
Abstract
Hereditary renal hypouricaemia (HRH) is a genetic disorder commonly associated with exercise-induced acute kidney injury (AKI). We report the case of a 19-year-old man who was admitted to hospital with exercise-induced AKI and who was subsequently shown to have HRH. We believe this to be the first description of a case of HRH co-presenting with rhabdomyolysis.
Case report
A 19-year-old man was admitted to hospital with a history of dysuria, recurrent vomiting, severe muscle pain and weakness. Two days previously he had undertaken a session of rigorous exercise for the first time in the local gymnasium. His urine was slightly dark in colour. He had no history of illegal drug abuse, alcohol consumption, trauma, recent illness or any previous episode of a similar nature. There was no known family history of muscular or metabolic disease.
On admission his vital signs were as follows: heart rate 96/min, temperature 37.1℃, respiratory rate 20/min and blood pressure 130/80 mmHg. On examination there was muscular tenderness particularly in the calf muscles. There was no evidence of oedema or skin rash in the extremities. Power was 5/5 in both lower and upper limbs. The remaining physical examination was unremarkable. Laboratory investigations showed serum creatinine 736 μmol/L (reference interval 53–106 μmol/L), urea 16.7 mmol/L (reference interval 2.5–7.5 mmol/L), sodium 138 mmol/L (reference interval 135–145 mmol/L), potassium 6.2 mmol/L (reference interval 3.5–5.0 mmol/L), uric acid 243 μmol/L (reference interval 208–416 μmol/L) and creatinine kinase 10,127 U/L (reference interval 10–190 U/L). Serum C-reactive protein concentration and full blood count were within normal reference intervals. Further investigation revealed mildly increased serum alanine and aspartate aminotransferase activities. Routine urinalysis revealed protein of 1+ with 10–12 red blood cells per high power field. Abdominal ultrasound scan was normal. A diagnosis of exercise-induced rhabdomyolysis leading to acute kidney injury (AKI) was made and the patient was treated accordingly. Following regular haemodialysis, kidney function improved gradually and he was discharged within a week of hospitalization. At this time his serum creatinine concentration was 172 μmol/L, urea 6.0 mmol/L, sodium 140 mmol/L and potassium 3.9 mmol/L.
Two months later on a follow-up visit he had symptoms of myalgia with arthalgia. Laboratory investigations showed: serum creatinine 106 μmol/L, urea 5.7 mmol/L, sodium 137 mmol/L, potassium 3.9 mmol/L and uric acid 17 μmol/L. The uric acid result was rechecked and confirmed as correct on a fresh sample. He was not receiving any uric acid lowering drugs.
To investigate the cause of severe hypouricaemia a fractional excretion of uric acid (FEUA = urinary uric acid × serum creatinine × 100/serum uric acid × urine creatinine) and 24 h urinary uric acid excretion were measured. The FEUA was 151% (reference interval 5–11%) and 24 h urinary uric acid was 2.59 mmol/24 h (reference interval 1.48–4.43 mmol/24 h). Urinary protein loss was normal. The patient also underwent abdominal ultrasound for the presence of renal stones but the findings were normal. A provisional diagnosis of idiopathic renal hypouricaemia was made. To identify any possible genetic origin his brother was screened for serum and urinary uric acid. His serum uric acid was 12 μmol/L with a FEUA of 190% and a normal 24 h urinary uric acid excretion. His brother also gave a history of exercise intolerance with particular difficulty in playing soccer. The patient and his elder brother were then provisionally diagnosed with hereditary renal hypouricaemia (HRH). Ethnically our patient was a Bengali residing in the state of West Bengal, India. Interestingly, there are no published reports of any patient with HRH from India. Unfortunately genetic analysis could not be done in our patients.
Discussion
Rhabdomyolysis is a common condition that can lead to devastating complications, including renal failure and death. It is the break down of muscle fibres resulting in leakage of toxic cellular contents into the systemic circulation .The common clinical manifestations of rhabdomyolysis are hypovolaemia, AKI and hyperkalaemia. 1 The aetiologies may be subdivided into traumatic, exercise-induced, toxicological, environmental, metabolic, infectious, immunological and inherited disorders. 2 Rhabdomyolysis is a common cause of AKI which can occur after excessive, strenuous, unaccustomed activity. Exercise-induced AKI, may present with and without rhabdomyolysis. 3
In our patient, the characteristic history of exercise-induced AKI and muscular pain led us to suspect rhabdomyolysis, which was confirmed by the raised serum creatine kinase activity. 4
showing various laboratory parameters of the patient at admission and two months later during follow-up
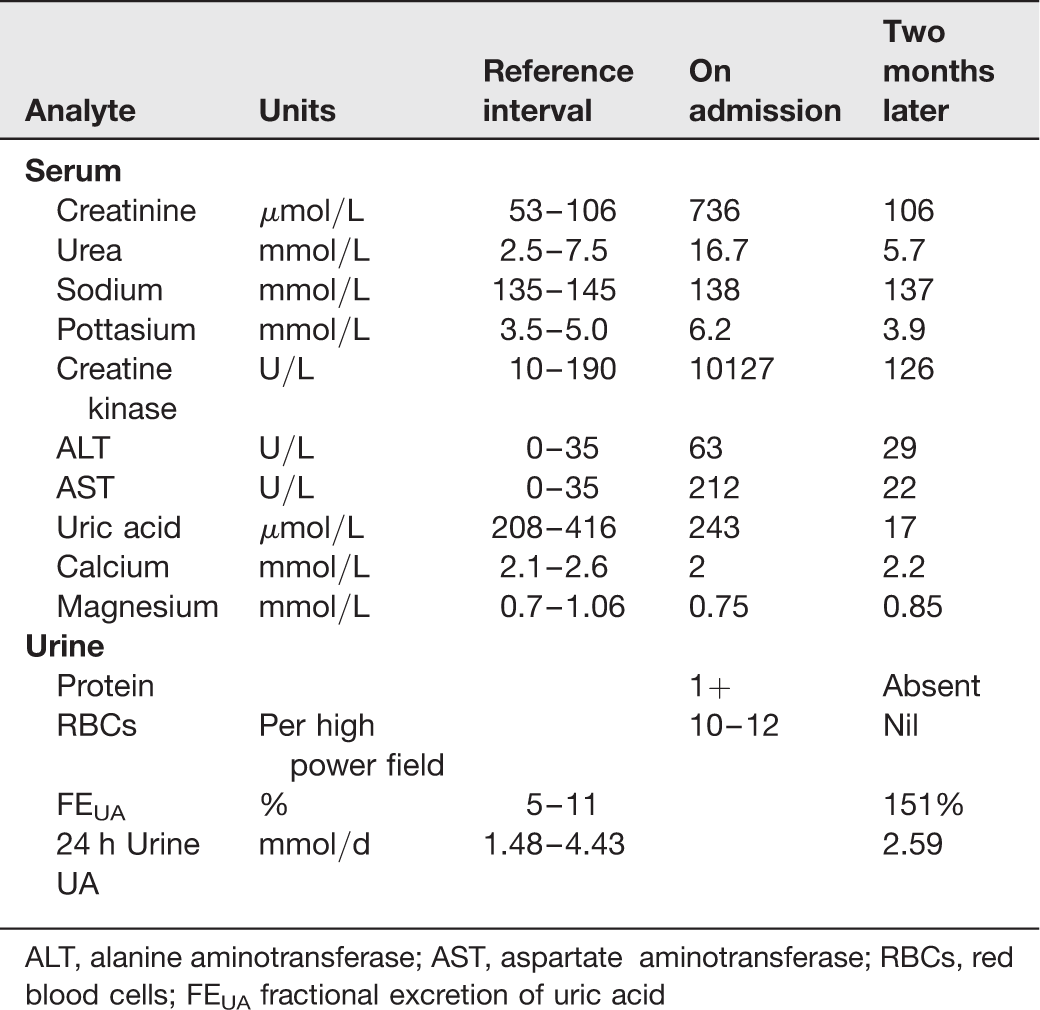
ALT, alanine aminotransferase; AST, aspartate aminotransferase; RBCs, red blood cells; FEUA fractional excretion of uric acid
Renal hypouricaemia is a rare disorder in which there is an isolated defect of tubular uric acid transport leading to profound hypouricaemia along with increased urinary uric acid excretion. This condition is very rare and until now, most cases have been described in the Japanese population with a prevalence rate of 0.12%. 5 Nephrolithiasis and exercise-induced AKI have been associated with renal hypouricaemia. Patients with renal hypouricemia have a 200-fold greater predisposition to exercise-induced AKI than those without renal hypouricemia. 5 Hereditary hypouricaemia complicated by nephrolithiasis and exercise-induced AKI has mainly been reported in Japanese patients with loss-of-function URAT1 mutations transmitted as an autosomal recessive trait. 6 When we screened the patient's brother we found that he too had severe hypouricaemia with very high urinary uric acid excretion: genetic analysis was not done. He also gave a history of muscular pain after exercise but there was no previous history of AKI.
The diagnosis of HRH may be missed in patients who present with exercise-induced AKI since their serum uric acid concentrations may be normal at the time of presentation.
Uric acid is the most abundant aqueous antioxidant. It assists in the preservation of endothelial dilation during oxidative stress and plays a vital role by scavenging oxygen free radicals. Hypouricaemia among patients with HRH may predispose them to ischaemic AKI compounded by exercise-induced renal vasoconstriction and excessive production of free radicals in the renal tubules.7,8 Ohta et al. 9 identified that HRH has a high male preponderance and suggested that antioxidant properties of oestrogen might be protective in females. Exercise intolerance is probably one of the clinical symptoms of HRH. Both the patient and his brother were treated with vitamin C (500 mg) and vitamin E (200 IU) daily. It has been suggested by Ming et al. 3 that HRH is a cause of non-rhabdomyolysis presenting exercise-induced AKI but our case is inconsistent with this view and has shown that HRH can also present with rhabdomyolysis. We believe this to be the first description of a case of HRH presenting with rhabdomyolysis.