
Abstract
Background
Comparability of cholesterol measurement is clinically required and external quality assurance (EQA) programmes are important to verify the trueness of routine methods.
Methods
We developed a gas chromatography-isotope dilution mass spectrometry (GC-IDMS) total cholesterol assay to investigate the cause of a suspected matrix-related negative bias with the Beckman Coulter enzymatic method discovered in an EQA programme. The GC-IDMS method was calibrated with certified reference material and verified against a secondary reference method. Bias between the GC-IDMS and Beckman Coulter methods was estimated according to Clinical and Laboratory Standards Institute (CLSI) protocol EP9-A2 with 40 clinical samples.
Results
At clinically important decision levels, no significant bias was demonstrated on patients' samples (all results within a ±3% limit). A matrix effect confined to the EQA material that affected the Beckman Coulter total cholesterol method was confirmed.
Conclusions
The GC-IDMS method is suitable as a higher order total cholesterol method in a routine clinical laboratory. Matrix effects defeat the objectives of EQA schemes by preventing the verification of trueness. Given the importance of obtaining a true cholesterol result without systematic error, we recommend that EQA material without matrix effects should be used.
Introduction
True and precise serum total and LDL cholesterol measurement is pivotal in establishing coronary heart disease risk and monitoring treatment for individual patients with access to therapeutic intervention. Reimbursement of health-care providers in some health-care systems is also dependent on achieving specific target values as set out in guidelines. 1–4 To meet these challenges, the laboratory standardization panel of the National Cholesterol Education Program recommended a total precision target of ≤3% and a bias of ±3% for clinical laboratory cholesterol methods with patients' samples. 1
Target values published in clinical guidelines can be traced to the Centers for Disease Control and the Cholesterol Reference Method Laboratory Network (CRMLN) secondary reference method procedures (RMP). 5 Until recently, the secondary RMP was a modification of the Abell–Levy–Brodie–Kendall method, but this method is being replaced by gas chromatography-isotope dilution mass spectrometry (GC-IDMS) which is generally accepted as the highest order analytical procedure with high analyte specificity and selectivity. 6 Comparability of a routine laboratory cholesterol measurement depends on the traceability of patient results via a hierarchy of transfer protocols from the manufacturer's calibrators, certified reference materials (CRM), secondary RMP to a definitive RMP based on GC-IDMS.
External quality assessment (EQA) programmes with target values traceable to a RMP are therefore important to verify trueness of routine methods and the comparability of patient results. EQA programmes for cholesterol have historically been plagued by manufacturer-specific matrix effects. 4,7–10 Matrix effects are properties unique to calibrators and control material that arise in the manufacturing process when biological materials such as serum are lyophilized or otherwise modified.
Our laboratory network, all of which use the same Beckman Coulter method, participates in the Royal College of Pathologists of Australasia Quality Assurance Programme (RCPA QAP), and has noted a persistent negative bias with cholesterol, raising the question whether a true bias affecting patient results was present or whether this was an artefact of the material when using this method (matrix effect): a slope of 0.92 and an intercept of −0.021 mmol/L with an average negative bias of 0.365 mmol/L were reported for cycle 83 of the RCPA QAP General Chemistry programme in 2010. A similar bias was also seen in the RCPA QAP Special Lipids programme in 2010. From the end-of-cycle summary report, it also appeared as if this phenomenon affected all Beckman Coulter users as well as some method groups from other manufacturers. A patient sample exchange programme with laboratories using alternative instrument and reagent manufacturers suggested a matrix effect of the EQA material, but this approach was unsatisfactory to verify trueness and comparability.
To address these issues, we developed a GC-IDMS method suitable for a modern clinical laboratory and traceable to the primary RMP. We used the GC-IDMS method to analyse clinical samples and EQA material to investigate the cause of the observed bias.
Methods
Samples
Fresh serum, selected to cover the analytical range of interest, was collected from excess samples after completion of routine analyses and stored at −20°C until analysis. Stored aliquots from the RCPA QAP cycle 38 for Special Lipids and cycle 83 for General Chemistry (2010) were analysed in parallel on both the Beckman Coulter and GC-IDMS assays. Comparison samples were analysed in a single run.
Materials
Reagents were of analytical reagent grade. Cholesterol (99% purity) was obtained from Sigma-Aldrich (St Louis, MO, USA) and D6 Cholesterol (97–98% isotopic purity) was obtained from Cambridge Isotopes Laboratories (Andover, MA, USA). CRM was obtained from the Reference Material Institute for Clinical Chemistry Standards (Kanagawa-ken, Japan;
Aliquots of patient serum samples stored at −20°C and shipped on dry ice were analysed by the University of Washington, Department of Medicine, Northwest Lipid Research Laboratories (NWLRL) (Seattle, WA, USA), a CRMLN laboratory, with the Abell–Levy–Brodie–Kendall method.
Analytical methods
Routine serum cholesterol was measured on a Beckman Coulter DxC800 analyser with an enzymatic cholesterol oxidase/peroxidase method according to the manufacturer's instructions (Beckman Coulter Diagnostics, Brea, CA, USA; PN467825). The package insert for the Beckman Coulter Multi-Calibrator (PN442600) claimed traceability to NIST 911b.
The GC-IDMS total cholesterol assay was a modification of our routine 7-dehydrocholesterol method and is similar to other published total cholesterol methods with some modifications which are briefly described below. 6,11 Serum (20 μL) was saponified with 40% potassium hydroxide (100 μL) at 60°C for 60 min and was extracted with hexane after addition of saturated sodium chloride. The hexane layer was collected after centrifugation, evaporated to dryness over nitrogen and reconstituted in n-propanol (150 μL) prior to analysis in an underivatized form (e.g. non-silylated). A Shimadzu QP2010 plus GCMS system (Shimadzu USA Manufacturing Inc., Canby, OR, USA) was used in electron impact ionization scan mode (300–400 amu). Reconstituted sample extract (1 μL) was injected in split mode (25:1 split) using a DB5-MS (5% phenylmethylpolysiloxane) capillary column (15 m by 0.25 mm film by 0.25 mm internal diameter; Agilent Technologies, Inc., Santa Clara, CA, USA). A calibration curve was prepared from secondary cholesterol calibrators in ethanol over the concentration range 1.0–10.0 mmol/L with 2.5 mmol/L D6 cholesterol internal standard. Results were calculated from the ion peak area ratios (m/z 386–392) after fitting a quadratic regression equation (R 2 = 0.9996). The assigned values of the calibrators were adjusted after analysis of JCCRM 223–225 and JCCRM 211–213. Analysis was performed in duplicate.
Statistics
Bias was estimated according to Clinical and Laboratory Standards Institute (CLSI) protocol EP9-A2 using Microsoft Excel software (Microsoft Corporation, Redmond, WA, USA). 12
Results
The GC-IDMS cholesterol calibrators required only minor adjustment to align with the CRM values (slope 1.02, intercept 0.19 mmol/L). The repeatability of the GC-IDMS assay was 3.6% at 3.2 mmol/L, 2.5% at 4.8 mmol/L and 2.1% at 6.9 mmol/L compared with 0.8% with the Beckman Coulter assay across the measuring range. The total analytical time required for a batch of 40 samples was approximately eight hours with a chromatography time of 11 min per sample.
Total serum cholesterol bias estimation with clinical samples
The bias estimation was performed according to the CLSI EP9-A2 protocol. The Beckman Coulter and GC-IDMS methods were compared with the Northwest Lipid Research Laboratory (NWLRL), a member of the Cholesterol Reference Method Laboratory Network, using 10 patients' samples. The Beckman Coulter and GC-IDMS methods were subsequently compared with an additional 40 clinical samples. Acceptable bias was taken as ±3% of the target value. All results are reported in mmol/L. % bias was calculated using non-rounded values, and the tabulated results have been rounded to two decimal places. GC-IDMS, gas chromatography-isotope dilution mass spectrometry
An extended comparison of the Beckman Coulter assay against the validated GC-IDMS assay confirmed the absence of a significant bias with 40 clinical samples (Table 1). The comparison of total cholesterol in clinical samples and RCPA QAP samples assayed by GC-IDMS and Beckman Coulter are presented in Figure 1. The apparent negative bias of the Beckman Coulter assay was confined to the RCPA QAP material and was not evident with clinical samples, and we therefore concluded that this was indicative of a matrix effect confined to the RCPA QAP material.
Comparison of GC-IDMS and Beckman Coulter total cholesterol methods. Passing–Bablok regression yielded the following results (95% CI): clinical samples (n = 40), Beckman Coulter offset −0.279 (−0.433 to −0.181) and slope 1.070 (1.042–1.106); RCPA QAP (n = 11), Beckman Coulter offset −0.090 (−0.367 to 0.128) and slope 0.889 (0.842 to 0.946). GC-IDMS, gas chromatography-isotope dilution mass spectrometry; RCPA QAP, Royal College of Pathologists of Australasia Quality Assurance Programme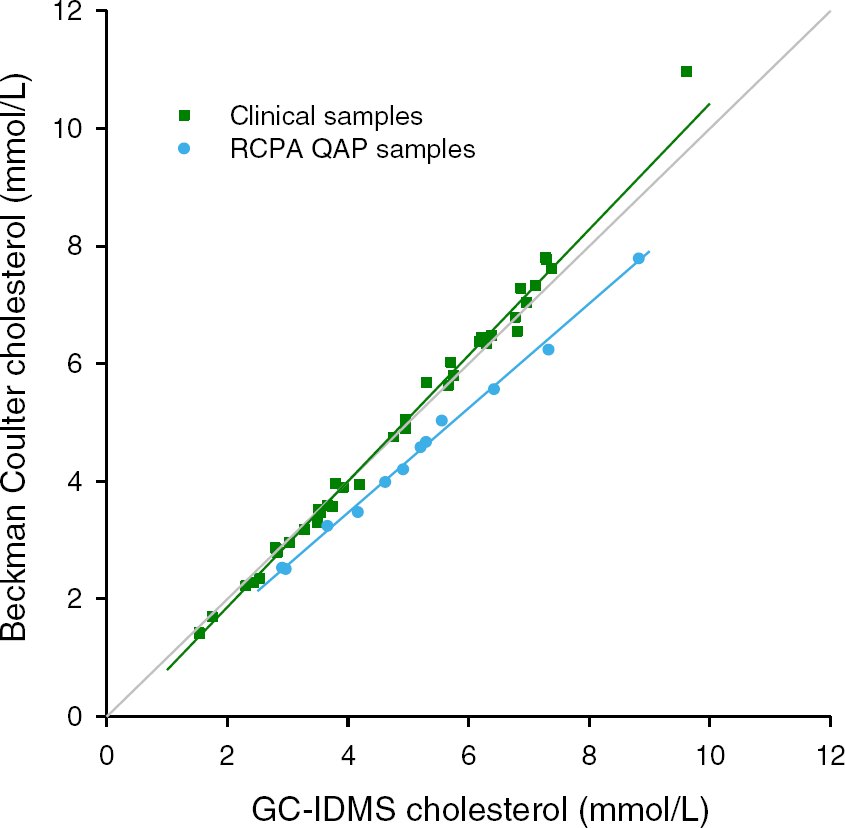
Discussion
We have developed a simplified GC-IDMS total cholesterol assay that is suitable as a higher order field method. The GC-IDMS was calibrated against CRM and the trueness of the GC-IDMS and Beckman Coulter enzymatic methods were validated by comparison of clinical samples assayed by a CRMLN laboratory. We have demonstrated a matrix effect in the EQA material that affects the Beckman Coulter enzymatic method. Given the minimal bias and excellent precision observed with an average repeatability of 0.8% and a long-term total precision of 2.5%, the Beckman Coulter enzymatic total cholesterol assay surpassed analytical requirements.
The small negative bias of the GC-IDMS method relative to CRMLN results may be explained by methodological differences such as variation in the purity of chemicals or the accuracy of weighing when preparing calibrators, the use of D6-cholesterol as opposed to 13C2- or 13C3-cholesterol internal standards and the fact that our method did not employ a derivatization step. The Abell–Levy–Brodie–Kendall method is also known to exhibit a small positive bias due to non-specific chromogen interference when compared with the GC-IDMS primary reference method and this was also described for the proposed new secondary GC-IDMS reference method. 6 The GC-IDMS method we described meets the requirement of a bias of ±3% and is suitable as a higher order analytical method for a modern clinical laboratory and provides convenient evidence of traceability to certified reference methods and materials. The relatively low precision of this method compared with that achieved by an automated enzymatic method will, however, require replicate analyses. Investigation of analytical specificity and precision over a longer time period needs to be performed before a general recommendation on the wider application of the GC-IDMS method can be made. We will use the method to investigate problematic clinical samples and to periodically verify the trueness of our routine total cholesterol assay.
Matrix effects defeat some objectives of an EQA scheme by preventing the verification of trueness by an individual laboratory and monitoring standardization across laboratories. 10 Sample exchange between routine laboratories employing alternative enzymatic cholesterol methods is an unsatisfactory alternative as it is a tenuous assumption that the comparative method itself is correct, and some method groups exhibited an even more pronounced bias than the Beckman Coulter method group on the RCPA QAP. Comparison with the post hoc method peer group means in an EQA programme similarly adds little additional information as the trueness of the whole group may be affected.
One possible solution is to periodically validate the trueness against a method employing a different analytical principle that has itself been validated as we have described here. The simplest solution from a clinical laboratory perspective would be to use quality control materials devoid of matrix effects in an EQA programme. 10 A rigorous protocol has been described to prepare commutable quality control material for total cholesterol, triglyceride and HDL cholesterol from fresh serum, and the JCCRM 223–225 material we obtained was indeed prepared according to this protocol. 13 Given the importance of obtaining a true cholesterol result, we recommend that EQA programmes use material free from matrix effects. If no practical alternative is available, formal method-specific target values should be established by the EQA supplier.
DECLARATIONS