year history of isolated generalized flushing. Her past medical history included hypertension and a hysterectomy for uterovaginal prolapse at the age of 45 y following which she received oestrogen replacement therapy for 15 y. She was taking ramipril. A clinical examination was unremarkable. Investigations, however, revealed a raised 24-h urine 5-HIAA excretion of 198 μmol after appropriate advice regarding avoidance of foods and medicines that may increase 5-HIAA excretion. Other investigations including 24-h urinary free catecholamines, serum thyroid function tests, serum calcitonin, plasma glucose, routine biochemistry and haematology, and inflammatory markers were normal. On review, when specifically asked about OTC medication, she stated that she was taking Sweet Dreams (equivalent to 100 mg of 5-HTP per day) to help her sleep. Repeat 24-h urine 5-HIAA, four weeks after stopping Sweet Dreams, was normal at 10 μmol, as was serum CgA.
Discussion
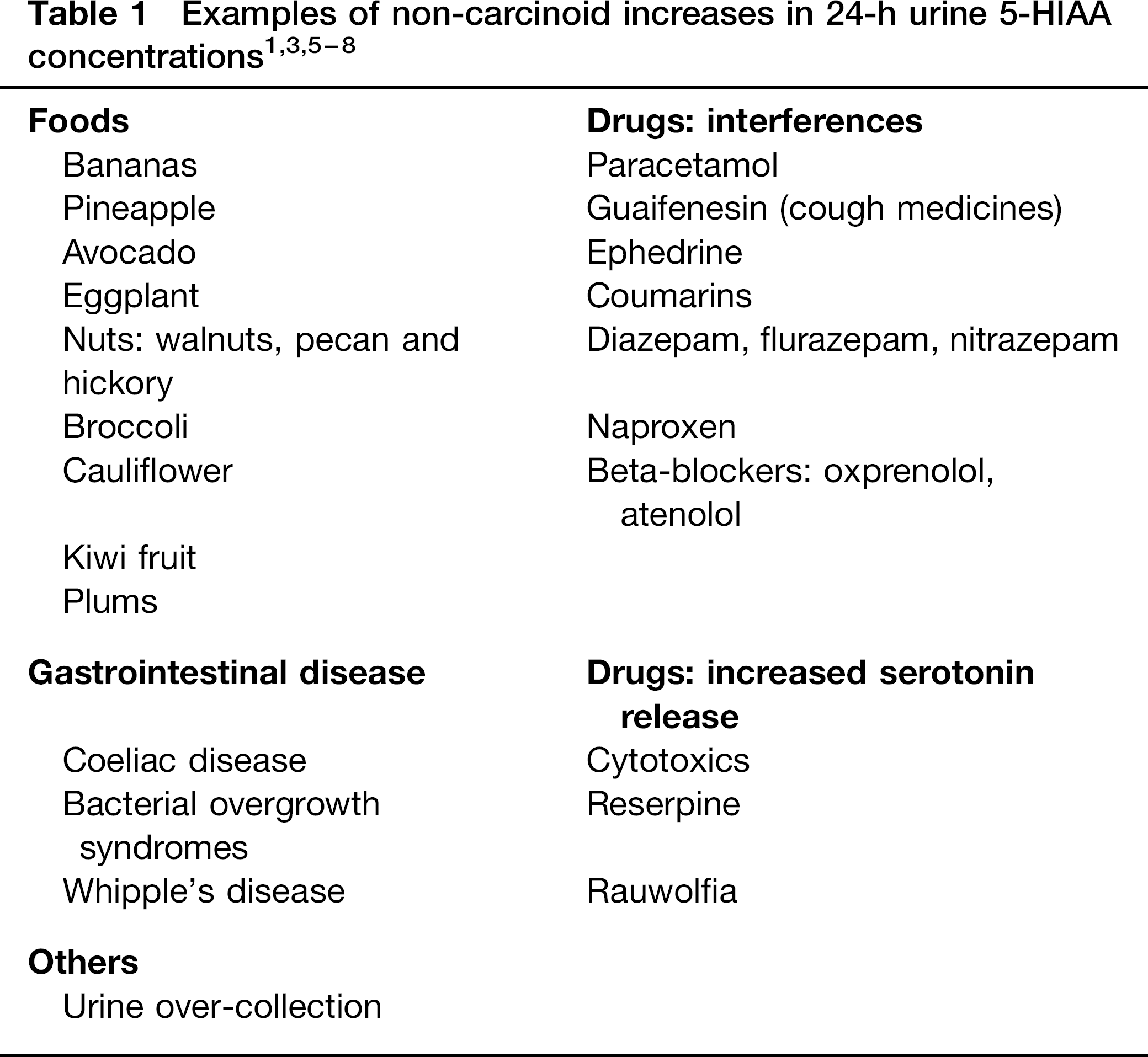
Biochemical confirmation of carcinoid syndrome includes elevated 24-h urine 5-HIAA (a metabolite of serotonin) excretion and raised plasma chromogranins. Markedly elevated 24-h urine 5-HIAA excretion, as in the reported cases, is almost always associated with carcinoid syndrome. In selected populations, the reported sensitivity of 24-h urine 5-HIAA is 35–73% while its specificity is 100% for carcinoid disease.9,10 Minor elevation in 24-h urine 5-HIAA excretion may occur with drugs, non-carcinoid gastrointestinal disease and tryptophan-rich foods (Table 1).1,3,5–7 CgA, a general neuroendocrine tumour marker, is considered the best marker for detecting carcinoid tumours and for monitoring disease activity. In selected populations, elevated CgA has a specificity of 96–84% and a sensitivity of 55–85% depending on cut-off values.9,11 Inflammatory conditions, renal insufficiency, achlorhydric gastritis and treatment with proton pump inhibitors may raise CgA concentrations. 12
5-HTP is an intermediary metabolite in the biosynthesis of serotonin from the essential amino acid L-tryptophan. Usually, 1–3% of dietary tryptophan is metabolized to serotonin. 5-HTP is not normally present in the diet and dietary supplements are commercially extracted from the seeds of the African plant, Griffonia simplicifoli. Unlike L-tryptophan, 5-HTP is only metabolized to serotonin and cannot be shunted into niacin or protein production. Since oral supplements of 5-HTP increase brain serotonin metabolism,13,14 it has been used in conditions that may be associated with decreased brain serotonin concentrations including depression, insomnia as well as disorders of mood, anxiety and appetite, but evidence for clinical effectiveness remains controversial.15,16 5-HTP is also promoted for a wide variety of ailments, including flushing, without an evidence base for efficacy. In our patients, the introduction and stopping of 5-HTP supplements had no effect on their flushing.
The importance of 5-HTP supplementation is recognition that it increases 24-h urine 5-HIAA excretion indicating carcinoid syndrome,17,18 and if unrecognized may lead to a misdiagnosis of carcinoid disease, particularly in ‘symptomatic’ patients. 18 As 5-HTP is not a prescribed drug, patients may not report their use and should be specifically asked about OTC medication and herbal remedies. If unrecognized, this may lead to inappropriate and unnecessary investigation and undue patient anxiety as illustrated in these case reports. In case 1, the discordance in serum CgA and urine 5-HIAA results alerted us to the possibility of a false-positive result for carcinoid syndrome, whereas in case 2, 5-HTP ingestion was specifically elicited as the index of suspicion for carcinoid disease was low.
In summary, we report two patients with markedly elevated 24-h urine 5-HIAA excretion due to 5-HTP self-medication. We suggest that elevated 24-h urine 5-HIAA in patients with a low index of clinical suspicion for carcinoid disease should prompt specific enquiries about OTC medication and herbal remedies to avoid undue patient anxiety and unnecessary investigation. Discordance between CgA and 24-h urine 5-HIAA results should alert to the possibility of an exogeneous source for raised 24-h urine 5-HIAA concentrations.